Atqua Sultan 1 , Faisal Shamim 2 , Saima Rashid 3
Authors affiliations:
HTGP, or hypertriglyceridemia-induced pancreatitis, is an uncommon but important cause of acute pancreatitis that is frequently linked to metabolic diseases, including obesity and diabetes mellitus. We describe the case of a 47-year-old woman who had a history of hypertension, diabetes, and hypercholesterolemia. She developed severe HTGP, which was further complicated by portal vein thrombosis and diabetic ketoacidosis (DKA). She was initially treated for DKA after being admitted with severe gastric discomfort and metabolic acidosis. However, HTGP was diagnosed due to consistently high triglyceride values (1426 mg/dL). Imaging revealed vascular problems and relatively severe pancreatitis. Following treatment with insulin, fibrate medication, and anticoagulation, the patient's triglycerides significantly decreased and their clinical condition improved. This case emphasizes the significance of early detection and focused treatment in HTGP as well as the diagnostic difficulties presented by overlapping metabolic disorders. Treatment is made more difficult by the interaction of DKA and HTGP, which calls for a multidisciplinary strategy. Our case example adds to the increasing amount of research highlighting the necessity of tailored lipid-lowering plans and careful metabolic monitoring in order to avoid recurrence and enhance patient outcomes.
Keywords: Hypertriglyceridemia, Acute Pancreatitis, Diabetic Ketoacidosis, Insulin Infusion, Fibrate Therapy
Citation: Sultan A, Shamim F, Rashid S. Hypertriglyceridemia as a rare cause of acute pancreatitis: A case report, Anaesth. pain intensive care 2025;29(9):1313-16. DOI: 10.35975/apic.v29i9.3072
Received: November 25, 2025; Revised: November 26, 2025; Accepted: November 30, 2025
Acute pancreatitis (AP) is a potentially fatal inflammatory illness of the pancreas that varies in severity from mild to severe necrotizing disease. While gallstones and alcohol remain the most common etiologies, hypertriglyceridemia (HTG) has emerged as an increasingly recognized cause of acute pancreatitis, responsible for approximately 1–10% of cases globally, depending on population and diagnostic thresholds.1,2
Hypertriglyceridemia-induced pancreatitis (HTGP) generally occurs when serum triglyceride levels exceed 1000 mg/dL, although lower levels may also be implicated in genetically or metabolically predisposed individuals.2,3 The underlying mechanism involves chylomicron-mediated plugging of pancreatic capillaries, resulting in ischemia and the release of toxic free fatty acids following lipase activity, which leads to acinar cell injury and inflammation.3,4 Patients with diabetes mellitus, obesity, or familial lipid disorders are particularly susceptible.
Given the rising incidence of obesity, diabetes, and metabolic syndrome, awareness of HTGP as a distinct clinical entity is increasingly important. Early recognition, timely metabolic control, and a multidisciplinary management strategy can significantly improve outcomes and prevent recurrence. The present case contributes to the growing body of literature emphasizing the overlap between DKA and HTGP and highlights the importance of individualized, evidence-based management to optimize patient recovery.
This case report describes a rare example of acute pancreatitis caused by HTGP in a severely ill patient who was hospitalized to the surgical intensive care unit (SICU). We review the diagnostic process, management techniques, such as insulin therapy and plasma exchange, and the difficulties in treating this rare but dangerous illness. This paper emphasizes the significance of early detection and customized treatments to enhance patient outcomes by increasing awareness of HTGP.
A 47-year-old woman with a history of hypertension, hypercholesterolemia, and diabetes mellitus arrived at the emergency room after experiencing increasing stomach pain and frequent vomiting for seven days. She had a blood pressure of 118/72 mm Hg, a respiratory rate of 22 breaths per minute, a tachycardia of 132 beats per minute, and an oxygen saturation of 99% on room air when she was admitted. An examination showed discomfort in the right upper quadrant of the abdomen without rebound or guarding. Due to respiratory distress, she was initially placed on noninvasive ventilation; however, as her work of breathing increased and respiratory failure appeared imminent, she was subsequently intubated and transferred to the Surgical Intensive Care Unit for further management.
Arterial blood gas analysis showed metabolic acidosis. Given her clinical presentation, a diabetic ketoacidosis (DKA) protocol was initiated with aggressive insulin therapy and fluid resuscitation. However, her metabolic acidosis persisted, necessitating continuous renal replacement therapy in the intensive care unit. Ultrasonography revealed a heterogeneous, bulky pancreas, consistent with acute pancreatitis, along with an echogenic focus within the portal vein demonstrating absent flow on color Doppler. Additionally, hepatomegaly with fatty infiltration was observed. Contrast-enhanced computed tomography of the abdomen confirmed moderately severe acute pancreatitis with a Balthazar score of 4 and demonstrated thrombosis in the superior mesenteric, splenic, and portal veins.
Laboratory findings were notable for a markedly elevated serum triglyceride level of 1426 mg/dL. Pancreatic enzyme levels were also elevated, with an amylase of 998 IU/L and lipase of 1443 IU/L. Blood glucose and ketone levels were closely monitored in accordance with the DKA protocol. The patient was treated with fibrate infusions to lower triglycerides, in addition to insulin and heparin to address both hyperglycemia and hypertriglyceridemia-induced pancreatitis. Although her initial presentation was consistent with DKA, the lack of response to standard therapy, coupled with the significantly elevated triglyceride levels, led to the diagnosis of hypertriglyceridemia-induced pancreatitis (HTGP).
After four days of intensive care, the patient was successfully extubated and later transferred out of the SICU. At a one-month follow-up after discharge, repeat lipid profiling showed a significant reduction in serum triglycerides to 148 mg/dL.
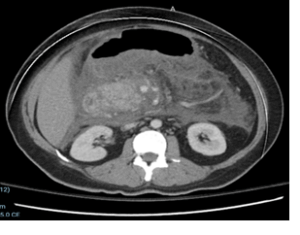
Figure 1: Ultrasonography reveals a heterogeneous, bulky pancreas, consistent with acute pancreatitis, along with an echogenic focus within the portal vein demonstrating absent flow on color Doppler. There is hepatomegaly with fatty infiltration
Hypertriglyceridemia is charcterized by an excess of lipoprotein-transporting macromolecules in the plasma, with levels exceeding the 95th percentile of the reference population.4 It can be classified as primary (familial) or secondary (acquired). Primary is often linked to genetic abnormalities, as categorized by Fredrickson’s classification, whereas secondary Hypertriglyceridemia may be attributed to various acquired conditions, including insulin resistance, hypothyroidism, alcohol consumption, dietary factors, and metabolic disorders. Hypertriglyceridemia-induced pancreatitis (HTGP) accounts for approximately 7% of all cases of acute pancreatitis, making it the third most common cause after gallstones and alcohol consumption. More than 75% of HTGP cases are due to acquired conditions that exacerbate underlying genetic susceptibilities.5
Our patient initially presented with metabolic acidosis and was diagnosed with DKA. Despite standard DKA management, her condition did not improve, leading to the diagnosis of HTGP. Her significantly high triglyceride level (1426 mg/dL) played a significant role in determining that HTGP was the root cause of her pancreatitis. According to the literature, triglyceride levels above 1000 mg/dL are usually what cause acute pancreatitis.6 The data from our patient were in line with this cutoff, highlighting the part hypertriglyceridemia plays in the aetiology of pancreatitis.
Because of its similarities to other causes of acute pancreatitis, HTGP is frequently difficult to diagnose. The possibility of normal or falsely low amylase values in patients with severe hypertriglyceridemia is one of the main diagnostic challenges.7 This happens as a result of elevated fat levels interfering with amylase tests, which results in inaccurate values. According to studies, despite having severe pancreatitis, up to 50% of HTGP patients may have "normal" serum amylase levels.8 Accurate diagnosis is further complicated by fasting-related decreases and postprandial chylomicron increases. In our case, distinguishing HTGP from other possible causes of pancreatitis required a close examination of the patient's lipid profile and clinical presentation.
A unique feature of our case was the co-occurrence of DKA, which itself can exacerbate hypertriglyceridemia. Insulin deficiency in DKA results in defective clearance of very low-density lipoproteins (VLDL) and increased hepatic VLDL production, leading to profound hypertriglyceridemia. While severe hypertriglyceridemia in DKA is rare, it has been documented in prior studies. The bidirectional relationship between HTGP and DKA is significant because pancreatitis can precipitate DKA, and conversely, DKA can cause hypertriglyceridemia. This interplay highlights the importance of monitoring blood glucose and lipid levels in patients presenting with metabolic acidosis and pancreatitis symptoms.9
The pathophysiology of HTGP remains incompletely understood. Current evidence suggests that chylomicrons precipitate within the pancreatic capillaries, leading to ischemia, acinar cell injury, and an inflammatory cascade mediated by free fatty acids released via lipoprotein lipase activity. This mechanism results in pancreatic necrosis and systemic inflammation. Genetic predisposition plays a role in some cases, with mutations in the lipoprotein lipase (LPL) gene being identified in several patients with recurrent HTGP episodes.10 Our patient did not undergo genetic testing, but her history of hyperlipidemia and metabolic syndrome suggests a potential underlying genetic susceptibility.
Management of HTGP requires a two-pronged approach: acute treatment of pancreatitis and long-term prevention of recurrence. Acute management involves aggressive fluid resuscitation, analgesia, and lipid-lowering therapies. While insulin and heparin infusions enhance LPL activity to facilitate triglyceride clearance, the role of plasmapheresis in rapidly reducing chylomicron levels remains debated.11 Some studies advocate for plasmapheresis in cases of severe hypertriglyceridemia (>2000 mg/dL) or refractory pancreatitis, but its routine use is controversial due to variable efficacy and resource constraints.12 In this case, our patient was treated with insulin and fibrate therapy, leading to a significant reduction in triglyceride levels to 148 mg/dL at one-month follow-up.
Long-term management is centered on preventing future HTGP episodes through lifestyle modifications and pharmacological interventions. Dietary changes, including a low-fat, high-fiber diet and omega-3 fatty acid supplementation, are essential. Strict glycemic control is particularly important in patients with diabetes, as insulin therapy plays a crucial role in triglyceride metabolism.13 Our patient was discharged with lipid-lowering medications and dietary counseling, emphasizing the importance of sustained triglyceride management.
In comparison with published literature, this case underscores several critical aspects of HTGP, including the challenges of diagnosis, the interplay between HTGP and DKA, and the need for tailored management strategies. Although earlier research has emphasised the significance of HTGP detection in individuals with metabolic syndrome.14 Our case example contributes to the increasing body of evidence showing that DKA can aggravate the presentation of pancreatitis and considerably increase hypertriglyceridemia. The fact that our patient's condition was successfully resolved using insulin, fibrates, and heparin supports the effectiveness of traditional lipid-lowering techniques in an emergency.
In conclusion, this case emphasises how critical it is to identify HTGP as a unique clinical entity and distinguish it from other causes of pancreatitis. Clinicians should have a strong suspicion for HTGP in patients with considerably raised triglyceride levels, especially those with diabetes or metabolic syndrome. A multidisciplinary strategy combining endocrinologists, gastroenterologists, and critical care experts is required to improve patient outcomes and prevent recurrence.
Authors affiliations:
- Atqua Sultan, Senior Registrar, Department of Anesthesiology, Nishtar Hospital, Multan. Pakistan; Email: me.atqua@gmail.com
- Faisal Shamim, Associate Professor, Department of Anesthesiology, Aga Khan University Hospital, Stadium Road, Karachi, Pakistan; Email: Faisal.shamim@aku.edu
- Saima Rashid, Assistant Professor, Department of Anesthesiology, Aga Khan University Hospital, Stadium Road, Karachi, Pakistan; Email: saima.rashid@aku.edu
ABSTRACT
HTGP, or hypertriglyceridemia-induced pancreatitis, is an uncommon but important cause of acute pancreatitis that is frequently linked to metabolic diseases, including obesity and diabetes mellitus. We describe the case of a 47-year-old woman who had a history of hypertension, diabetes, and hypercholesterolemia. She developed severe HTGP, which was further complicated by portal vein thrombosis and diabetic ketoacidosis (DKA). She was initially treated for DKA after being admitted with severe gastric discomfort and metabolic acidosis. However, HTGP was diagnosed due to consistently high triglyceride values (1426 mg/dL). Imaging revealed vascular problems and relatively severe pancreatitis. Following treatment with insulin, fibrate medication, and anticoagulation, the patient's triglycerides significantly decreased and their clinical condition improved. This case emphasizes the significance of early detection and focused treatment in HTGP as well as the diagnostic difficulties presented by overlapping metabolic disorders. Treatment is made more difficult by the interaction of DKA and HTGP, which calls for a multidisciplinary strategy. Our case example adds to the increasing amount of research highlighting the necessity of tailored lipid-lowering plans and careful metabolic monitoring in order to avoid recurrence and enhance patient outcomes.
Keywords: Hypertriglyceridemia, Acute Pancreatitis, Diabetic Ketoacidosis, Insulin Infusion, Fibrate Therapy
Citation: Sultan A, Shamim F, Rashid S. Hypertriglyceridemia as a rare cause of acute pancreatitis: A case report, Anaesth. pain intensive care 2025;29(9):1313-16. DOI: 10.35975/apic.v29i9.3072
Received: November 25, 2025; Revised: November 26, 2025; Accepted: November 30, 2025
1. INTRODUCTION
Acute pancreatitis (AP) is a potentially fatal inflammatory illness of the pancreas that varies in severity from mild to severe necrotizing disease. While gallstones and alcohol remain the most common etiologies, hypertriglyceridemia (HTG) has emerged as an increasingly recognized cause of acute pancreatitis, responsible for approximately 1–10% of cases globally, depending on population and diagnostic thresholds.1,2
Hypertriglyceridemia-induced pancreatitis (HTGP) generally occurs when serum triglyceride levels exceed 1000 mg/dL, although lower levels may also be implicated in genetically or metabolically predisposed individuals.2,3 The underlying mechanism involves chylomicron-mediated plugging of pancreatic capillaries, resulting in ischemia and the release of toxic free fatty acids following lipase activity, which leads to acinar cell injury and inflammation.3,4 Patients with diabetes mellitus, obesity, or familial lipid disorders are particularly susceptible.
Given the rising incidence of obesity, diabetes, and metabolic syndrome, awareness of HTGP as a distinct clinical entity is increasingly important. Early recognition, timely metabolic control, and a multidisciplinary management strategy can significantly improve outcomes and prevent recurrence. The present case contributes to the growing body of literature emphasizing the overlap between DKA and HTGP and highlights the importance of individualized, evidence-based management to optimize patient recovery.
This case report describes a rare example of acute pancreatitis caused by HTGP in a severely ill patient who was hospitalized to the surgical intensive care unit (SICU). We review the diagnostic process, management techniques, such as insulin therapy and plasma exchange, and the difficulties in treating this rare but dangerous illness. This paper emphasizes the significance of early detection and customized treatments to enhance patient outcomes by increasing awareness of HTGP.
2. CASE REPORT
A 47-year-old woman with a history of hypertension, hypercholesterolemia, and diabetes mellitus arrived at the emergency room after experiencing increasing stomach pain and frequent vomiting for seven days. She had a blood pressure of 118/72 mm Hg, a respiratory rate of 22 breaths per minute, a tachycardia of 132 beats per minute, and an oxygen saturation of 99% on room air when she was admitted. An examination showed discomfort in the right upper quadrant of the abdomen without rebound or guarding. Due to respiratory distress, she was initially placed on noninvasive ventilation; however, as her work of breathing increased and respiratory failure appeared imminent, she was subsequently intubated and transferred to the Surgical Intensive Care Unit for further management.
Arterial blood gas analysis showed metabolic acidosis. Given her clinical presentation, a diabetic ketoacidosis (DKA) protocol was initiated with aggressive insulin therapy and fluid resuscitation. However, her metabolic acidosis persisted, necessitating continuous renal replacement therapy in the intensive care unit. Ultrasonography revealed a heterogeneous, bulky pancreas, consistent with acute pancreatitis, along with an echogenic focus within the portal vein demonstrating absent flow on color Doppler. Additionally, hepatomegaly with fatty infiltration was observed. Contrast-enhanced computed tomography of the abdomen confirmed moderately severe acute pancreatitis with a Balthazar score of 4 and demonstrated thrombosis in the superior mesenteric, splenic, and portal veins.
Laboratory findings were notable for a markedly elevated serum triglyceride level of 1426 mg/dL. Pancreatic enzyme levels were also elevated, with an amylase of 998 IU/L and lipase of 1443 IU/L. Blood glucose and ketone levels were closely monitored in accordance with the DKA protocol. The patient was treated with fibrate infusions to lower triglycerides, in addition to insulin and heparin to address both hyperglycemia and hypertriglyceridemia-induced pancreatitis. Although her initial presentation was consistent with DKA, the lack of response to standard therapy, coupled with the significantly elevated triglyceride levels, led to the diagnosis of hypertriglyceridemia-induced pancreatitis (HTGP).
After four days of intensive care, the patient was successfully extubated and later transferred out of the SICU. At a one-month follow-up after discharge, repeat lipid profiling showed a significant reduction in serum triglycerides to 148 mg/dL.
Figure 1: Ultrasonography reveals a heterogeneous, bulky pancreas, consistent with acute pancreatitis, along with an echogenic focus within the portal vein demonstrating absent flow on color Doppler. There is hepatomegaly with fatty infiltration
3. DISCUSSION
Hypertriglyceridemia is charcterized by an excess of lipoprotein-transporting macromolecules in the plasma, with levels exceeding the 95th percentile of the reference population.4 It can be classified as primary (familial) or secondary (acquired). Primary is often linked to genetic abnormalities, as categorized by Fredrickson’s classification, whereas secondary Hypertriglyceridemia may be attributed to various acquired conditions, including insulin resistance, hypothyroidism, alcohol consumption, dietary factors, and metabolic disorders. Hypertriglyceridemia-induced pancreatitis (HTGP) accounts for approximately 7% of all cases of acute pancreatitis, making it the third most common cause after gallstones and alcohol consumption. More than 75% of HTGP cases are due to acquired conditions that exacerbate underlying genetic susceptibilities.5
Our patient initially presented with metabolic acidosis and was diagnosed with DKA. Despite standard DKA management, her condition did not improve, leading to the diagnosis of HTGP. Her significantly high triglyceride level (1426 mg/dL) played a significant role in determining that HTGP was the root cause of her pancreatitis. According to the literature, triglyceride levels above 1000 mg/dL are usually what cause acute pancreatitis.6 The data from our patient were in line with this cutoff, highlighting the part hypertriglyceridemia plays in the aetiology of pancreatitis.
Because of its similarities to other causes of acute pancreatitis, HTGP is frequently difficult to diagnose. The possibility of normal or falsely low amylase values in patients with severe hypertriglyceridemia is one of the main diagnostic challenges.7 This happens as a result of elevated fat levels interfering with amylase tests, which results in inaccurate values. According to studies, despite having severe pancreatitis, up to 50% of HTGP patients may have "normal" serum amylase levels.8 Accurate diagnosis is further complicated by fasting-related decreases and postprandial chylomicron increases. In our case, distinguishing HTGP from other possible causes of pancreatitis required a close examination of the patient's lipid profile and clinical presentation.
A unique feature of our case was the co-occurrence of DKA, which itself can exacerbate hypertriglyceridemia. Insulin deficiency in DKA results in defective clearance of very low-density lipoproteins (VLDL) and increased hepatic VLDL production, leading to profound hypertriglyceridemia. While severe hypertriglyceridemia in DKA is rare, it has been documented in prior studies. The bidirectional relationship between HTGP and DKA is significant because pancreatitis can precipitate DKA, and conversely, DKA can cause hypertriglyceridemia. This interplay highlights the importance of monitoring blood glucose and lipid levels in patients presenting with metabolic acidosis and pancreatitis symptoms.9
The pathophysiology of HTGP remains incompletely understood. Current evidence suggests that chylomicrons precipitate within the pancreatic capillaries, leading to ischemia, acinar cell injury, and an inflammatory cascade mediated by free fatty acids released via lipoprotein lipase activity. This mechanism results in pancreatic necrosis and systemic inflammation. Genetic predisposition plays a role in some cases, with mutations in the lipoprotein lipase (LPL) gene being identified in several patients with recurrent HTGP episodes.10 Our patient did not undergo genetic testing, but her history of hyperlipidemia and metabolic syndrome suggests a potential underlying genetic susceptibility.
Management of HTGP requires a two-pronged approach: acute treatment of pancreatitis and long-term prevention of recurrence. Acute management involves aggressive fluid resuscitation, analgesia, and lipid-lowering therapies. While insulin and heparin infusions enhance LPL activity to facilitate triglyceride clearance, the role of plasmapheresis in rapidly reducing chylomicron levels remains debated.11 Some studies advocate for plasmapheresis in cases of severe hypertriglyceridemia (>2000 mg/dL) or refractory pancreatitis, but its routine use is controversial due to variable efficacy and resource constraints.12 In this case, our patient was treated with insulin and fibrate therapy, leading to a significant reduction in triglyceride levels to 148 mg/dL at one-month follow-up.
Long-term management is centered on preventing future HTGP episodes through lifestyle modifications and pharmacological interventions. Dietary changes, including a low-fat, high-fiber diet and omega-3 fatty acid supplementation, are essential. Strict glycemic control is particularly important in patients with diabetes, as insulin therapy plays a crucial role in triglyceride metabolism.13 Our patient was discharged with lipid-lowering medications and dietary counseling, emphasizing the importance of sustained triglyceride management.
In comparison with published literature, this case underscores several critical aspects of HTGP, including the challenges of diagnosis, the interplay between HTGP and DKA, and the need for tailored management strategies. Although earlier research has emphasised the significance of HTGP detection in individuals with metabolic syndrome.14 Our case example contributes to the increasing body of evidence showing that DKA can aggravate the presentation of pancreatitis and considerably increase hypertriglyceridemia. The fact that our patient's condition was successfully resolved using insulin, fibrates, and heparin supports the effectiveness of traditional lipid-lowering techniques in an emergency.
4. CONCLUSION
In conclusion, this case emphasises how critical it is to identify HTGP as a unique clinical entity and distinguish it from other causes of pancreatitis. Clinicians should have a strong suspicion for HTGP in patients with considerably raised triglyceride levels, especially those with diabetes or metabolic syndrome. A multidisciplinary strategy combining endocrinologists, gastroenterologists, and critical care experts is required to improve patient outcomes and prevent recurrence.
- Ethical Considerations
- Conflict of Interest
- Funding
- Author contribution
9. REFERENCES
- Gapp J, Tariq A, Chandra S. Acute Pancreatitis. [Updated 2023 Feb 9]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan.
- de Pretis N, Amodio A, Frulloni L. Hypertriglyceridemic pancreatitis: Epidemiology, pathophysiology and clinical management. United European Gastroenterol J. 2018 Jun;6(5):649-655.
- Leppäniemi, A., Tolonen, M., Tarasconi, A. et al. 2019 WSES guidelines for the management of severe acute pancreatitis. World J Emerg Surg 14, 27 (2019).
- Subramanian S. Hypertriglyceridemia: Pathophysiology, Role of Genetics, Consequences, and Treatment. [Updated 2024 Jan 8]. In: Feingold KR, Anawalt B, Blackman MR, et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-
- Fredrickson DS. An international classification of hyperlipidemias and hyperlipoproteinemias. Ann Intern Med. 1971;75:471–2.
- Aryal MR, Mainali NR, Gupta S, Singla M. Acute pancreatitis owing to very high triglyceride levels treated with insulin and heparin infusion. BMJ Case Rep. 2013 Apr 22;2013:bcr2013008550.
- Melnick S, Nazir S, Gish D, Aryal MR. Hypertriglyceridemic pancreatitis associated with confounding laboratory abnormalities. J Community Hosp Intern Med Perspect. 2016 Jul 6;6(3):31808.
- Du AV, Pahomeanu MR, Ghiță AI, Constantinescu DI, Grigore DG, Bota AD et al. Hypertriglyceridemia-Induced Acute Pancreatitis-The Milky Way Constellation-The Seven-Year Experience of a Large Tertiary Centre. Diagnostics (Basel). 2024 May 26;14(11):1105.
- Kota SK, Kota SK, Jammula S, et al. Hypertriglyceridemia-induced recurrent acute pancreatitis: a case-based review. Indian J Endocrinol Metab. 2012;16:141–3.
- Tiperneni R, Padappayil RP, Mohan G, Patton C. Diabetic Ketoacidosis and Hypertriglyceridemiainduced Pancreatitis: Can the Perfect Storm Happen Twice? J Community Hosp Intern Med Perspect. 2022 Jul 4;12(4):85-88
- Hidalgo, N.J., Pando, E., Alberti, P. et al. The role of high serum triglyceride levels on pancreatic necrosis development and related complications. BMC Gastroenterol 23, 51 (2023). https://doi.org/10.1186/s12876-023-02684-9
- Gligorijevic N, Stefanovic-Racic M, Kershaw EE. Medical management of hypertriglyceridemia in pancreatitis. Curr Opin Gastroenterol. 2023 Sep 1;39(5):421-427.
- Shaka H, El-Amir Z, Jamil A, Kwei-Nsoro R, Wani F, Dahiya DS, Kichloo A, Amblee A. Plasmapheresis in hypertriglyceridemia-induced acute pancreatitis. Proc (Bayl Univ Med Cent). 2022 11;35(6):768-772.
- Gupta M, Liti B, Barrett C, Thompson PD, Fernandez AB. Prevention and Management of Hypertriglyceridemia-Induced Acute Pancreatitis During Pregnancy: A Systematic Review. Am J Med. 2022 Jun;135(6):709-714.