Urooj Faisal 1 , Marium Noor 2 , Anwarul Haque3
Authors affiliations:
Background & objective: Accurate completion of Death Certificate (DC) is vital information of health statistics. Limited data is available on pediatric death certificates especially from Pakistan. The rationale of this study was to evaluate the accuracy and completeness of DC issued from a pediatric intensive care unit (PICU).
Methodology: A descriptive cross-sectional study was conducted in PICU of new public-sector pediatric in Karachi from January to June 2023. All deaths in children (1 month -15 years) occurred in PICU from medical illnesses and DCs were prepared by junior doctors. A total of 163 DCs were reviewed for major and minor errors in cause of death according to WHO international standards.
Results: Of 163 DCs, none were error-free. The total number of errors was 499 and mean number of errors was 3.06 per patient. The major errors were 306 and most common was mechanism of death reported as cardiopulmonary arrest as underlying cause of death (98.8%), minor errors were 193 and most common was the absence of time interval (100%).
Conclusion: Very high rate of errors was observed in death certificates from a pediatric intensive care unit. Educational interventions are urgently needed with follow-up study.
Abbreviations: COD: cause of death, DC: Death Certificate, MCCD: Medical Certificate of Cause of Death PICU: pediatric intensive care unit,
Keywords: Death certificate, Errors, Major and minor, Children, Cause of death
Citation: Faisal U, Noor M, Haque A. Critical analysis of death certificates issued by a public sector pediatric intensive care unit in Pakistan. Anaesth. pain intensive care 2025;29(9):1279-83. DOI: 10.35975/apic.v29i9.3065
Received: June 13, 2025; Revised: November 13, 2024; Accepted: December 23, 2025
The Medical Certificate of Cause of Death (MCCD) is commonly called the Death certificate (DC), which is a permanent medico-legal document of individual’s death.1 It provides detailed information about an individual’s cause of death and his/her demographic characteristics.2 DC has a very important role in health statistics that can be used for research purposes, planning health policies and resource management.3 Reporting accurate and complete data in DC is a key element in evaluation of health information system.
A fundamental issue in DC is inaccurate and inadequate reporting on cause of death (COD) of individual, which leads to erroneous health statistics, especially in children from low- and middle-income countries. Mortality rate of children, especially under-five is very high in developing countries.4 The inaccurate reporting COD in children leads to a major challenge in epidemiological data. Studies have shown that the reporting of COD in DC is very poor worldwide with errors reporting from 20-100%.5-7 The World Health Organization (WHO) recommends the standard reporting the COD based on the International Classification of Diseases (ICD-10) classification of diseases. The ICD plays a crucial role in mortality statistics and analysis in standardization of cause of death reporting, facilitates international health monitoring and research, and contributes to efforts aimed at improving health outcomes and reducing mortality globally.8
The current form of DC was updated last in 2016, after more than 50 years as shown in Figure 1.
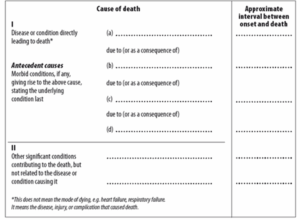
Figure 1: International Form of Medical Certificate of Cause of Death.
It has two parts: Part 1 is used to record sequence of events leading to death as immediate COD then intermediate COD and last one should be underlying COD, and Part 2 is used to record other significant conditions contributing to death.9 The COD is a chain of events like Acute Myocarditis leads to cardiogenic shock and terminal event was “cardiac arrest”, which is mechanism of death and not cause of death.
Several reports have been published on accuracy of DC worldwide.6 Errors in death certificates (DCE), especially from pediatric critical care units are rarely reported.10 The rationale of this study was to evaluate the accuracy and completeness of DC issued from a pediatric intensive care unit of a newly established public-sector Children’s Hospital, Korangi. The objective of this study is to assess the frequency and types of errors in preparing DC by a physician.
A descriptive and cross-sectional study was conducted to evaluate all DCs of children aged 1-month to 15-years admitted in the pediatric intensive care unit (PICU) of Sindh Institute of Child Health & Neonatology (SICHN) Korangi, Karachi over a six-month period from January 1 to June 30, 2023. The study was approved by the institutional Ethical Review Committee (SICHN/Ex-004/2024 September 25,2023). SICHN is a pediatric health-initiative by the Sindh Government of Pakistan, providing high-quality medical care free of cost to critically ill children all over Sindh. SICHN Korangi is a 200-beded tertiary care teaching hospital located in a very low socio-economic area of metropolis city of Karachi and serving a population of more than 2.5 million.
The Pediatric Intensive Care Unit (PICU) at SICHN is a closed multi-disciplinary unit that provides critical care services to children suffering from life-threatening conditions. The 28-bedded PICU has all 4-S components. All deaths in the study period that occurred and for which death certificates and medical records were available were included. We retrospectively reviewed the medical records of eligible patients and collected the following data into a structured data collection sheet including: age, gender, admitting diagnosis, co-morbidity and details of death certificate based on format of WHO-MCCD. We included only natural deaths occurred in PICU during study period and excluded unnatural deaths. The medical officers or pediatric resident-trainees prepared all DCs. Errors were divided into major and minor errors according to the criteria described in the previous studies and were described in Table 1.11
All data entered into Microsoft Excel 2010. Data was presented as number and percentages either as means with standard deviation or median with range. Descriptive statistics were applied for analysis by using simple mathematical calculation. The estimated sample size for this study is 151 if prevalence of 89% errors in pediatric death certificate with a 95% confidence interval and 5% margin of error.10 After adding 10% drop out; then final cohort size is 166. Convenient sampling was taken. The primary outcome of this study was to assess the frequency and types of errors in DCs.
During the study period, 288 (15.1% of admission) death certificates were issued, consecutive 166 DCs were reviewed and three were excluded due to non-availability of DC from electronic medical records. Patients’ characteristics were shown in Table 2. Disease classification according to 1CD 10 is given in Figure 2. No DC was error-free. The total numbers of errors were 499 in 163 DCs. The major and minor errors in DCs were 294 and 185 respectively.
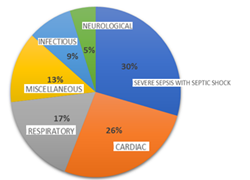
Figure 2: Classification of diseases according to ICD 10
The characteristics of errors in DC are shown in Table 3. Frequencies of major errors are given in Figure 3.
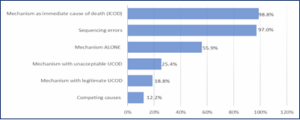
Figure 3: Frequencies of major errors.
The mean number of errors was 3.06 per patient. The most common major error was reporting mechanism of death as the immediate cause of death (ICOD). The cardiopulmonary arrest was alone documented as Underlying Cause of Death (UCOD) in 161 DCs (98.8%). 97% (158) DCs had improper sequencing.
Compared to major error, there was a smaller number of minor errors in DCs. There was no abbreviation used in DCs of our cohort. There were 100 % lack of documenting timeline and Other Significant Conditions (OSC) in all DCs.
The accuracy and appropriate completeness of death certificate is paramount for mortality statistics and public health surveillance. We found a very high rate of errors (100%) in DCs and almost ≥3 errors per DC. Previously; the errors in DCs have been described in various categories and grades of severity of errors in published literature. For last one decade, reporting of errors in DCs was categorized as “major errors” and “minor errors” with few sub-headings with simple and clear explanation to create a better standardization.6 We compared our results with similar studies and observations were similar too. Gupta et al observed 89% errors in 1251 DCs of children with ratio of almost one error per patient.10 Atreya et al reported mechanism of death as ICOD in 78% of their evaluation of errors in DC from hospital-based study from Nepal.5 Qaddumi et al (2017) found almost 45% as a major error in reporting underlying cause of death in a descriptive report from Palestine.12 Haque et al also reported 200 errors in 202 DCs of adult patients (almost one error per DC) from a tertiary-care teaching hospital of Pakistan.13 Errors in DCs is very common worldwide with range from 20%-100%.6,7 Most of reports are hospital-based on DCE as well as COD worldwide. There are available two systemic reviews and meta-analysis on DCE and COD.5,14. However, there were few pediatric reports and two reports from adult ICU.15,16
We have 306 (61.3%) major errors and 193 (38.7%) minor errors in our cohort. The numbers of major and minor errors per DC were 0.6 and 0.4 respectively. Both multiple and mixed errors were common like in other reports. The most common major error in our cohort was reporting mechanism of death as ICOD (98.8%). Most of DCE occurred in underlying and immediate COD worldwide.17,18 The reporting of wrong cause or mechanism of death or lack of an acceptable underlying cause of death in DCs is common in most of related studies. DCE was found in 100% in documenting either as wrong cause or mechanism of death; 98.8% listed “cardiopulmonary arrest” as the cause of death.19
Most of the deaths occurred in the intensive care units. For this reason, we performed analysis of pediatric DCs from PICU of new public hospital for children for this reason. However, most of the clinical reports on DCs are from hospital-based data.20 Few published reports are disease specific like cancer or injuries.21,22 As far as our knowledge, there is no standardized system of documenting death certificates in Pakistan. However, there was near 100% error in drafting DCs from two local institutions.13,19
The WHO recommended international standard DC was implemented almost a decade ago in Bangladesh after education and training in preparing the death document.23 Despite all major and minors, one remarkable observation was in our cohort that there was zero used of abbreviation in any DCs. It was reported in various studies, ranging from 39%- 58%.5,10,12 There is an urgent need to initiate interactive educational training and workshops on drafting cause of death in DCs, with periodic audit and provision of feedback to all physicians at national to improve the accuracy and completeness of DC, which lead to improve the mortality statistics of Pakistan. Several different educational interventions have been attempted in different healthcare settings to improve the quality of DCs in the last decade, with varying rate of success.15,24-26
There were several strengths and limitations in our study. This study is unique for several reasons. We used clearly defined errors types in our study, which can be used for comparison in future studies. It is an exploratory study and results need to be validated by other PICUs. We examined the contents of all DCs from electronic medical records rather than code data. However, we knew that it is a single center, small sample size, limited to only medical illnesses and probability of missing and inaccurate data due to retrospective in origin.
Reporting of erroneous cause of death is a serious concern in DCs. There is an urgent need for training, interactive workshops, periodic audits with provision of feedback of health-care providers on drafting the cause of death on DCs to improve accurate completion of DCs and for better health statistics.
7. Data availability
The numerical data generated during this research is available with the authors.
8. Conflict of interest
All authors declare that there was no conflict of interest.
9. Disclosure
The abstract of this study was presented as oral presentation in Critical Care Congress 2024, dated January 21-24 at Phoenix, AZ, USA [Abstract #: A-306]. Critical Care Medicine 52(1):p S128, January 2024.
10. Authors’ contribution
UF: Designed, did data collection, analysis and initial draft of manuscript.
MN: Did data collection.
AH: Conceived idea and did critical review, editing and final guarantor of manuscript.
Authors affiliations:
- Urooj Faisal, FCPS, PEDS, Fellow Pediatric Critical Care Medicine, Department of Pediatrics, Division of Pediatric Intensive Care Unit, Sindh Institute of Child Health and Neonatology (SICHN), Karachi, Pakistan; Email: uroojmalik@gmail.com
- Marium Noor, MBBS, Medical Officer, Department of Pediatrics, Division of Pediatric Intensive Care Unit, Sindh Institute of Child Health and Neonatology (SICHN), Karachi, Pakistan; Email: mariumnoor09@gmail.com
- Anwarul Haque, DAMP, DABPCCM, Professor, Department of Pediatrics, Division of Pediatric Intensive Care Unit, Sindh Institute of Child Health and Neonatology (SICHN), Karachi, Pakistan; Email: anwar2haque@gmail.com
ABSTRACT
Background & objective: Accurate completion of Death Certificate (DC) is vital information of health statistics. Limited data is available on pediatric death certificates especially from Pakistan. The rationale of this study was to evaluate the accuracy and completeness of DC issued from a pediatric intensive care unit (PICU).
Methodology: A descriptive cross-sectional study was conducted in PICU of new public-sector pediatric in Karachi from January to June 2023. All deaths in children (1 month -15 years) occurred in PICU from medical illnesses and DCs were prepared by junior doctors. A total of 163 DCs were reviewed for major and minor errors in cause of death according to WHO international standards.
Results: Of 163 DCs, none were error-free. The total number of errors was 499 and mean number of errors was 3.06 per patient. The major errors were 306 and most common was mechanism of death reported as cardiopulmonary arrest as underlying cause of death (98.8%), minor errors were 193 and most common was the absence of time interval (100%).
Conclusion: Very high rate of errors was observed in death certificates from a pediatric intensive care unit. Educational interventions are urgently needed with follow-up study.
Abbreviations: COD: cause of death, DC: Death Certificate, MCCD: Medical Certificate of Cause of Death PICU: pediatric intensive care unit,
Keywords: Death certificate, Errors, Major and minor, Children, Cause of death
Citation: Faisal U, Noor M, Haque A. Critical analysis of death certificates issued by a public sector pediatric intensive care unit in Pakistan. Anaesth. pain intensive care 2025;29(9):1279-83. DOI: 10.35975/apic.v29i9.3065
Received: June 13, 2025; Revised: November 13, 2024; Accepted: December 23, 2025
1. INTRODUCTION
The Medical Certificate of Cause of Death (MCCD) is commonly called the Death certificate (DC), which is a permanent medico-legal document of individual’s death.1 It provides detailed information about an individual’s cause of death and his/her demographic characteristics.2 DC has a very important role in health statistics that can be used for research purposes, planning health policies and resource management.3 Reporting accurate and complete data in DC is a key element in evaluation of health information system.
A fundamental issue in DC is inaccurate and inadequate reporting on cause of death (COD) of individual, which leads to erroneous health statistics, especially in children from low- and middle-income countries. Mortality rate of children, especially under-five is very high in developing countries.4 The inaccurate reporting COD in children leads to a major challenge in epidemiological data. Studies have shown that the reporting of COD in DC is very poor worldwide with errors reporting from 20-100%.5-7 The World Health Organization (WHO) recommends the standard reporting the COD based on the International Classification of Diseases (ICD-10) classification of diseases. The ICD plays a crucial role in mortality statistics and analysis in standardization of cause of death reporting, facilitates international health monitoring and research, and contributes to efforts aimed at improving health outcomes and reducing mortality globally.8
The current form of DC was updated last in 2016, after more than 50 years as shown in Figure 1.
Figure 1: International Form of Medical Certificate of Cause of Death.
It has two parts: Part 1 is used to record sequence of events leading to death as immediate COD then intermediate COD and last one should be underlying COD, and Part 2 is used to record other significant conditions contributing to death.9 The COD is a chain of events like Acute Myocarditis leads to cardiogenic shock and terminal event was “cardiac arrest”, which is mechanism of death and not cause of death.
Several reports have been published on accuracy of DC worldwide.6 Errors in death certificates (DCE), especially from pediatric critical care units are rarely reported.10 The rationale of this study was to evaluate the accuracy and completeness of DC issued from a pediatric intensive care unit of a newly established public-sector Children’s Hospital, Korangi. The objective of this study is to assess the frequency and types of errors in preparing DC by a physician.
2. METHODOLOGY
A descriptive and cross-sectional study was conducted to evaluate all DCs of children aged 1-month to 15-years admitted in the pediatric intensive care unit (PICU) of Sindh Institute of Child Health & Neonatology (SICHN) Korangi, Karachi over a six-month period from January 1 to June 30, 2023. The study was approved by the institutional Ethical Review Committee (SICHN/Ex-004/2024 September 25,2023). SICHN is a pediatric health-initiative by the Sindh Government of Pakistan, providing high-quality medical care free of cost to critically ill children all over Sindh. SICHN Korangi is a 200-beded tertiary care teaching hospital located in a very low socio-economic area of metropolis city of Karachi and serving a population of more than 2.5 million.
The Pediatric Intensive Care Unit (PICU) at SICHN is a closed multi-disciplinary unit that provides critical care services to children suffering from life-threatening conditions. The 28-bedded PICU has all 4-S components. All deaths in the study period that occurred and for which death certificates and medical records were available were included. We retrospectively reviewed the medical records of eligible patients and collected the following data into a structured data collection sheet including: age, gender, admitting diagnosis, co-morbidity and details of death certificate based on format of WHO-MCCD. We included only natural deaths occurred in PICU during study period and excluded unnatural deaths. The medical officers or pediatric resident-trainees prepared all DCs. Errors were divided into major and minor errors according to the criteria described in the previous studies and were described in Table 1.11
| Table I: Definitions of major and minor errors in death certificate. | ||
| Type of error | Definition | |
| MAJOR CAUSES: (Influence the cause of death) | Mechanism of death listed without an underlying cause | Mechanism or non-specific condition listed as underlying cause of death |
| Improper sequencing | Sequence of events does not make sense; underlying cause of death not listed on the lowest completed line of Part I | |
| Competing causes | Two or more causally unrelated, etiologically specific diseases listed in Part I |
|
| MINOR CAUSES:
(Doesn’t influence the cause of death) |
Use of Abbreviations | Abbreviations used to identify diseases |
| Time interval between death and each diagnosis was not stated | No time intervals listed in Part I or Part II | |
| Mechanism of death followed by a legitimate underlying cause of death |
Use of a mechanism, but qualified by an etiologically specific cause of death | |
All data entered into Microsoft Excel 2010. Data was presented as number and percentages either as means with standard deviation or median with range. Descriptive statistics were applied for analysis by using simple mathematical calculation. The estimated sample size for this study is 151 if prevalence of 89% errors in pediatric death certificate with a 95% confidence interval and 5% margin of error.10 After adding 10% drop out; then final cohort size is 166. Convenient sampling was taken. The primary outcome of this study was to assess the frequency and types of errors in DCs.
3. RESULTS
During the study period, 288 (15.1% of admission) death certificates were issued, consecutive 166 DCs were reviewed and three were excluded due to non-availability of DC from electronic medical records. Patients’ characteristics were shown in Table 2. Disease classification according to 1CD 10 is given in Figure 2. No DC was error-free. The total numbers of errors were 499 in 163 DCs. The major and minor errors in DCs were 294 and 185 respectively.
| Table 2: Demographic Data | |
| Total Admissions | 1899 |
| Mortality | 288 (15.1%) |
| Age Median Range |
8.4 Months 1 Months-15 Years |
| Male: Female | 60:40 |
Figure 2: Classification of diseases according to ICD 10
The characteristics of errors in DC are shown in Table 3. Frequencies of major errors are given in Figure 3.
| Table 3: Details of errors | |
| Error | N (%) |
| Total number of errors | 49 |
| Major errors | 30 (61.32) |
| Minor errors | 19 (38.68) |
| ≥ 3 errors in one patient | 15 (98.36) |
| Major errors alone in patient | 0 (0) |
| Minor errors alone in patient | 4 (2.5) |
| Mixed major and minor errors | 159 (97.5) |
Figure 3: Frequencies of major errors.
The mean number of errors was 3.06 per patient. The most common major error was reporting mechanism of death as the immediate cause of death (ICOD). The cardiopulmonary arrest was alone documented as Underlying Cause of Death (UCOD) in 161 DCs (98.8%). 97% (158) DCs had improper sequencing.
Compared to major error, there was a smaller number of minor errors in DCs. There was no abbreviation used in DCs of our cohort. There were 100 % lack of documenting timeline and Other Significant Conditions (OSC) in all DCs.
4. DISCUSSION
The accuracy and appropriate completeness of death certificate is paramount for mortality statistics and public health surveillance. We found a very high rate of errors (100%) in DCs and almost ≥3 errors per DC. Previously; the errors in DCs have been described in various categories and grades of severity of errors in published literature. For last one decade, reporting of errors in DCs was categorized as “major errors” and “minor errors” with few sub-headings with simple and clear explanation to create a better standardization.6 We compared our results with similar studies and observations were similar too. Gupta et al observed 89% errors in 1251 DCs of children with ratio of almost one error per patient.10 Atreya et al reported mechanism of death as ICOD in 78% of their evaluation of errors in DC from hospital-based study from Nepal.5 Qaddumi et al (2017) found almost 45% as a major error in reporting underlying cause of death in a descriptive report from Palestine.12 Haque et al also reported 200 errors in 202 DCs of adult patients (almost one error per DC) from a tertiary-care teaching hospital of Pakistan.13 Errors in DCs is very common worldwide with range from 20%-100%.6,7 Most of reports are hospital-based on DCE as well as COD worldwide. There are available two systemic reviews and meta-analysis on DCE and COD.5,14. However, there were few pediatric reports and two reports from adult ICU.15,16
We have 306 (61.3%) major errors and 193 (38.7%) minor errors in our cohort. The numbers of major and minor errors per DC were 0.6 and 0.4 respectively. Both multiple and mixed errors were common like in other reports. The most common major error in our cohort was reporting mechanism of death as ICOD (98.8%). Most of DCE occurred in underlying and immediate COD worldwide.17,18 The reporting of wrong cause or mechanism of death or lack of an acceptable underlying cause of death in DCs is common in most of related studies. DCE was found in 100% in documenting either as wrong cause or mechanism of death; 98.8% listed “cardiopulmonary arrest” as the cause of death.19
Most of the deaths occurred in the intensive care units. For this reason, we performed analysis of pediatric DCs from PICU of new public hospital for children for this reason. However, most of the clinical reports on DCs are from hospital-based data.20 Few published reports are disease specific like cancer or injuries.21,22 As far as our knowledge, there is no standardized system of documenting death certificates in Pakistan. However, there was near 100% error in drafting DCs from two local institutions.13,19
The WHO recommended international standard DC was implemented almost a decade ago in Bangladesh after education and training in preparing the death document.23 Despite all major and minors, one remarkable observation was in our cohort that there was zero used of abbreviation in any DCs. It was reported in various studies, ranging from 39%- 58%.5,10,12 There is an urgent need to initiate interactive educational training and workshops on drafting cause of death in DCs, with periodic audit and provision of feedback to all physicians at national to improve the accuracy and completeness of DC, which lead to improve the mortality statistics of Pakistan. Several different educational interventions have been attempted in different healthcare settings to improve the quality of DCs in the last decade, with varying rate of success.15,24-26
5. LIMITATIONS
There were several strengths and limitations in our study. This study is unique for several reasons. We used clearly defined errors types in our study, which can be used for comparison in future studies. It is an exploratory study and results need to be validated by other PICUs. We examined the contents of all DCs from electronic medical records rather than code data. However, we knew that it is a single center, small sample size, limited to only medical illnesses and probability of missing and inaccurate data due to retrospective in origin.
6. CONCLUSION
Reporting of erroneous cause of death is a serious concern in DCs. There is an urgent need for training, interactive workshops, periodic audits with provision of feedback of health-care providers on drafting the cause of death on DCs to improve accurate completion of DCs and for better health statistics.
7. Data availability
The numerical data generated during this research is available with the authors.
8. Conflict of interest
All authors declare that there was no conflict of interest.
9. Disclosure
The abstract of this study was presented as oral presentation in Critical Care Congress 2024, dated January 21-24 at Phoenix, AZ, USA [Abstract #: A-306]. Critical Care Medicine 52(1):p S128, January 2024.
10. Authors’ contribution
UF: Designed, did data collection, analysis and initial draft of manuscript.
MN: Did data collection.
AH: Conceived idea and did critical review, editing and final guarantor of manuscript.
11. REFERENCES
- Kotabagi RB, Chaturvedi RK, Banerjee A. Medical certification of cause of death. Med J Armed Forces India. 2004 Jul 1;60(3):261-72. PMCID: PMC4923180 DOI: 1016/S0377-1237(04)80060-1
- Mayorathan U. The Management of Death in Sri Lanka and Potential Solutions for the Future. Jaffna Medical Journal. 2023 Dec 31;35(2). DOI: 10.4038/jmj.v35i2.187
- Brooks EG, Reed KD. Principles and pitfalls: a guide to death certification. Clinical medicine & research. 2015 Jun 1;13(2):74-82. PMCID: PMC4504663 DOI: 3121/cmr.2015.1276
- Tharwani ZH, Bilal W, Khan HA, Kumar P, Butt MS, Hamdana AH, et al. Infant & child mortality in Pakistan and its determinants: a review. INQUIRY: The Journal of Health Care Organization, Provision, and Financing. 2023 Apr;60:00469580231167024. PMCID: PMC10126599 DOI: 1177/00469580231167024
- Atreya A, Acharya B, Yadav PP, Menezes RG, Nepal S. Evaluation of errors on death certificates. J Nepal Health Res Counc. 2024 Jun 22;22:150-6. DOI: 33314/jnhrc.v22i01.4941
- Alipour J, Payandeh A. Common errors in reporting cause-of-death statement on death certificates: a systematic review and meta-analysis. J Forensic Leg Med. 2021 Aug 1;82:102220. DOI: 1016/j.jflm.2021.102220
- Madadin M, Alhumam AS, Bushulaybi NA, Alotaibi AR, Aldakhil HA, Alghamdi AY, et al. Common errors in writing the cause of death certificate in the Middle East. J Forensic Leg Med. 2019 Nov 1;68:101864. DOI: 1016/j.jflm.2019.101864
- World Health Organization. (1979). Medical certification of cause of death : instructions for physicians on use of international form of medical certificate of cause of death, 4th ed. World Health Organization. https://iris.who.int/handle/10665/40557
- World Health Organization. International statistical classification of diseases and related health problems. 10th revision. Geneva: WHO; 2016. Available from: https://www.who.int/classifications/icd/ICD10Volume2_en_2010.pdf.
- Gupta N, Bharti B, Singhi S, Kumar P, Thakur JS. Errors in filling WHO death certificate in children: lessons from 1251 death certificates. J Trop Pediatrics. 2014 Feb 1;60(1):74-8. DOI: 1093/tropej/fmt059
- Myers KA, Farquhar DR. Improving the accuracy of death certification. CMAJ. 1998 May 19;158(10):1317-23. PMCID: PMC1229326
- Qaddumi JA, Nazzal Z, Yacoup AR, Mansour M. Quality of death notification forms in North West Bank/Palestine: a descriptive study. BMC Research Notes. 2017 Dec;10:1-6. PMCID: PMC5387246 DOI: 1186/s13104-017-2469-0
- Haque AS, Shamim K, Siddiqui NH, Irfan M, Khan JA. Death certificate completion skills of hospital physicians in a developing country. BMC Health Serv Res. 2013 Dec;13:1-5. PMCID: PMC3717134 DOI: 1186/1472-6963-13-205
- Al Busaidi S, Al Alawi AM, Al Masruri R, Al Balushi S, Al-Badi A. Quality of death certification based on the documented underlying cause of death: a retrospective study. J Forensic Leg Med 2023 Jul 1;97:102547. DOI: 1016/j.jflm.2023.102547
- Azim A, Singh P, Bhatia P, Baronia AK, Gurjar M, Poddar B, Singh RK. Impact of an educational intervention on errors in death certification: An observational study from the intensive care unit of a tertiary care teaching hospital. J Anaesthesiol Clin Pharmacol 2014 Jan 1;30(1):78-81. PMCID: PMC3927298 DOI: 4103/0970-9185.125708