Khizra Saleem 1*, Tasmina Panhwer 2 , Muhammad Khalid 3 , Sherwali Khan 4 , Anwar Ul Haque 5
Authors affiliations:
Background & objective: This study aimed to determine the accuracy of the perfusion index (PI) as a predictor of mortality in critically ill pediatric patients.
Methodology: A prospective observational study was conducted from September 2023 to February 2024 in the Pediatric Intensive Care Unit (PICU) of the Sindh Institute of Child Health and Neonatology (SICHN). All patients aged 1 month to 15 years who did not undergo any interventions were included. Perfusion index (PI) values were measured at 0, 1, and 6 hours using a Masimo Radical-7 pulse oximeter, along with documentation of hemodynamic parameters.
Results: Among 296 critically ill children (median age: 9 months), 84 (28.4%) died. A total of 888 PI readings were recorded. At 0 hours, 47% had a PI < 1.0, which was significantly associated with mortality (p < 0.001). Perfusion Index (PI) at 0 hours showed 76.2% sensitivity and 64.6% specificity; at 6 hours, specificity rose to 87.3%. ROC analysis showed AUCs of 0.75 and 0.74 at 0 and 6 hours, respectively. Persistently low PI was linked with higher mortality.
Conclusions: A persistently low perfusion index (PI) is associated with increased mortality in critically ill pediatric patients, supporting it as a non-invasive early risk stratification and triage tool in the PICU.
Abbreviations: PI: Perfusion index, PICU: Pediatric Intensive Care Unit, SI: shock index, ScvO₂: central venous oxygen saturation, SET: Signal Extraction Technology
Keywords: Perfusion index; Pediatric ICU; Pulse Oximetry; Mortality; Infant; Child
Citation: Saleem K, Panhwer T, Khalid M, Khan S, Haque AU. Perfusion index as a non-invasive predictor of mortality in the pediatric ICU: a prospective observational study. Anaesth. pain intensive care 2025;29(8):912-918. DOI: 10.35975/apic.v29i8.3018.
Received: July 18, 2025; Revised: August 05, 2025; Accepted: August 06, 2025
Hemodynamic monitoring is essential in managing critically ill children admitted to pediatric intensive care units (PICUs). Traditionally, clinical assessments have focused on macrocirculatory parameters such as blood pressure and cardiac output. Emerging research suggests that microcirculatory markers may offer a more accurate assessment of tissue perfusion and overall circulatory health than traditional macrocirculatory measures.1
Invasive markers like serum lactate, central venous oxygen saturation (ScvO₂), and the central venous-to-arterial PCO₂ gap are frequently employed in high-income settings but remain impractical in many low- and middle-income countries (LMICs) due to the need for specialized equipment and personnel.2,3 As a result, there is growing interest in non-invasive tools that can be applied reliably in resource-constrained settings.
The perfusion index (PI), derived from pulse oximetry, is a non-invasive and continuous indicator of peripheral perfusion. It reflects the ratio between pulsatile (arterial) and non-pulsatile (venous and capillary) blood flow, influenced primarily by stroke volume and vasomotor tone.4,5 Variations in PI have been associated with early shock, fluid responsiveness, and outcomes in critically ill patients. 6,7
The PI serves as a useful triage tool, providing earlier prediction of mortality and ICU stay duration than traditional indicators such as lactate.8,9 Moreover, it may aid in evaluating fluid responsiveness, particularly in spontaneously breathing patients.10 Pathological values vary by age, with thresholds of <1.15 in children under 3 years, <1.25 for ages 3–10, and <1.55 for ages 10–12 years. 11 Perfusion Index has been increasingly recognized as a prognostic indicator of morbidity and mortality in pediatric critical care settings.12 Despite its advantages, its utility in predicting mortality in critically ill pediatric patients, particularly in LMIC settings, remains under-explored.
It was hypothesized that lower perfusion index values are associated with higher in-hospital mortality among critically ill children. The present study evaluates the predictive accuracy of the perfusion index in determining in-hospital mortality, addressing the existing gap in pediatric-specific evidence for this non-invasive hemodynamic marker.
This single-center prospective, observational study was conducted over 6 months, from September 2023 to February 2024 at one of the largest pediatric Intensive Care Units of an academic hospital. The study was approved by institutional ethics review committee (IEC: SICHN/IRB-002/2023).
A total of 296 critically ill children aged one month to 15 years admitted to PICU. were included. Children with congenital heart disease, limb anomalies, or prior treatment at another healthcare facility were excluded. The collected data encompassed demographic, clinical, laboratory, and outcome-related variables. Hemodynamic variables, including heart rate, capillary refill time, systolic blood pressure, mean arterial pressure (MAP), and shock index (SI), calculated as heart rate divided by systolic blood pressure, were recorded at 0, 1, and 6 hours.
The perfusion index (PI) was measured using Masimo Radical-7 pulse oximeters (2012 model) with Signal Extraction Technology (SET). Sensors were applied to the finger or toe, depending on optimal signal quality, and maintained at the same site throughout measurements unless repositioning was necessary due to signal interference. If difficulties arose, the site was changed.
PI values were recorded after verifying an artifact-free plethysmographic waveform, with measurements taken for 20 seconds every minute over 3 minutes.13 The average of three readings was used. In the emergency department, ambient room temperature was used, whereas in the PICU, the environment was maintained at 22–24°C. PI values remained consistent across finger and toe sites, with minimal intra-patient variability.
Data were analyzed using SPSS version 23.0. Continuous variables were presented as means ± SD or as medians with interquartile ranges (IQRs) if not normally distributed. Categorical variables were expressed as frequencies and percentages. Comparisons between survivors and non-survivors, as well as between low PI and normal PI groups on admission, were performed using the t-test (or Mann–Whitney U test for non-normally distributed data) and the chi-square test, respectively, at a 5% significance level. Correlations between admission PI and clinical hemodynamic parameters were assessed using Pearson’s correlation coefficient (r). Receiver operating characteristic (ROC) curve analysis was performed to evaluate the predictive ability of the perfusion index (PI) and shock index (SI) at 0 and 6 hours for mortality. The area under the curve (AUC) was calculated, and the optimal cutoff for PI was determined using the Youden Index (J), defined as J = Sensitivity + Specificity – 1.
Among the 296 children with sepsis, the median age was 9 months (IQR: 18), and 53% were male. Malnutrition was present in 41.2% of cases, and 16.9% had comorbid conditions. Multiple organ dysfunction syndrome was observed in 14.5% of patients. The overall in-hospital mortality rate was 28.4%.
The most frequently involved system was respiratory system (41.6%), followed by the nervous (13.2%) and cardiovascular (12.8%) systems. At admission, the mean perfusion index (PI) was 1.4 ± 1.2, with 47% of patients presenting with a low PI (<1.0). By 6 hours, the mean PI increased to 1.8 ± 1.1, and the proportion of children with low PI (<1.0) decreased to 22%, indicating possible hemodynamic improvement.
Baseline characteristics including age, gender, weight, malnutrition and presence of comorbidity were comparable in survivors and non-survivors. However, the prevalence of multiple organ dysfunction syndrome (MODS) was significantly higher in non-survivors compared to survivors (32.1% vs. 7.5%). Similarly, the prevalence of respiratory illness was more common in survivors (50.5% vs. 19.0%) and cardiovascular disease was more common in non-survivors (29.8% vs. 6.1%) (Table 1).Heart rate showed a decreasing trend at 6 hours. Capillary refill time remained stable at 3.0 ± 1.0 seconds initially but improved slightly to 2.7 ± 0.7 seconds by 6 hours. A decline was observed in systolic, diastolic, and mean arterial pressures over time. An improvement in perfusion index was observed from admission (1.4 ± 1.2) to 6 hours (1.8 ± 1.1) indicating potential hemodynamic stabilization. The admission perfusion index (PI 0-hrs) in non-survivors was significantly lower compared to survivors (0.8 ± 0.9 vs. 1.6 ± 1.3, P < 0.001). PI at 6 hours remained significantly lower in non-survivors (1.1 ± 0.9 vs 1.9 ± 1.0, P < 0.001) (Table 2).
At admission, low PI (<1.0) was more prevalent among non-survivors (76.2%) than survivors (35.4%), demonstrating its early association with mortality risk. At 6 hours, the overall prevalence of low PI declined; however, it remained present in 45.2% of non-survivors (38 of 84) compared to just 12.7% of survivors (27 of 212), highlighting its continued association with adverse outcomes.
Diagnostic accuracy of low PI (<1.0) for predicting mortality improved from 67.9% at baseline to 75.3% at 6 hours. At admission, the positive predictive value (PPV) of low PI was moderate (~46%), while the negative predictive value (NPV) was high, indicating that normal PI was strongly associated with survival (Table 3).
The receiver operating characteristic (ROC) analysis was performed to evaluate the predictive ability of Perfusion Index (PI) and Shock Index (SI) at 0 hours for mortality. The area under the curve (AUC) for PI_0hr was 0.747 (95% CI: 0.682 – 0.812, P < 0.001), indicating moderate diagnostic accuracy. In contrast, the AUC for SI_0hr was 0.389 (95% CI: 0.311 – 0.468, P = 0.004), which is below 0.5, indicating poor discrimination and limited reliability as a prognostic marker. The optimal cutoff for PI_0hr, determined using the Youden Index, was 0.59, yielding a sensitivity of 0.739 and specificity of 0.592.(Figure 1) However, due to the poor AUC of SI_0hr, no meaningful cutoff could be determined.
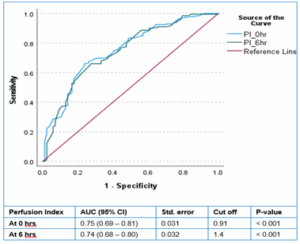
Figure 1: AUC: area under curve
Similarly, the ROC analysis for PI and SI at 6 hours was conducted to assess their prognostic utility. The AUC for PI_6hr was 0.744 (95% CI: 0.676 – 0.812, p < 0.001), indicating moderate predictive accuracy. In contrast, the AUC for SI_6hr was 0.428 (95% CI: 0.345 – 0.512, p = 0.068), which remains below 0.5, suggesting poor discrimination and limited clinical utility for mortality prediction. (Figure 2)
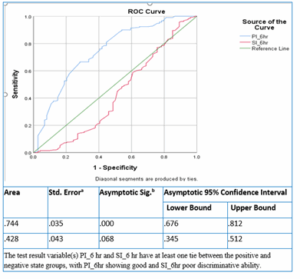
Figure 2: AUC curve at 6 hours
In this prospective observational study of the pulse oximetry-derived perfusion index, which included all patients admitted to the pediatric ICU during the study period, two major conclusions were drawn. First, the prognostic value of PI was demonstrated through the association of an initially low PI and failure to respond to resuscitative measures with high mortality. The second observation was the detection of occult shock using PI when clinical signs of shock were not present. In this study, 47% of patients had a low perfusion index on admission; improvement in the perfusion index was observed over time with treatment, and high mortality was noted in children with a low perfusion index at baseline and a persistently low PI after treatment. PI enhances the accuracy of hemodynamic assessment and perfusion status evaluation; its non-invasive nature makes it a convenient tool for continuous assessment of tissue perfusion and microcirculatory status.14
Clinical studies in pediatric shock have assessed the correlation of PI with signs of peripheral perfusion such as capillary refill time, hemodynamic variables such as heart rate and blood pressure, and biochemical signs of shock such as lactate levels.15 Talay et al. (2023), reported a significant correlation of PI with capillary refill time (P < 0.05) in children with shock.16 Similarly, there was also a good correlation between PI and heart rate as well as systolic blood pressure in the reports of Sivaprasath et al. (2019),17 and Ullah et al.(2021).15 PI has emerged as a useful parameter in the early recognition of shock and monitoring response to therapy in critically ill children, especially in resource-constrained settings. It has been widely used in many acute care settings, including emergency rooms, anesthesia, intensive care units, and trauma care.18 Kockan et al. compared PI with age-specific SI and demonstrated that non-survivors had significantly lower perfusion index (PI) values and higher average shock index (ASI) compared to survivors. 19
Alakaya et al. reported that PI is a valuable parameter to predict mortality in patients admitted in pediatric intensive care units. In their study, the specificity and sensitivity of low PI for mortality among 372 critically ill children were 90.1% and 75.9% respectively. 5 Published reports have demonstrated a direct correlation between low PI and mortality, identifying it as a prognostic marker in children admitted to PICU with variable values of sensitivity, specificity and area under the curve.6,20 A secondary analysis of a multicenter study in children with severe malaria showed low admission PI associated with two-fold greater odds of in-hospital mortality (OR, 2.44 [1.02–5.88]; P = 0.045) and a sensitivity and specificity of 51.4% and 63.4%, respectively for mortality. 1
There is no consensus on normal and pathological values of PI in children of different ages. The optimal cut-off of mean PI on admission in PICU was 0.91 for prediction of mortality in critically ill children in this study. However, Lalitha et al. observed a critical PI of <0.6 in their study including 50% of children with septic shock, and found a 42% improvement in PI at 6 hours.13 The sensitivity of a low PI for predicting mortality decreased from 76% at baseline to 45% indicating a lower ability to correctly identify non-survivors at 0-hour compared to the 6-hours measurements respectively. However, specificity improved significantly from 64% to 87, suggesting a stronger ability to correctly classify survivors. The negative predictive value remained relatively consistent over time, indicating PI as a strong predictor of survival supporting its use for risk stratification in pediatric sepsis.
The ROC analysis in our study indicated that PI AUC of 0.75 at 1 and 0.74 at 6 hours helps in predicting mortality among children with sepsis. This suggests that PI measurement at the thresholds used (low <1.0, normal ≥1.0) can provide a fair indication of mortality risk, with low PI values being moderately associated with higher likelihood of mortality compared to normal PI values. Mortality was notably higher in patients with low PI at 6 hours with 58.5%, who did not survive, compared to 19.9% in the normal PI group. These findings suggest that persistent low PI at 6 hours is strongly associated with critical illness, increased severity, and a significantly higher risk of mortality in pediatric sepsis.
The prospective design of this study, including a wide spectrum of clinical diagnoses in critically ill patients, strengthens its findings and highlights the perfusion index as a valuable tool for hemodynamic assessment and outcome prediction in the PICU. However, the moderate AUC value of PI indicates that it may not fully predict the outcome on its own and should ideally be used as an adjunct to other clinical indicators.
This study has several limitations, including a relatively small sample size, its single-center design, arbitrary time points for measurements, and the inclusion of a wide range of age groups. These factors may influence the generalizability of the findings and warrant further multicenter studies with standardized protocols to validate the results. This study did not include a comparison of the perfusion index with other peripheral tissue perfusion indicators, such as capillary refill time, core-to-peripheral temperature gradient, or mottling score, nor with established disease severity scores as outcome predictors. Incorporating these comparisons could have further strengthened the findings and underscored the perfusion index as a valuable adjunct in critical care assessment.
Almost half of the children had a low PI on admission to the PICU, and one-quarter failed to improve after therapeutic interventions. Low PI at admission and after resuscitation were strong predictors of mortality. A large, multicenter prospective study with well-defined PI reference values for children of different ages admitted to the PICU is needed.
Authors affiliations:
- Khizra Saleem, Sindh Institute of Child Health & Neonatology, Karachi, Pakistan; Email: khizrasaleem22@gmail.com, {ORCID: 0009-0003-4970-3153}
- Tasmina Panhwer, Sindh Institute of Child Health & Neonatology, Karachi, Pakistan; Email: panhwertasmina92@yahoo.com, {ORCID: 0009- 0006-9441-5734}
- Muhammad Khalid, Nishtar Medical University & Hospital, Multan, Pakistan; Email: khalidsaleem2001@hotmail.com, {ORCID: 0000-0003-3179-167X}
- Sherwali Khan, Sindh Institute of Child Health & Neonatology, Karachi, Pakistan; Email: khansheryafzal@gmail.com
- Anwar Ul Haque, Sindh Institute of Child Health & Neonatology, Karachi, Pakistan; Email: Anwar2haque@gmail.com, {ORCID: 0000-0002-5223-8892}
ABSTRACT
Background & objective: This study aimed to determine the accuracy of the perfusion index (PI) as a predictor of mortality in critically ill pediatric patients.
Methodology: A prospective observational study was conducted from September 2023 to February 2024 in the Pediatric Intensive Care Unit (PICU) of the Sindh Institute of Child Health and Neonatology (SICHN). All patients aged 1 month to 15 years who did not undergo any interventions were included. Perfusion index (PI) values were measured at 0, 1, and 6 hours using a Masimo Radical-7 pulse oximeter, along with documentation of hemodynamic parameters.
Results: Among 296 critically ill children (median age: 9 months), 84 (28.4%) died. A total of 888 PI readings were recorded. At 0 hours, 47% had a PI < 1.0, which was significantly associated with mortality (p < 0.001). Perfusion Index (PI) at 0 hours showed 76.2% sensitivity and 64.6% specificity; at 6 hours, specificity rose to 87.3%. ROC analysis showed AUCs of 0.75 and 0.74 at 0 and 6 hours, respectively. Persistently low PI was linked with higher mortality.
Conclusions: A persistently low perfusion index (PI) is associated with increased mortality in critically ill pediatric patients, supporting it as a non-invasive early risk stratification and triage tool in the PICU.
Abbreviations: PI: Perfusion index, PICU: Pediatric Intensive Care Unit, SI: shock index, ScvO₂: central venous oxygen saturation, SET: Signal Extraction Technology
Keywords: Perfusion index; Pediatric ICU; Pulse Oximetry; Mortality; Infant; Child
Citation: Saleem K, Panhwer T, Khalid M, Khan S, Haque AU. Perfusion index as a non-invasive predictor of mortality in the pediatric ICU: a prospective observational study. Anaesth. pain intensive care 2025;29(8):912-918. DOI: 10.35975/apic.v29i8.3018.
Received: July 18, 2025; Revised: August 05, 2025; Accepted: August 06, 2025
1. INTRODUCTION
Hemodynamic monitoring is essential in managing critically ill children admitted to pediatric intensive care units (PICUs). Traditionally, clinical assessments have focused on macrocirculatory parameters such as blood pressure and cardiac output. Emerging research suggests that microcirculatory markers may offer a more accurate assessment of tissue perfusion and overall circulatory health than traditional macrocirculatory measures.1
Invasive markers like serum lactate, central venous oxygen saturation (ScvO₂), and the central venous-to-arterial PCO₂ gap are frequently employed in high-income settings but remain impractical in many low- and middle-income countries (LMICs) due to the need for specialized equipment and personnel.2,3 As a result, there is growing interest in non-invasive tools that can be applied reliably in resource-constrained settings.
The perfusion index (PI), derived from pulse oximetry, is a non-invasive and continuous indicator of peripheral perfusion. It reflects the ratio between pulsatile (arterial) and non-pulsatile (venous and capillary) blood flow, influenced primarily by stroke volume and vasomotor tone.4,5 Variations in PI have been associated with early shock, fluid responsiveness, and outcomes in critically ill patients. 6,7
The PI serves as a useful triage tool, providing earlier prediction of mortality and ICU stay duration than traditional indicators such as lactate.8,9 Moreover, it may aid in evaluating fluid responsiveness, particularly in spontaneously breathing patients.10 Pathological values vary by age, with thresholds of <1.15 in children under 3 years, <1.25 for ages 3–10, and <1.55 for ages 10–12 years. 11 Perfusion Index has been increasingly recognized as a prognostic indicator of morbidity and mortality in pediatric critical care settings.12 Despite its advantages, its utility in predicting mortality in critically ill pediatric patients, particularly in LMIC settings, remains under-explored.
It was hypothesized that lower perfusion index values are associated with higher in-hospital mortality among critically ill children. The present study evaluates the predictive accuracy of the perfusion index in determining in-hospital mortality, addressing the existing gap in pediatric-specific evidence for this non-invasive hemodynamic marker.
2. METHODOLOGY
This single-center prospective, observational study was conducted over 6 months, from September 2023 to February 2024 at one of the largest pediatric Intensive Care Units of an academic hospital. The study was approved by institutional ethics review committee (IEC: SICHN/IRB-002/2023).
A total of 296 critically ill children aged one month to 15 years admitted to PICU. were included. Children with congenital heart disease, limb anomalies, or prior treatment at another healthcare facility were excluded. The collected data encompassed demographic, clinical, laboratory, and outcome-related variables. Hemodynamic variables, including heart rate, capillary refill time, systolic blood pressure, mean arterial pressure (MAP), and shock index (SI), calculated as heart rate divided by systolic blood pressure, were recorded at 0, 1, and 6 hours.
The perfusion index (PI) was measured using Masimo Radical-7 pulse oximeters (2012 model) with Signal Extraction Technology (SET). Sensors were applied to the finger or toe, depending on optimal signal quality, and maintained at the same site throughout measurements unless repositioning was necessary due to signal interference. If difficulties arose, the site was changed.
PI values were recorded after verifying an artifact-free plethysmographic waveform, with measurements taken for 20 seconds every minute over 3 minutes.13 The average of three readings was used. In the emergency department, ambient room temperature was used, whereas in the PICU, the environment was maintained at 22–24°C. PI values remained consistent across finger and toe sites, with minimal intra-patient variability.
Data were analyzed using SPSS version 23.0. Continuous variables were presented as means ± SD or as medians with interquartile ranges (IQRs) if not normally distributed. Categorical variables were expressed as frequencies and percentages. Comparisons between survivors and non-survivors, as well as between low PI and normal PI groups on admission, were performed using the t-test (or Mann–Whitney U test for non-normally distributed data) and the chi-square test, respectively, at a 5% significance level. Correlations between admission PI and clinical hemodynamic parameters were assessed using Pearson’s correlation coefficient (r). Receiver operating characteristic (ROC) curve analysis was performed to evaluate the predictive ability of the perfusion index (PI) and shock index (SI) at 0 and 6 hours for mortality. The area under the curve (AUC) was calculated, and the optimal cutoff for PI was determined using the Youden Index (J), defined as J = Sensitivity + Specificity – 1.
3. RESULTS
Among the 296 children with sepsis, the median age was 9 months (IQR: 18), and 53% were male. Malnutrition was present in 41.2% of cases, and 16.9% had comorbid conditions. Multiple organ dysfunction syndrome was observed in 14.5% of patients. The overall in-hospital mortality rate was 28.4%.
The most frequently involved system was respiratory system (41.6%), followed by the nervous (13.2%) and cardiovascular (12.8%) systems. At admission, the mean perfusion index (PI) was 1.4 ± 1.2, with 47% of patients presenting with a low PI (<1.0). By 6 hours, the mean PI increased to 1.8 ± 1.1, and the proportion of children with low PI (<1.0) decreased to 22%, indicating possible hemodynamic improvement.
Baseline characteristics including age, gender, weight, malnutrition and presence of comorbidity were comparable in survivors and non-survivors. However, the prevalence of multiple organ dysfunction syndrome (MODS) was significantly higher in non-survivors compared to survivors (32.1% vs. 7.5%). Similarly, the prevalence of respiratory illness was more common in survivors (50.5% vs. 19.0%) and cardiovascular disease was more common in non-survivors (29.8% vs. 6.1%) (Table 1).Heart rate showed a decreasing trend at 6 hours. Capillary refill time remained stable at 3.0 ± 1.0 seconds initially but improved slightly to 2.7 ± 0.7 seconds by 6 hours. A decline was observed in systolic, diastolic, and mean arterial pressures over time. An improvement in perfusion index was observed from admission (1.4 ± 1.2) to 6 hours (1.8 ± 1.1) indicating potential hemodynamic stabilization. The admission perfusion index (PI 0-hrs) in non-survivors was significantly lower compared to survivors (0.8 ± 0.9 vs. 1.6 ± 1.3, P < 0.001). PI at 6 hours remained significantly lower in non-survivors (1.1 ± 0.9 vs 1.9 ± 1.0, P < 0.001) (Table 2).
| Table 1: Demographic and clinical data of critically ill children admitted to PICU (N = 296) | ||||
| Characteristics | Overall
(N = 296) |
Survivors
(n = 212) |
Non-survivors
(n = 84) |
P-value* |
| Age - months (median, IQR) | 9, 18 | 8, 14 | 10.5, 19 | 0.283 |
| Gender – Male | 157 (53) | 119 (56.1) | 38 (45.2) | 0.090 |
| Weight (kg) | 8.7 ± 6.1 | 8.4 ± 5.8 | 9.6 ± 6.6 | 0.129 |
| Malnutrition | 122 (41.2) | 83 (39.2) | 39 (46.4) | 0.251 |
| Any Co-morbid condition | 50 (16.9) | 38 (17.9) | 12 (14.3) | 0.451 |
| Multiorgan dysfunction Syndrome | 43 (14.5) | 16 (7.5) | 27 (32.1) | < 0.001 |
| Provisional System Involved
Respiratory Cardiovascular Nervous system Miscellaneous |
123 (41.6) 38 (12.8) 39 (13.2) 96 (32.4) |
107 (50.5) 13 (6.1) 30 (14.2) 62 (29.2) |
16 (19.0) 25 (29.8) 9 (10.7) 34 (40.5) |
< 0.001 |
| Perfusion Index at 0 hrs. | 1.4 ± 1.2 | 1.6 ± 1.3 | 0.8 ± 0.9 | < 0.001 |
| Low PI (< 1.0) at 0 hrs. | 139 (47) | 75 (35.4) | 64 (76.2) | < 0.001 |
| Perfusion Index at 6 hrs. | 1.8 ± 1.1 | 1.9 ± 1.0 | 1.1 ± 0.9 | < 0.001 |
| Low PI (< 1.0) at 6 hrs. | 65 (22) | 27 (12.7) | 38 (45.2) | < 0.001 |
| Data are presented as n (%) or mean ± SD; *t-test for mean comparison, Mann-Whitney U test for median comparison and chi-square test for comparison of categorical data. P < 0.05 is considered significant | ||||
| Table 2: Clinical parameters of sepsis in children (N = 296) | ||||
| Parameter | Overall
(N = 296) |
Survivors
(n = 212) |
Non-Survivors
(n = 84) |
P-value* |
| Hear rate - 0 hrs 6 hrs |
151.5 ± 26.8 | 151.8 ± 27.5 | 150.7 ± 24.6 | 0.748 |
| 139.0 ± 25.2 | 137.4 ± 22.7 | 143.1 ± 29.2 | .113 | |
| Capillary Refill Time – -- 0 hrs - 6 hrs |
3.0 ± 1.0 | 2.8 ± 0.9 | 3.4 ± 1.1 | < 0.001 |
| 2.7 ± 0.7 | 2.6 ± 0.6 | 2.9 ± 0.9 | 0.005 | |
| Systolic Blood Pressure – 0 hrs - 6 hrs |
104.5 ± 17.3 | 106.6 ± 15.8 | 99.2 ± 18.8 | 0.002 |
| 100.8 ± 14.7 | 101.7 ± 14.5 | 98.4 ± 14.1 | 0.072 | |
| Diastolic Blood Pressure - 0 hrs - 6 hrs |
62.3 ± 16.5 | 63.4 ± 15.8 | 59.3 ± 16.7 | 0.045 |
| 58.5 ± 13.5 | 59.8 ± 13.6 | 55.0 ± 11.8 | 0.006 | |
| Mean Arterial Pressure – 0 hrs - 6 hrs |
76.0 ± 16.9 | 77.5 ± 16.4 | 71.9 ± 16.4 | 0.009 |
| 72.8 ± 16.2 | 74.2 ± 15.7 | 69.5 ± 13.6 | 0.017 | |
| Perfusion Index – 0 hrs. | 1.4 ± 1.2 | 1.6 ± 1.3 | 0.8 ± 0.9 | < 0.001 |
| Low PI (< 1.0) 0 hrs. | 139 (47) | 75 (35.4) | 64 (76.2) | < 0.001 |
| Perfusion Index – 6 hrs. | 1.8 ± 1.1 | 1.9 ± 1.0 | 1.1 ± 0.9 | < 0.001 |
| Low PI (< 1.0) 6 hrs. (Yes) | 65 (22) | 27 (41.5) | 38 (58.5) | < 0.001 |
| *Independent sample t-test, chi-square test for categorical comparison; Data are presented as n (%) or mean ± SD;
P < 0.05 is considered significant |
||||
At admission, low PI (<1.0) was more prevalent among non-survivors (76.2%) than survivors (35.4%), demonstrating its early association with mortality risk. At 6 hours, the overall prevalence of low PI declined; however, it remained present in 45.2% of non-survivors (38 of 84) compared to just 12.7% of survivors (27 of 212), highlighting its continued association with adverse outcomes.
Diagnostic accuracy of low PI (<1.0) for predicting mortality improved from 67.9% at baseline to 75.3% at 6 hours. At admission, the positive predictive value (PPV) of low PI was moderate (~46%), while the negative predictive value (NPV) was high, indicating that normal PI was strongly associated with survival (Table 3).
| Table 3: Diagnostic accuracy of low PI at baseline and 6-hours in predicting mortality in children (N = 296) | ||||
| Perfusion Index* | At Baseline | At 6-hours | ||
| Survivors | Non-survivors | Survivors | Non-survivors | |
| Low | 64 | 75 | 38 | 27 |
| Normal | 20 | 137 | 46 | 185 |
| Sensitivity Specificity Positive predictive Value Negative predictive Value Accuracy |
76.2% (95% CI: 65.7% to 84.8%) 64.6% (95% CI: 57.8% to 71.1%) 46.0% (95% CI: 40.7% to 51.5%) 87.3% (95% CI: 82.2% to 91.1%) 67.9% (95% CI: 62.3% to 73.2%) |
45.4% (95% CI: 34.3% to 56.5%) 87.3% (95% CI: 82.0% to 91.4%) 58.5% (95% CI: 47.9% to 68.3%) 80.1% (95% CI: 76.7% to 83.1%) 75.3% (95% CI: 70.0% to 80.1%) |
||
The receiver operating characteristic (ROC) analysis was performed to evaluate the predictive ability of Perfusion Index (PI) and Shock Index (SI) at 0 hours for mortality. The area under the curve (AUC) for PI_0hr was 0.747 (95% CI: 0.682 – 0.812, P < 0.001), indicating moderate diagnostic accuracy. In contrast, the AUC for SI_0hr was 0.389 (95% CI: 0.311 – 0.468, P = 0.004), which is below 0.5, indicating poor discrimination and limited reliability as a prognostic marker. The optimal cutoff for PI_0hr, determined using the Youden Index, was 0.59, yielding a sensitivity of 0.739 and specificity of 0.592.(Figure 1) However, due to the poor AUC of SI_0hr, no meaningful cutoff could be determined.
Figure 1: AUC: area under curve
Similarly, the ROC analysis for PI and SI at 6 hours was conducted to assess their prognostic utility. The AUC for PI_6hr was 0.744 (95% CI: 0.676 – 0.812, p < 0.001), indicating moderate predictive accuracy. In contrast, the AUC for SI_6hr was 0.428 (95% CI: 0.345 – 0.512, p = 0.068), which remains below 0.5, suggesting poor discrimination and limited clinical utility for mortality prediction. (Figure 2)
Figure 2: AUC curve at 6 hours
4. DISCUSSION
In this prospective observational study of the pulse oximetry-derived perfusion index, which included all patients admitted to the pediatric ICU during the study period, two major conclusions were drawn. First, the prognostic value of PI was demonstrated through the association of an initially low PI and failure to respond to resuscitative measures with high mortality. The second observation was the detection of occult shock using PI when clinical signs of shock were not present. In this study, 47% of patients had a low perfusion index on admission; improvement in the perfusion index was observed over time with treatment, and high mortality was noted in children with a low perfusion index at baseline and a persistently low PI after treatment. PI enhances the accuracy of hemodynamic assessment and perfusion status evaluation; its non-invasive nature makes it a convenient tool for continuous assessment of tissue perfusion and microcirculatory status.14
Clinical studies in pediatric shock have assessed the correlation of PI with signs of peripheral perfusion such as capillary refill time, hemodynamic variables such as heart rate and blood pressure, and biochemical signs of shock such as lactate levels.15 Talay et al. (2023), reported a significant correlation of PI with capillary refill time (P < 0.05) in children with shock.16 Similarly, there was also a good correlation between PI and heart rate as well as systolic blood pressure in the reports of Sivaprasath et al. (2019),17 and Ullah et al.(2021).15 PI has emerged as a useful parameter in the early recognition of shock and monitoring response to therapy in critically ill children, especially in resource-constrained settings. It has been widely used in many acute care settings, including emergency rooms, anesthesia, intensive care units, and trauma care.18 Kockan et al. compared PI with age-specific SI and demonstrated that non-survivors had significantly lower perfusion index (PI) values and higher average shock index (ASI) compared to survivors. 19
Alakaya et al. reported that PI is a valuable parameter to predict mortality in patients admitted in pediatric intensive care units. In their study, the specificity and sensitivity of low PI for mortality among 372 critically ill children were 90.1% and 75.9% respectively. 5 Published reports have demonstrated a direct correlation between low PI and mortality, identifying it as a prognostic marker in children admitted to PICU with variable values of sensitivity, specificity and area under the curve.6,20 A secondary analysis of a multicenter study in children with severe malaria showed low admission PI associated with two-fold greater odds of in-hospital mortality (OR, 2.44 [1.02–5.88]; P = 0.045) and a sensitivity and specificity of 51.4% and 63.4%, respectively for mortality. 1
There is no consensus on normal and pathological values of PI in children of different ages. The optimal cut-off of mean PI on admission in PICU was 0.91 for prediction of mortality in critically ill children in this study. However, Lalitha et al. observed a critical PI of <0.6 in their study including 50% of children with septic shock, and found a 42% improvement in PI at 6 hours.13 The sensitivity of a low PI for predicting mortality decreased from 76% at baseline to 45% indicating a lower ability to correctly identify non-survivors at 0-hour compared to the 6-hours measurements respectively. However, specificity improved significantly from 64% to 87, suggesting a stronger ability to correctly classify survivors. The negative predictive value remained relatively consistent over time, indicating PI as a strong predictor of survival supporting its use for risk stratification in pediatric sepsis.
The ROC analysis in our study indicated that PI AUC of 0.75 at 1 and 0.74 at 6 hours helps in predicting mortality among children with sepsis. This suggests that PI measurement at the thresholds used (low <1.0, normal ≥1.0) can provide a fair indication of mortality risk, with low PI values being moderately associated with higher likelihood of mortality compared to normal PI values. Mortality was notably higher in patients with low PI at 6 hours with 58.5%, who did not survive, compared to 19.9% in the normal PI group. These findings suggest that persistent low PI at 6 hours is strongly associated with critical illness, increased severity, and a significantly higher risk of mortality in pediatric sepsis.
The prospective design of this study, including a wide spectrum of clinical diagnoses in critically ill patients, strengthens its findings and highlights the perfusion index as a valuable tool for hemodynamic assessment and outcome prediction in the PICU. However, the moderate AUC value of PI indicates that it may not fully predict the outcome on its own and should ideally be used as an adjunct to other clinical indicators.
5. LIMITATIONS
This study has several limitations, including a relatively small sample size, its single-center design, arbitrary time points for measurements, and the inclusion of a wide range of age groups. These factors may influence the generalizability of the findings and warrant further multicenter studies with standardized protocols to validate the results. This study did not include a comparison of the perfusion index with other peripheral tissue perfusion indicators, such as capillary refill time, core-to-peripheral temperature gradient, or mottling score, nor with established disease severity scores as outcome predictors. Incorporating these comparisons could have further strengthened the findings and underscored the perfusion index as a valuable adjunct in critical care assessment.
6. CONCLUSION
Almost half of the children had a low PI on admission to the PICU, and one-quarter failed to improve after therapeutic interventions. Low PI at admission and after resuscitation were strong predictors of mortality. A large, multicenter prospective study with well-defined PI reference values for children of different ages admitted to the PICU is needed.
- Acknowledgements
- Conflict of interest
- Funding
- Authors’ contribution
11. REFERENCES
- Boland W, Datta D, Namazzi R, Bond C, Conroy AL, Mellencamp KA, et al. Peripheral Perfusion Index in Ugandan Children With Plasmodium falciparum Severe Malaria: Secondary Analysis of Outcomes in a 2014–2017 Cohort Study. Pediatr Crit Care Med. 2024;25(12):1117–26. PMCID: PMC11617272 DOI: 1097/PCC.0000000000003624
- Salluh JIF, Burghi G, Haniffa R. Intensive care for COVID-19 in low- and middle-income countries: research opportunities and challenges. Intensive Care Medicine. 2021;47(2):226-9. PMCID: PMC7661330 DOI: 1007/s00134-020-06285-y
- Talay MN, Orhan Ö. Using Perfusion Index and Clinical Follow-ups in Pediatric Intensive Care Unit. J Biotechnol Strateg Health Res. 2023;7(4):249–57.
- Coutrot M, Dudoignon E, Joachim J, Gayat E, Vallee F, Depret F. Perfusion index: physical principles, physiological meanings and clinical implications in anaesthesia and critical care. Anaesth Crit Care Pain Med. 2021;40(6):100964.DOI: 1016/j.accpm.2021.100964
- Alakaya M, Arslankoylu AE, Erdogan S. The usefulness of perfusion index for predicting mortality in pediatric intensive care unit. J Pediatr Emerg Intensive Care Med. 2022;9(2):123–9. doi:10.4274/cayd.galenos.2022.87609
- Bazaraa H, Roby S, Salah E, Algebaly H. Assessment of tissue perfusion using the peripheral perfusion index and lactate clearance in shock in pediatric patients. Shock Augusta Ga. 2021;56(6):933–8.
- Mongkolpun W, Orbegozo D, Cordeiro CP, Franco CJ, Vincent JL, Creteur J. Alterations in skin blood flow at the fingertip are related to mortality in patients with circulatory shock. Crit Care Med. 2020;48(4):443–50. DOI: 1097/CCM.0000000000004177
- Daş M, Bardakci O, Siddikoglu D, Akdur G, Yilmaz MC, Akdur O, et al. Prognostic performance of peripheral perfusion index and shock index combined with ESI to predict hospital outcome. Am J Emerg Med. 2020;38(10):2055–9. DOI: 1016/j.ajem.2020.06.084
- Shi X, Xu M, Yu X, Lu Y. Peripheral perfusion index predicting prolonged ICU stay earlier and better than lactate in surgical patients: an observational study. BMC Anesthesiol. 2020;20(1):153. PMCID: PMC7301460 DOI: 1186/s12871-020-01072-0
- Rao SV, Kandasamy S. Peripheral Perfusion Index for Prediction of Fluid Responsiveness in Spontaneously Breathing Critically Ill Patients: A Prospective Observational Study. Indian Journal of Critical Care Medicine. 2025;29(2):151-4 PMCID: PMC11915433 DOI: 5005/jp-journals-10071-24898
- Hu X jing, Ding J xiang, Wang Y, Niu C, Zhang Y, Zhao Q ming, et al. Peripheral perfusion index percentiles for healthy newborns by gestational age and sex in China. Sci Rep. 2020;10(1):4213. PMCID: PMC7060175 DOI: 1038/s41598-020-60741-9
- Koreti S, Gaur A. Role of perfusion index as a prognostic indicator in pediatric critical care. International Journal of Medicine & Public Health. 2025;15(2).
- Av L, Kuzhikkombil Mani S, Ghosh S. Perfusion index variations in children with septic shock: single-center observational cohort study in India. Pediatr Crit Care Med. 2024;25(1):47–53. DOI: 1097/PCC.0000000000003348
- Ismail J, Sankar J. Peripheral Perfusion Index – Magic Wand in Prediction of Shock? Indian J Pediatr. 2019 Oct;86(10):879–80. DOI: 1007/s12098-019-03028-w
- Allah M, Biswas S, Islam MS, Hossain M, Chowdhury MJBA, Chowdhury R, et al. Peripheral Perfusion Index in Assessment of Shock in Paediatric Intensive Care Unit of A Tertiary Care Hospital. IAHS Med J. 2021;4(2):46–50. DOI: https://doi.org/10.3329/iahsmj.v4i2.62525
- Talay MN, Orhan Ö. Çocuk Yoğun Bakım Ünitesi’nde Perfüzyon İndeksi Kullanımı ve Klinik İzlemleri. J Biotechnol Strateg Health Res. 2023;7(4):249–57.
- Sivaprasath P, Mookka Gounder R, Mythili B. Prediction of shock by peripheral perfusion index. Indian J Pediatr. 2019;86:903–8. DOI: 1007/s12098-019-02993-6
- Alakaya M, Arslanköylü AE. Evaluation of perfusion index in pediatric trauma patients. Turk J Trauma Emerg Surg. 2022;28(5):593. PMCID: PMC10442984 DOI: 14744/tjtes.2021.68145
- Koçkan BS, Doğan S, Kalafat AFB, Fettahoğlu S, Guner M, Avcu V, et al. Correlation Between Age Shock Index and Perfusion Index with Emergency Severity Index and its Predictive Value on In-hospital Mortality. Glob Emerg Crit Care 2023;2(2):41-46 DOI: 10.4274/globecc.galenos.2023.25743
- Hamade B, Bayram JD, Hsieh YH, Khishfe B, Al Jalbout N. Modified Shock Index as a Predictor of Admission and In-hospital Mortality in Emergency Departments; an Analysis of a US National Database. Arch Acad Emerg Med. 2023;11(1):e34. PMCID: PMC10197905 DOI: 22037/aaem.v11i1.1901