Salman Yahya 1 , Sonia Zafar 2 , Sher Mohammad 3
Author affiliations:
During the past few decades, the healthcare provision has rapidly evolved into a multidimensional task, involving not only the clinical specialists, but also a host of other fields, including information technology, continuous professional training, medical engineering, supply chain management, and counseling sections. A sound interplay of all these is crucial to the satisfaction of the patients as well as their family members. Here comes the concept of ‘clinical governance’, which has evolved into a super-specialty in its own right.
Keywords: Clinical governance; Clinical specialties; Healthcare;
Citation: Yahya S, Zafar S, Mohammad S. Clinical governance: from framework to culture (Editorial).Anaesth. pain intensive care 2025;29(7):653-655. DOI: 10.35975/apic.v29i7.2949
Received: June 25, 2025; Revised: July 10, 2025; Accepted: July 20, 2025
The delivery of safe, effective, and patient-centered care is the primary concept of modern healthcare systems. Achieving and sustaining these standards requires not only clinical expertise but also structured accountability, leadership, and a culture of continuous improvement. The concept of clinical governance—first introduced in the United Kingdom in 1998—provides such a framework. It was envisioned as a systematic approach through which healthcare organizations could be held responsible for quality, safety, and patient outcomes, ensuring that clinical excellence was not left to chance but embedded in the daily delivery of care.1
In the decades since its inception, clinical governance has been widely recognized and adapted across healthcare systems worldwide. Yet, its promise has not always been fully realized. While some organizations have embedded clinical governance as a culture of learning and improvement, others have struggled to move beyond bureaucratic compliance. This editorial explores the evolution of clinical governance, its key elements, challenges in implementation, and its future projection.
Clinical governance emerged in response to a series of healthcare scandals in the United Kingdom during the 1990s, including the events at Bristol Royal Infirmary, which exposed systemic failures in accountability and patient safety.2 In its White Paper A First Class Service, the UK Department of Health formalized the concept, declaring that organizations must take responsibility for continuously improving the quality of services.3 This was a key moment: for the first time, quality was placed on equal footing with financial and operational performance.
The model integrated several pre-existing mechanisms—clinical audit, risk management, evidence-based medicine, continuing professional development, and patient involvement—into a single framework. Importantly, it shifted responsibility from individual clinicians to organizations, emphasizing collective accountability.4
Over time, the principles of clinical governance have transcended the NHS and influenced global health policy. The World Health Organization now promotes quality of care as a central pillar of universal health coverage, aligning closely with the ethos of clinical governance.5
The concept of clinical governance is commonly explained around seven interdependent pillars.6
1. Clinical Effectiveness – integrating best available evidence into practice to ensure effective care.
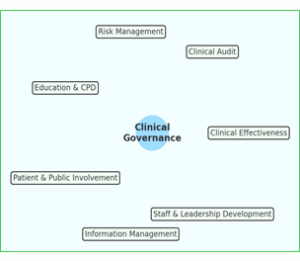
Figure 1: Seven pillars of clinical governance
Among those 7 pillars, patient safety is of utmost importance. Healthcare is inherently complex and error-prone. Reason’s “Swiss Cheese Model” illustrates how latent system failures align with active errors to produce harm.7 Clinical governance provides the structures to mitigate these risks—incident reporting systems, root cause analyses, and safety protocols.
The consequences of governance failures are stark. The Mid Staffordshire NHS Trust scandal revealed how an overemphasis on financial targets and organizational image could result in neglect, suffering, and avoidable harm.8 The subsequent Francis Inquiry underscored that governance must prioritize patients above all else, and that safety and compassion are inseparable from quality.
While systems and processes are essential, clinical governance succeeds or fails on the basis of culture. Dixon-Woods et al..9] demonstrated that lasting improvement depends on fostering cultures of trust, openness, and collective responsibility. Leadership is extremely important and plays a key role in this process. In cultures dominated by blame, errors are concealed, and learning opportunities are lost. By contrast, organizations that promote psychological safety encourage staff to report concerns and participate in improvement initiatives. Leaders must therefore do more than enforce compliance; they must model values of integrity, openness, and patient-centeredness.
Another distinguishing feature of clinical governance is its explicit emphasis on patient and public involvement. This represents a paradigm shift from paternalism to partnership. Coulter.10] highlights that patients’ perspectives are vital indicators of quality, and their input must inform both service delivery and system governance. Shared decision making and the informed consent process play a vital role in patient involvement and in developing their confidence in the care they receive from healthcare professionals.
Meaningful engagement includes patient representation on committees, co-design of services, and systematic integration of patient-reported outcomes. Involving patients not only enhances quality but also restores trust, particularly in systems where confidence has been eroded by failures.
Despite its conceptual clarity, clinical governance faces enduring challenges:
Healthcare is evolving rapidly, and clinical governance must adapt to remain relevant. Several emerging themes warrant attention:
Clinical governance remains one of the most significant innovations in healthcare quality policy. By integrating structures, processes, and culture, it provides a framework for accountability and improvement. Its success, however, depends less on compliance with procedures and more on genuine cultural commitment to patient safety and quality.
For clinicians, managers, and policymakers alike, the challenge is to ensure that governance is not experienced as bureaucracy but as a shared commitment to better care. Leadership must foster openness, empower staff, and involve patients meaningfully in shaping services. Only by moving beyond frameworks to culture can clinical governance fulfil its promise: safeguarding the trust upon which all healthcare systems depend.
10. Conflicts of interest
None declared by the authors/
11. Authors’ contribution
All authors took part in the concept, literature search, and manuscript preparation.
Author affiliations:
- Salman Yahya, Consultant Anesthetist, North West Anglia NHS Foundation Trust, UK.
- Sonia Zafar, Trust Grade Doctor (Core Trainee), General Medicine, York and Scarborough Teaching Hospitals, NHS Foundation Trust, UK.
- Sher Mohammad, Consultant Anesthetist (Retired), Sheffield Teaching Hospitals NHS Foundation Trust, UK
ABSTRACT
During the past few decades, the healthcare provision has rapidly evolved into a multidimensional task, involving not only the clinical specialists, but also a host of other fields, including information technology, continuous professional training, medical engineering, supply chain management, and counseling sections. A sound interplay of all these is crucial to the satisfaction of the patients as well as their family members. Here comes the concept of ‘clinical governance’, which has evolved into a super-specialty in its own right.
Keywords: Clinical governance; Clinical specialties; Healthcare;
Citation: Yahya S, Zafar S, Mohammad S. Clinical governance: from framework to culture (Editorial).Anaesth. pain intensive care 2025;29(7):653-655. DOI: 10.35975/apic.v29i7.2949
Received: June 25, 2025; Revised: July 10, 2025; Accepted: July 20, 2025
1. INTRODUCTION
The delivery of safe, effective, and patient-centered care is the primary concept of modern healthcare systems. Achieving and sustaining these standards requires not only clinical expertise but also structured accountability, leadership, and a culture of continuous improvement. The concept of clinical governance—first introduced in the United Kingdom in 1998—provides such a framework. It was envisioned as a systematic approach through which healthcare organizations could be held responsible for quality, safety, and patient outcomes, ensuring that clinical excellence was not left to chance but embedded in the daily delivery of care.1
In the decades since its inception, clinical governance has been widely recognized and adapted across healthcare systems worldwide. Yet, its promise has not always been fully realized. While some organizations have embedded clinical governance as a culture of learning and improvement, others have struggled to move beyond bureaucratic compliance. This editorial explores the evolution of clinical governance, its key elements, challenges in implementation, and its future projection.
2. ORIGINS AND EVOLUTION
Clinical governance emerged in response to a series of healthcare scandals in the United Kingdom during the 1990s, including the events at Bristol Royal Infirmary, which exposed systemic failures in accountability and patient safety.2 In its White Paper A First Class Service, the UK Department of Health formalized the concept, declaring that organizations must take responsibility for continuously improving the quality of services.3 This was a key moment: for the first time, quality was placed on equal footing with financial and operational performance.
The model integrated several pre-existing mechanisms—clinical audit, risk management, evidence-based medicine, continuing professional development, and patient involvement—into a single framework. Importantly, it shifted responsibility from individual clinicians to organizations, emphasizing collective accountability.4
Over time, the principles of clinical governance have transcended the NHS and influenced global health policy. The World Health Organization now promotes quality of care as a central pillar of universal health coverage, aligning closely with the ethos of clinical governance.5
3. The Pillars of Clinical Governance
The concept of clinical governance is commonly explained around seven interdependent pillars.6
1. Clinical Effectiveness – integrating best available evidence into practice to ensure effective care.
- Clinical Audit – systematically evaluating care against standards and implementing improvements.
- Risk Management – identifying, assessing, and reducing risks to patient safety.
- Education, Training, and Continuous Professional Development – ensuring the workforce remains skilled and competent.
- Patient and Public Involvement – involving patients as partners in care planning and evaluation.
- Information Management – collecting and using data to support decision-making and transparency.
- Staff and Leadership Development – facilitating supportive environments that encourage innovation and accountability.
Figure 1: Seven pillars of clinical governance
4. Patient safety as the cornerstone
Among those 7 pillars, patient safety is of utmost importance. Healthcare is inherently complex and error-prone. Reason’s “Swiss Cheese Model” illustrates how latent system failures align with active errors to produce harm.7 Clinical governance provides the structures to mitigate these risks—incident reporting systems, root cause analyses, and safety protocols.
The consequences of governance failures are stark. The Mid Staffordshire NHS Trust scandal revealed how an overemphasis on financial targets and organizational image could result in neglect, suffering, and avoidable harm.8 The subsequent Francis Inquiry underscored that governance must prioritize patients above all else, and that safety and compassion are inseparable from quality.
5. Leadership and Organizational Culture
While systems and processes are essential, clinical governance succeeds or fails on the basis of culture. Dixon-Woods et al..9] demonstrated that lasting improvement depends on fostering cultures of trust, openness, and collective responsibility. Leadership is extremely important and plays a key role in this process. In cultures dominated by blame, errors are concealed, and learning opportunities are lost. By contrast, organizations that promote psychological safety encourage staff to report concerns and participate in improvement initiatives. Leaders must therefore do more than enforce compliance; they must model values of integrity, openness, and patient-centeredness.
6. The Role of Patients and the Public
Another distinguishing feature of clinical governance is its explicit emphasis on patient and public involvement. This represents a paradigm shift from paternalism to partnership. Coulter.10] highlights that patients’ perspectives are vital indicators of quality, and their input must inform both service delivery and system governance. Shared decision making and the informed consent process play a vital role in patient involvement and in developing their confidence in the care they receive from healthcare professionals.
Meaningful engagement includes patient representation on committees, co-design of services, and systematic integration of patient-reported outcomes. Involving patients not only enhances quality but also restores trust, particularly in systems where confidence has been eroded by failures.
7. Challenges in Implementation
Despite its conceptual clarity, clinical governance faces enduring challenges:
- Resource Constraints – Workforce shortages, financial pressures, and increasing patient demand can undermine governance initiatives..11
- Bureaucratization – In some settings, governance degenerates into paperwork and compliance, detached from clinical reality.
- Variability in Application – Differences in leadership, organizational culture, and resources lead to inconsistent implementation.
4. Balancing Accountability and Learning – Achieving the right balance between holding staff accountable and fostering a no-blame culture remains a persistent tension.
8. The Future of Clinical Governance
Healthcare is evolving rapidly, and clinical governance must adapt to remain relevant. Several emerging themes warrant attention:
- Digital Transformation – The rise of electronic health records, artificial intelligence, and real-time analytics presents new opportunities for evidence-based care, proactive risk management, and performance monitoring.12
- Global Harmonization – Increasing alignment of governance frameworks across countries can facilitate benchmarking and shared learning.
- Equity and Inclusion – Governance must address disparities in care, ensuring that improvements benefit all patients, regardless of socio-economic or demographic factors.
- Sustainability and Resilience – In the context of climate change, pandemics, and global crises, governance must support not only immediate safety but also long-term resilience.5
9. CONCLUSION
Clinical governance remains one of the most significant innovations in healthcare quality policy. By integrating structures, processes, and culture, it provides a framework for accountability and improvement. Its success, however, depends less on compliance with procedures and more on genuine cultural commitment to patient safety and quality.
For clinicians, managers, and policymakers alike, the challenge is to ensure that governance is not experienced as bureaucracy but as a shared commitment to better care. Leadership must foster openness, empower staff, and involve patients meaningfully in shaping services. Only by moving beyond frameworks to culture can clinical governance fulfil its promise: safeguarding the trust upon which all healthcare systems depend.
10. Conflicts of interest
None declared by the authors/
11. Authors’ contribution
All authors took part in the concept, literature search, and manuscript preparation.
REFERENCES
- Scally G, Donaldson LJ. Clinical governance and the drive for quality improvement in the new NHS in England. 1998;317(7150):61–65. DOI: 10.1136/bmj.317.7150.61 PubMed PMC1113460
- Halligan A, Donaldson L. Implementing clinical governance: turning vision into reality. 2001;322(7299):1413–1417. PMCID: PMC1120478 DOI: 10.1136/bmj.322.7299.1413
- Department of Health. A First Class Service: Quality in the new NHS. London: HMSO; 1998.
- Smith J. Review of NHS Efficiency and Productivity. London: Department of Health; 2012.
- World Health Organization. Quality health services: a planning guide. Geneva: WHO; 2021.
- Halligan A. The seven pillars of clinical governance. Hosp Med. 1999;60(10):707–712.
- Reason J. Human error: models and management. 2000;320(7237):768–770. PMCID: PMC1117770 DOI: 10.1136/bmj.320.7237.768
- Francis R. Report of the Mid Staffordshire NHS Foundation Trust Public Inquiry. London: The Stationery Office; 2013.
- Dixon‑Woods M, Baker R, Charles K, Dawson J, Jerzembek G, Martin G, et al. Culture and behaviour in the English National Health Service: overview of lessons from a large multimethod study. BMJ Qual Saf. 2014;23(2):106–115. DOI: 1007/s00268-013-2397-7
- Coulter A. The Autonomous Patient: Ending Paternalism in Medical Care. London: Nuffield Trust; 2002.
- Ham C. Health policy in Britain. 6th ed. Basingstoke: Palgrave Macmillan; 2009.
- Topol E. The Creative Destruction of Medicine: How the Digital Revolution Will Create Better Health Care. New York: Basic Books; 2012.