Nazmy Edward Seif 1, Kamel Salama Salem 2, Ahmed Ali Gado 3, Victor Farouk Jaccoub 4*
Authors affliations:
Background & objective: Upper abdominal surgery has been known to adversely affect the respiratory activity of pediatric patients due to the significant postoperative pain. We aimed to assess the efficacy of erector spinae plane block in addition to general anesthesia (GA) in such surgeries and its role in improving the analgesia and outcomes in children.
Methodology: A randomized controlled study was conducted on 40 pediatric patients scheduled for elective open upper abdominal surgeries, such as open cholecystectomy, splenectomy, or operations on the kidneys as pyeloplasty, cyst excision & partial or total nephrectomy at Abo-Elreesh Hospital, Cairo, from November 2020 to November 2022. The patients were equally divided into Group C, which received GA, with no block, and Group E, which received erector spinae plane block (ESPB) after GA. Hemodynamics were recorded intraoperative and up to 1 hour postoperatively. Analgesic quality and respiratory dynamics were assessed postoperatively.
Results: Total postoperative tramadol consumption was significantly reduced in Group E (21.3 ± 11.7) compared to Group C (71.7 ± 19.7), P < 0.001. HR values during the procedure and up to 1 hour after surgery were significantly decreased by the ESPB (P < 0.001). Respiratory activity parameters (rate, depth, and oxygen saturation) were significantly improved in Group E (P < 0.001).
Conclusion: ESPB decreased intraoperative nociception and improved the postoperative analgesia, which resulted in better respiratory activity with fewer requirements for oxygen supplements.
Research clinical trial registration number: NCT04518215
Abbreviations: ESPB: erector spinae plane block, ESM: erector spinae muscle, GA: general anesthesia, HR: heart rate, MAP: mean arterial pressure, PACU: post-anesthesia care unit, FLACC: Face, Leg, Activity, Cry, Consolability
Keywords: erector; spinae; pediatric; block; abdominal; surgery
Citation: Seif NE, Salem AKS, Gado AAM, Jaccoub VF. Ultrasound-guided erector spinae plane block for pediatric upper abdominal surgery: a randomized controlled study. Anaesth. pain intensive care 2025;29(7):663-669. DOI: 10.35975/apic.v29i7.2942
Received: April 17, 2025; Revised: September 02, 2024; Accepted: September 10, 2025
Open cholecystectomy, splenectomy, or procedures affecting the kidney, such as pyeloplasty, cyst excision, and partial or complete nephrectomy, are among the upper abdominal operations performed on children. Achieving an acceptable degree of analgesia, maintaining free respiratory muscle strength, and early patient movement are critical elements of perioperative care. These surgeries are typically accompanied by considerable postoperative pain.1
Despite significant improvements in the prevention and treatment of known complications of upper abdominal surgery, morbidity remains 20% to 25% or greater, as described by Celli BR et al. (1984).2 All patients who undergo major surgical procedures in the upper abdomen are at risk of postoperative respiratory limitation due to atelectasis that results from pain.2
Intraoperatively, both the anesthetic and the surgical techniques cause physiologic changes. These changes persist in the post-operative period, as a result of lingering effects from the anesthesia, narcotics, and surgery, as well as pain-related restricted expansion of the lungs or the chest wall, respiratory muscle dysfunction, abnormal respiratory drive, and abnormal respiratory muscle function brought on by surgery on the upper abdomen.3 As the incision site is close to the diaphragm, hypoxia is common in these types of surgeries.4
Opioid analgesics are widely prescribed for the management of moderate to severe postoperative pain. However, nausea, vomiting, sedation, and respiratory depression can be very troublesome side effects.5
The first effective report of the erector spinae plane block (ESPB) application was in 2016, when it was utilised to treat thoracic neuropathic pain in a patient with metastatic rib disease and rib fractures. Since then, a variety of surgeries, including thoracotomies, percutaneous nephrolithotomies, ventral hernia repairs, and even lumbar fusions, have been reported to have successfully utilised the block. Since this process is still in its early stages of development, multiple prospective studies and ESPB trials are continuing.6
In our trial, the analgesic value of intraoperative ESPB was evaluated. We hypothesized that it could improve the perioperative analgesia, decrease the opioid consumption after surgery (our primary outcome), which could enhance the respiratory activity after surgery.
A randomized controlled study was conducted at Abo-Elreesh Hospital, Cairo, from November 2020 to November 2022 on 40 pediatric patients of both sexes, aged between 2-12 years, and scheduled for elective open upper abdominal surgeries, such as open cholecystectomy, splenectomy, or operations on the kidneys as pyeloplasty, cyst excision & partial or total nephrectomy. The study was conducted after receiving approval from Cairo University Hospitals' research and ethics committee (Approval No. N-96-2020). Written informed consent was obtained from the parents. The trial was registered with clinicaltrials.gov with ID: NCT04518215. Exclusion criteria were parents' refusal, allergy to local anesthetics, or infection at the site of injection or coagulopathy.
Randomization was done using a computer-generated sequence. Concealment was achieved by the use of opaque envelopes placed in the operating room, and only opened at the patients’ arrival. Patients were randomized to receive conventional general anesthesia with no block (Group C) or general anesthesia plus ESPB using a local anesthetic (Group E).
The parents didn’t know the group of their kids. The anesthetic induction and block performance were achieved by the anesthetists not involved in the anesthetic management or postoperative outcome assessment. The intraoperative management and data collection were recorded by anesthetists, who were allowed to enter the operating room after a considerable time from induction so as not to know the group assignment.
Standard monitoring devices were attached, and baseline measurements of the heart rate (HR), mean arterial blood pressure (MAP), and oxygen saturation (SpO2) were noted. Atropine 0.01 mg/kg was administered intravenously after an intravenous line was established to induce general anesthesia in both groups using 8% sevoflurane in 100% oxygen.
Inj. atracurium 0.5 mg/kg IV and fentanyl 2 µg/kg were used as a muscle relaxant for endotracheal intubation using a cuffed endotracheal tube of the appropriate size.
Patients were assigned to either Group C (control group) to receive a general anesthetic with no block, or to Group E (block group) to receive a general anesthetic plus ESPB.
The block was performed at the level of T9–10 with the patient lying prone. A high-frequency linear ultrasound probe was positioned 1-2 cm laterally to the midline at the T9 level after skin disinfection with 10% Povidone Iodine. A 22 G needle was placed using an in-plane approach deep within the erector spinae muscle (ESM) after the transverse process and the erector spinae muscle had been identified. The delivery of 0.5–1 mL of normal saline allowed researchers to see the hydro-dissection between the transverse process and the ESM, confirming that the needle placement was accurate.
For unilateral ESPB, deep injections of 0.25% bupivacaine in a calculated volume of 0.5 mL/kg (with a maximum dose of 20 mL) were made into the ESM in accordance with the planned aspect of the operation.
The perioperative anesthetic care was carried out by the anesthetists blinded to the study groups. Sevoflurane 2% in 50% oxygen and air, atracurium 0.1 mg/kg every 15 to 25 minutes, were used to maintain anesthesia. Hemodynamic variables were monitored every 5 minutes; additional boluses of 1 g/kg fentanyl were administered when the HR or MAP rose above 20% of the baseline. All patients received 15 mg/kg of paracetamol for postoperative analgesia at the conclusion of the procedure, and they were all extubated once the residual effects of the muscle relaxants were abolished by atropine 0.02 mg/kg and neostigmine 0.05 mg/kg, and full muscle power and consciousness had been restored.
Hemodynamic variables were monitored every 15 minutes in the post-anesthesia care unit (PACU) up to 1 hour after surgery. As soon as a patient recovered in the PACU, the pain was first evaluated by FLACC (Face, Leg, Activity, Cry, Consolability) pain scale.7 The scale has a range of 0 to 10, with 0 denoting no pain and 10 denoting the most intense agony, and was assessed and recorded at 0 h (in PACU), then at 2, 4, 6, 9, 12, 18, and 24 h after surgery. Inj. paracetamol 15 mg/kg IV was given every 8 hours for standard postoperative analgesia. The time from extubation to the first complaint of pain with FLACC ≥ 4 was documented as the time to first analgesic request, and 1 mg/kg tramadol IV was given. At 6 months after surgery, the presence of painful sensation at the site of surgery was evaluated by a telephone call by an investigator who was blinded to group allocation.
The primary outcome was the total postoperative tramadol dose; secondary outcomes included perioperative HR and MAP values, total quantities of intraoperative fentanyl, first post-operative time moving around, hospital stay, and any adverse effects. Also, postoperative oxygen saturation, respiratory rate, depth of breathing, and the need for oxygen supplementation were observed.
G-power 3.1 software was used to conduct a power analysis. The primary outcome variable in the current study was the total amount of narcotic (tramadol) usage on the first day after surgery. We conducted a pilot study (7 patients) in each group, which revealed a mean of tramadol in Group C as 50.3 ± 26 mg versus 25.4 ± 14 mg in Group E. With a power of study of 90%, two two-tailed t-test, with an alpha value of 0.05, a sample of 40 patients was revealed after adding 20% for possible dropouts.
Statistical analysis
Data were fed to the computer and analysed using IBM SPSS software package version 20.0. (Armonk, NY: IBM Corp). Categorical data were represented as numbers and percentages. Chi-square test was applied to compare different groups. Alternatively, the Monte Carlo correction test was applied when more than 20% of the cells had expected counts less than 5. For continuous data, they were tested for normality by the Shapiro-Wilk test. Quantitative data are expressed as mean and standard deviation or median (range). Student t-test was used to compare two groups for normally distributed quantitative variables. On the other hand, Mann Whitney test was used to compare two groups for not normally distributed quantitative variables. Significance of the obtained results was judged at the 5% level.
The eligibility of 96 pediatric patients was assessed; 36 patients didn’t fulfill the inclusion criteria, and 20 patients or their parents refused to participate in this study. The remaining 40 patients were randomly and equally divided into Group E and Group C. All patients were followed up, and their data were analyzed without dropouts.
According to the demographic data, there was no significant difference between the groups related to their age, weight, gender or type or duration of surgery (Table 1).
Regarding perioperative hemodynamics, the vital signs between the groups were compared; Group E showed a significant reduction in heart rate during surgery and up to 1 hour after surgery (P < 0.001) (Figure 1). However, MAP values were significantly decreased in Group E than in Group C at 35, 55, 65, 70, and 75 minutes intraoperative and postoperative time points (P < 0.05) (Figure 2).
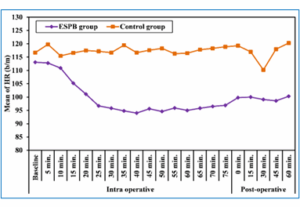
Figure 1: Comparative mean heart rates in the two studied groups
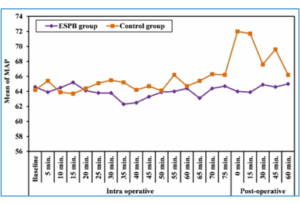
Figure 2: Comparative MAP in the two studied groups
Postoperative FLACC pain scores were significantly decreased in Group E, as compared to Group C at all assessment points except at 12 h and 18 h after surgery, as shown in Table 2.
Intraoperative fentanyl consumption was significantly reduced in Group E 2.80 ± 6.85 µg compared to the Group C 20 ± 4.87 µg, (P < 0.001). Total postoperative tramadol consumption (primary outcome) was significantly reduced in Group E compared to Group C (P < 0.001). Time to first request of postoperative analgesia was significantly reduced in Group E compared to Group C (P < 0.001), as can be seen in Table 3.
The impact of improved analgesic quality in Group E was reflected by the significantly earlier time to ambulate (P < 0.001), shorter hospital stays (P < 0.001), and lower incidence of chronic pain at 6 months after surgery (P = 0.02) as shown in Table 3.
Also, the respiratory muscle activity was significantly better in Group E as evidenced by the higher postoperative oxygen saturation values on room air in PACU, a lower number of patients requiring oxygen supplementation, lower respiratory rate values, with more patients achieving an adequate depth of breathing (P < 0.001) (Table 3).
Most of the patients undergoing major upper abdominal surgery run the risk of postoperative breathing problems due to atelectasis brought upon by pain. Open cholecystectomy, splenectomy, or procedures involving the kidneys, such as pyeloplasty, cyst excision, or partial or complete nephrectomy, are among the upper abdominal operations commonly undertaken in children. These surgeries are typically accompanied by considerable postoperative pain. Achieving adequate analgesia, maintaining respiratory muscle strength, and early patient mobilization are critical elements of perioperative care.
Anesthesia and the surgical procedure both cause physiological changes. Due to the effects of the anesthetic drugs, surgery, as well as the impact of pain, causing lung or chest wall restriction, respiratory muscle dysfunction, etc., these physiologic alterations continue in the post-operative period.
The most widely prescribed medications for the management of moderate to severe postoperative pain are opioid analgesics. Respiratory depression is frequently caused by opioid overdose, particularly when combined with longer-acting medications like morphine.
In our study, we substituted an ESPB for conventional analgesic methods. Our research demonstrated that ESPB was a successful pain management technique for children undergoing open upper abdominal surgery. It could be used in place of conventional analgesics with the satisfaction of the patients.
In the control group, the patients with FLACC scores of 4–7 necessitated postoperative supplementation with more analgesics. ESPB demonstrated satisfactory results of pain relief detected by low grading of FLACC scores (average 2-4) that did not require additional analgesic support.
The patients in the ESPB group had free respiratory muscle activity as evidenced by higher SpO2 levels and deeper respirations; whereas patients in the control group had lower oxygen saturations and required oxygen supplementation with shallower breathing that was primarily brought on by pain and basal lung atelectasis.
This was consistent with an earlier study performed by Forero et al. (2016), indicating that the ESPB may be a valuable therapeutic option in the management of post-thoracotomy pain syndrome (PTPS). Its immediate analgesic efficacy provides patients with temporary symptomatic relief while other aspects of chronic pain management are optimized, and it may also often confer prolonged analgesia.6
The results were also comparable with a meta-analysis for various surgeries performed by Yu Cui, et al. (2022), reporting that ESPB reduced the accumulated opioid consumption during the first 24 h after surgery. Besides, ESPB could prolong the time to first rescue analgesia after surgery.8
Kompal Jain, et al. (2018) conducted a study on a case series, proving the effectiveness of ESPB in pain reduction for conditions ranging from acute postoperative pain following breast, thoracotomy, and abdominal operations to chronic neuropathic pain.9
Viderman et al. (2022) performed a meta-analysis study that demonstrated that there were no reports of serious complications associated with ESPB for postoperative analgesia in adult abdominal surgery.10 Other studies confirmed the same results.11-14
Contrary to our findings, Heejoon et al. (2022) found that ESPB did not reduce overall fentanyl consumption in the first 24 hours following open gastrectomy and only lessened postoperative discomfort until three hours after surgery.15
There are some limitations to our study: First, the small sample size limits the generalizability of our findings. Second, we assessed oxygen saturation with color of the rate, and depth of respiratory excursion to assess the respiratory activity in our patients. Ultrasound-guided parameters like lung ultrasound score may be more reliable in assessing lung collapse after surgery. Although chronic pain incidence at 6 month was significantly lower in ESPB group, the small sample couldn’t power these findings. Finally, assessment of co-factors that determine pain chronicity like functional disability and anxiety scores could increase the global value of ESPB beyond its acute postoperative analgesic benefit.
ESPB decreased intraoperative nociception, improved the postoperative analgesia, and decreased opioid consumption after surgery, which resulted in better respiratory activity with fewer requirements for oxygen supplements.
7. Data availability
The data generated in this study are available upon request from the corresponding author.
8. Funding
No external funding or industry sponsorship was used in this study. The researchers used the university resources to complete the study.
9. Conflicts of interest
The authors declare that they had no conflicts of interest.
10. Authors' contributions
NES: Study concept and design, data collection and interpretation, drafting the manuscript and revising it, approved the final draft.
AKSS: Data collection and analysis, drafting the manuscript and revising it, approved the final draft.
AAMG: Data collection, interpretation, and analysis, drafted and revised the manuscript, approved the final draft.
VFJ: Study concept and design, data collection and interpretation, drafting the manuscript and revising it.
Authors affliations:
- Nazmy Edward Seif: Lecturer, Department of Anesthesiology, Surgical Intensive Care & Pain Management, Faculty of Medicine, Cairo University, Cairo, Egypt; Email: drnazmyseif@Kasralainy.edu.eg
- Atef Kamel Salama Salem: Lecturer, Department of Anesthesiology, Surgical Intensive Care & Pain Management, Faculty of Medicine, Cairo University, Cairo, Egypt; Email: atef.kamel@Kasralainy.edu.eg
- Ahmed Ali Mohamed Gado: Associate Professor, Department of Anesthesiology, Surgical Intensive Care & Pain Management, Faculty of Medicine, Cairo University, Cairo, Egypt; Email: Ahmed.Gado@Kasralainy.edu.eg
- Victor Farouk Jaccoub: Department of Anesthesiology, Surgical Intensive Care & Pain Management, Faculty of Medicine, Cairo University, Cairo, Egypt; Email: Dr.vfjacob@gmail.com
ABSTRACT
Background & objective: Upper abdominal surgery has been known to adversely affect the respiratory activity of pediatric patients due to the significant postoperative pain. We aimed to assess the efficacy of erector spinae plane block in addition to general anesthesia (GA) in such surgeries and its role in improving the analgesia and outcomes in children.
Methodology: A randomized controlled study was conducted on 40 pediatric patients scheduled for elective open upper abdominal surgeries, such as open cholecystectomy, splenectomy, or operations on the kidneys as pyeloplasty, cyst excision & partial or total nephrectomy at Abo-Elreesh Hospital, Cairo, from November 2020 to November 2022. The patients were equally divided into Group C, which received GA, with no block, and Group E, which received erector spinae plane block (ESPB) after GA. Hemodynamics were recorded intraoperative and up to 1 hour postoperatively. Analgesic quality and respiratory dynamics were assessed postoperatively.
Results: Total postoperative tramadol consumption was significantly reduced in Group E (21.3 ± 11.7) compared to Group C (71.7 ± 19.7), P < 0.001. HR values during the procedure and up to 1 hour after surgery were significantly decreased by the ESPB (P < 0.001). Respiratory activity parameters (rate, depth, and oxygen saturation) were significantly improved in Group E (P < 0.001).
Conclusion: ESPB decreased intraoperative nociception and improved the postoperative analgesia, which resulted in better respiratory activity with fewer requirements for oxygen supplements.
Research clinical trial registration number: NCT04518215
Abbreviations: ESPB: erector spinae plane block, ESM: erector spinae muscle, GA: general anesthesia, HR: heart rate, MAP: mean arterial pressure, PACU: post-anesthesia care unit, FLACC: Face, Leg, Activity, Cry, Consolability
Keywords: erector; spinae; pediatric; block; abdominal; surgery
Citation: Seif NE, Salem AKS, Gado AAM, Jaccoub VF. Ultrasound-guided erector spinae plane block for pediatric upper abdominal surgery: a randomized controlled study. Anaesth. pain intensive care 2025;29(7):663-669. DOI: 10.35975/apic.v29i7.2942
Received: April 17, 2025; Revised: September 02, 2024; Accepted: September 10, 2025
1. INTRODUCTION
Open cholecystectomy, splenectomy, or procedures affecting the kidney, such as pyeloplasty, cyst excision, and partial or complete nephrectomy, are among the upper abdominal operations performed on children. Achieving an acceptable degree of analgesia, maintaining free respiratory muscle strength, and early patient movement are critical elements of perioperative care. These surgeries are typically accompanied by considerable postoperative pain.1
Despite significant improvements in the prevention and treatment of known complications of upper abdominal surgery, morbidity remains 20% to 25% or greater, as described by Celli BR et al. (1984).2 All patients who undergo major surgical procedures in the upper abdomen are at risk of postoperative respiratory limitation due to atelectasis that results from pain.2
Intraoperatively, both the anesthetic and the surgical techniques cause physiologic changes. These changes persist in the post-operative period, as a result of lingering effects from the anesthesia, narcotics, and surgery, as well as pain-related restricted expansion of the lungs or the chest wall, respiratory muscle dysfunction, abnormal respiratory drive, and abnormal respiratory muscle function brought on by surgery on the upper abdomen.3 As the incision site is close to the diaphragm, hypoxia is common in these types of surgeries.4
Opioid analgesics are widely prescribed for the management of moderate to severe postoperative pain. However, nausea, vomiting, sedation, and respiratory depression can be very troublesome side effects.5
The first effective report of the erector spinae plane block (ESPB) application was in 2016, when it was utilised to treat thoracic neuropathic pain in a patient with metastatic rib disease and rib fractures. Since then, a variety of surgeries, including thoracotomies, percutaneous nephrolithotomies, ventral hernia repairs, and even lumbar fusions, have been reported to have successfully utilised the block. Since this process is still in its early stages of development, multiple prospective studies and ESPB trials are continuing.6
In our trial, the analgesic value of intraoperative ESPB was evaluated. We hypothesized that it could improve the perioperative analgesia, decrease the opioid consumption after surgery (our primary outcome), which could enhance the respiratory activity after surgery.
2. METHODOLOGY
A randomized controlled study was conducted at Abo-Elreesh Hospital, Cairo, from November 2020 to November 2022 on 40 pediatric patients of both sexes, aged between 2-12 years, and scheduled for elective open upper abdominal surgeries, such as open cholecystectomy, splenectomy, or operations on the kidneys as pyeloplasty, cyst excision & partial or total nephrectomy. The study was conducted after receiving approval from Cairo University Hospitals' research and ethics committee (Approval No. N-96-2020). Written informed consent was obtained from the parents. The trial was registered with clinicaltrials.gov with ID: NCT04518215. Exclusion criteria were parents' refusal, allergy to local anesthetics, or infection at the site of injection or coagulopathy.
Randomization was done using a computer-generated sequence. Concealment was achieved by the use of opaque envelopes placed in the operating room, and only opened at the patients’ arrival. Patients were randomized to receive conventional general anesthesia with no block (Group C) or general anesthesia plus ESPB using a local anesthetic (Group E).
The parents didn’t know the group of their kids. The anesthetic induction and block performance were achieved by the anesthetists not involved in the anesthetic management or postoperative outcome assessment. The intraoperative management and data collection were recorded by anesthetists, who were allowed to enter the operating room after a considerable time from induction so as not to know the group assignment.
Standard monitoring devices were attached, and baseline measurements of the heart rate (HR), mean arterial blood pressure (MAP), and oxygen saturation (SpO2) were noted. Atropine 0.01 mg/kg was administered intravenously after an intravenous line was established to induce general anesthesia in both groups using 8% sevoflurane in 100% oxygen.
Inj. atracurium 0.5 mg/kg IV and fentanyl 2 µg/kg were used as a muscle relaxant for endotracheal intubation using a cuffed endotracheal tube of the appropriate size.
Patients were assigned to either Group C (control group) to receive a general anesthetic with no block, or to Group E (block group) to receive a general anesthetic plus ESPB.
The block was performed at the level of T9–10 with the patient lying prone. A high-frequency linear ultrasound probe was positioned 1-2 cm laterally to the midline at the T9 level after skin disinfection with 10% Povidone Iodine. A 22 G needle was placed using an in-plane approach deep within the erector spinae muscle (ESM) after the transverse process and the erector spinae muscle had been identified. The delivery of 0.5–1 mL of normal saline allowed researchers to see the hydro-dissection between the transverse process and the ESM, confirming that the needle placement was accurate.
For unilateral ESPB, deep injections of 0.25% bupivacaine in a calculated volume of 0.5 mL/kg (with a maximum dose of 20 mL) were made into the ESM in accordance with the planned aspect of the operation.
The perioperative anesthetic care was carried out by the anesthetists blinded to the study groups. Sevoflurane 2% in 50% oxygen and air, atracurium 0.1 mg/kg every 15 to 25 minutes, were used to maintain anesthesia. Hemodynamic variables were monitored every 5 minutes; additional boluses of 1 g/kg fentanyl were administered when the HR or MAP rose above 20% of the baseline. All patients received 15 mg/kg of paracetamol for postoperative analgesia at the conclusion of the procedure, and they were all extubated once the residual effects of the muscle relaxants were abolished by atropine 0.02 mg/kg and neostigmine 0.05 mg/kg, and full muscle power and consciousness had been restored.
Hemodynamic variables were monitored every 15 minutes in the post-anesthesia care unit (PACU) up to 1 hour after surgery. As soon as a patient recovered in the PACU, the pain was first evaluated by FLACC (Face, Leg, Activity, Cry, Consolability) pain scale.7 The scale has a range of 0 to 10, with 0 denoting no pain and 10 denoting the most intense agony, and was assessed and recorded at 0 h (in PACU), then at 2, 4, 6, 9, 12, 18, and 24 h after surgery. Inj. paracetamol 15 mg/kg IV was given every 8 hours for standard postoperative analgesia. The time from extubation to the first complaint of pain with FLACC ≥ 4 was documented as the time to first analgesic request, and 1 mg/kg tramadol IV was given. At 6 months after surgery, the presence of painful sensation at the site of surgery was evaluated by a telephone call by an investigator who was blinded to group allocation.
The primary outcome was the total postoperative tramadol dose; secondary outcomes included perioperative HR and MAP values, total quantities of intraoperative fentanyl, first post-operative time moving around, hospital stay, and any adverse effects. Also, postoperative oxygen saturation, respiratory rate, depth of breathing, and the need for oxygen supplementation were observed.
G-power 3.1 software was used to conduct a power analysis. The primary outcome variable in the current study was the total amount of narcotic (tramadol) usage on the first day after surgery. We conducted a pilot study (7 patients) in each group, which revealed a mean of tramadol in Group C as 50.3 ± 26 mg versus 25.4 ± 14 mg in Group E. With a power of study of 90%, two two-tailed t-test, with an alpha value of 0.05, a sample of 40 patients was revealed after adding 20% for possible dropouts.
Statistical analysis
Data were fed to the computer and analysed using IBM SPSS software package version 20.0. (Armonk, NY: IBM Corp). Categorical data were represented as numbers and percentages. Chi-square test was applied to compare different groups. Alternatively, the Monte Carlo correction test was applied when more than 20% of the cells had expected counts less than 5. For continuous data, they were tested for normality by the Shapiro-Wilk test. Quantitative data are expressed as mean and standard deviation or median (range). Student t-test was used to compare two groups for normally distributed quantitative variables. On the other hand, Mann Whitney test was used to compare two groups for not normally distributed quantitative variables. Significance of the obtained results was judged at the 5% level.
3. RESULTS
The eligibility of 96 pediatric patients was assessed; 36 patients didn’t fulfill the inclusion criteria, and 20 patients or their parents refused to participate in this study. The remaining 40 patients were randomly and equally divided into Group E and Group C. All patients were followed up, and their data were analyzed without dropouts.
According to the demographic data, there was no significant difference between the groups related to their age, weight, gender or type or duration of surgery (Table 1).
| Table 1: Comparative demographic data of the two groups | |||
| Variables | ESPB group (n = 20) |
Control group (n = 20) |
P value |
| Age (yr) | 6.40 ± 2.23 | 6.15 ± 2.23 | 0.725 |
| Gender | |||
| Male | 11 (55.0) 9 (45.0) |
10 (50.0) 10 (50.0) |
0.752 |
| Female | |||
| Weight (kg) | 20.2 ± 4.67 | 19.8 ± 4.62 | 0.761 |
| ASA I | 10 (50.0) 10 (50.0) |
11 (55.0) 9 (45.0) |
0.752 |
| II | |||
| Duration of surgery (min) | 72.8 ± 5.50 | 76.3 ± 8.25 | 0.772 |
| Type of surgery | |||
| Splenectomy | 8 (40.0) | 5 (25.0) | 0.726 |
| Nephrectomy | 4 (20.0) | 4 (20.0) | |
| Cyst removal | 3 (15.0) | 3 (15.0) | |
| Cholecystectomy | 5 (25.0) | 6 (30.0) | |
| Pyeloplasty | 0 (0.0) | 2 (10.0) | |
| Data presented as n (%) or mean ± SD; P < 0.05 considered as significant | |||
Regarding perioperative hemodynamics, the vital signs between the groups were compared; Group E showed a significant reduction in heart rate during surgery and up to 1 hour after surgery (P < 0.001) (Figure 1). However, MAP values were significantly decreased in Group E than in Group C at 35, 55, 65, 70, and 75 minutes intraoperative and postoperative time points (P < 0.05) (Figure 2).
Figure 1: Comparative mean heart rates in the two studied groups
Figure 2: Comparative MAP in the two studied groups
Postoperative FLACC pain scores were significantly decreased in Group E, as compared to Group C at all assessment points except at 12 h and 18 h after surgery, as shown in Table 2.
| Table 2: postoperative pain scores | |||
| FLACC score | ESPB group (n = 20) |
Control group (n = 20) |
P value |
| 0 hr | 0.85 ± 1.14 | 4.05 ± 2.06 | < 0.001* |
| 2 | 0.95 ± 1.10 | 6.75 ± 17 | < 0.001* |
| 4 | 1 ± 0.65 | 2.60 ± 15 | < 0.001* |
| 6 | 2.30 ± 1.22 | 5.90 ± 0.97 | < 0.001* |
| 9 | 3.80 ± 0.70 | 2.25 ± 0.91 | < 0.001* |
| 12 | 5.80 ± 0.89 | 5.90 ± 12 | 0.820 |
| 18 | 3.30 ± 0.73 | 3.65 ± 1.46 | 0.461 |
| 24 | 1.65 ± 0.67 | 3.10 ± 1.25 | < 0.001* |
| *P < 0.05 considered significant | |||
Intraoperative fentanyl consumption was significantly reduced in Group E 2.80 ± 6.85 µg compared to the Group C 20 ± 4.87 µg, (P < 0.001). Total postoperative tramadol consumption (primary outcome) was significantly reduced in Group E compared to Group C (P < 0.001). Time to first request of postoperative analgesia was significantly reduced in Group E compared to Group C (P < 0.001), as can be seen in Table 3.
The impact of improved analgesic quality in Group E was reflected by the significantly earlier time to ambulate (P < 0.001), shorter hospital stays (P < 0.001), and lower incidence of chronic pain at 6 months after surgery (P = 0.02) as shown in Table 3.
Also, the respiratory muscle activity was significantly better in Group E as evidenced by the higher postoperative oxygen saturation values on room air in PACU, a lower number of patients requiring oxygen supplementation, lower respiratory rate values, with more patients achieving an adequate depth of breathing (P < 0.001) (Table 3).
| Table 3: analgesic and respiratory quality | |||
| Parameter | ESPB group (n = 20) |
Control group (n = 20) |
P value |
| Total tramadol consumption (mg) | 21.3 ± 11.7 | 71.7 ± 19.7 | <0.001* |
| intraoperative fentanyl consumption (mic) | 2.80 ± 6.85 | 20 ± 4.87 | <0.001* |
| First time request of postoperative analgesia (hr) | 11.7 ± 0.95 | 1.30 ± 0.98 | <0.001* |
| Onset of patient mobilization (hr) | 3 ± 13 | 6.60 ± 1.31 | <0.001* |
| Postoperative hospital stays (hr) | 27 ± 5.33 | 57.60 ± 126 | <0.001* |
| Postoperative oxygen saturation on room air in PACU | 96.0 ± 2.13 | 89.9 ± 2.56 | <0.001* |
| Depth of breathing Deep Shallow |
17 (85) 3 (15) |
7 (35) 13 (65) |
<0.001* |
| Respiratory rate (breaths/min) | 19.5 ± 3.41 | 28.2 ± 3.38 | <0.001* |
| Need for oxygen supplement | 3 (15) | 14 (70) | <0.001* |
| Chronic pain at 6 months | 9 (45) | 4 (20) | 0.02* |
| Data presented as n (%) or mean ± SD; P < 0.05 considered as significant | |||
4. DISCUSSION
Most of the patients undergoing major upper abdominal surgery run the risk of postoperative breathing problems due to atelectasis brought upon by pain. Open cholecystectomy, splenectomy, or procedures involving the kidneys, such as pyeloplasty, cyst excision, or partial or complete nephrectomy, are among the upper abdominal operations commonly undertaken in children. These surgeries are typically accompanied by considerable postoperative pain. Achieving adequate analgesia, maintaining respiratory muscle strength, and early patient mobilization are critical elements of perioperative care.
Anesthesia and the surgical procedure both cause physiological changes. Due to the effects of the anesthetic drugs, surgery, as well as the impact of pain, causing lung or chest wall restriction, respiratory muscle dysfunction, etc., these physiologic alterations continue in the post-operative period.
The most widely prescribed medications for the management of moderate to severe postoperative pain are opioid analgesics. Respiratory depression is frequently caused by opioid overdose, particularly when combined with longer-acting medications like morphine.
In our study, we substituted an ESPB for conventional analgesic methods. Our research demonstrated that ESPB was a successful pain management technique for children undergoing open upper abdominal surgery. It could be used in place of conventional analgesics with the satisfaction of the patients.
In the control group, the patients with FLACC scores of 4–7 necessitated postoperative supplementation with more analgesics. ESPB demonstrated satisfactory results of pain relief detected by low grading of FLACC scores (average 2-4) that did not require additional analgesic support.
The patients in the ESPB group had free respiratory muscle activity as evidenced by higher SpO2 levels and deeper respirations; whereas patients in the control group had lower oxygen saturations and required oxygen supplementation with shallower breathing that was primarily brought on by pain and basal lung atelectasis.
This was consistent with an earlier study performed by Forero et al. (2016), indicating that the ESPB may be a valuable therapeutic option in the management of post-thoracotomy pain syndrome (PTPS). Its immediate analgesic efficacy provides patients with temporary symptomatic relief while other aspects of chronic pain management are optimized, and it may also often confer prolonged analgesia.6
The results were also comparable with a meta-analysis for various surgeries performed by Yu Cui, et al. (2022), reporting that ESPB reduced the accumulated opioid consumption during the first 24 h after surgery. Besides, ESPB could prolong the time to first rescue analgesia after surgery.8
Kompal Jain, et al. (2018) conducted a study on a case series, proving the effectiveness of ESPB in pain reduction for conditions ranging from acute postoperative pain following breast, thoracotomy, and abdominal operations to chronic neuropathic pain.9
Viderman et al. (2022) performed a meta-analysis study that demonstrated that there were no reports of serious complications associated with ESPB for postoperative analgesia in adult abdominal surgery.10 Other studies confirmed the same results.11-14
Contrary to our findings, Heejoon et al. (2022) found that ESPB did not reduce overall fentanyl consumption in the first 24 hours following open gastrectomy and only lessened postoperative discomfort until three hours after surgery.15
5. LIMITATIONS
There are some limitations to our study: First, the small sample size limits the generalizability of our findings. Second, we assessed oxygen saturation with color of the rate, and depth of respiratory excursion to assess the respiratory activity in our patients. Ultrasound-guided parameters like lung ultrasound score may be more reliable in assessing lung collapse after surgery. Although chronic pain incidence at 6 month was significantly lower in ESPB group, the small sample couldn’t power these findings. Finally, assessment of co-factors that determine pain chronicity like functional disability and anxiety scores could increase the global value of ESPB beyond its acute postoperative analgesic benefit.
6. CONCLUSION
ESPB decreased intraoperative nociception, improved the postoperative analgesia, and decreased opioid consumption after surgery, which resulted in better respiratory activity with fewer requirements for oxygen supplements.
7. Data availability
The data generated in this study are available upon request from the corresponding author.
8. Funding
No external funding or industry sponsorship was used in this study. The researchers used the university resources to complete the study.
9. Conflicts of interest
The authors declare that they had no conflicts of interest.
10. Authors' contributions
NES: Study concept and design, data collection and interpretation, drafting the manuscript and revising it, approved the final draft.
AKSS: Data collection and analysis, drafting the manuscript and revising it, approved the final draft.
AAMG: Data collection, interpretation, and analysis, drafted and revised the manuscript, approved the final draft.
VFJ: Study concept and design, data collection and interpretation, drafting the manuscript and revising it.
11. REFERENCES
- Sato M, Iida T, Kikuchi C, Sasakawa T, Kunisawa T, Bosenberg A. Comparison of caudal ropivacaine-morphine and paravertebral catheter for major upper abdominal surgery in infants. Paediatr Anaesth. 2017;27(5):524-30. [PubMed] DOI: 1111/pan.13104
- Celli BR, Rodriguez K, Snider GL. A controlled trial of intermittent positive pressure breathing, incentive spirometry and deep breathing exercise in preventing pulmonary complications after abdominal surgery. Am Rev Respir Dis. 1984;130(1):12-5. [PubMed] DOI: 1164/arrd.1984.130.1.12
- Karcz M, Papadakos PJ. Respiratory complications in the post-anaesthesia care unit: A review of pathophysiological mechanisms. Can J Respir Ther. 2013;49(4):21-9. [PubMed]
- Pawar D. Common post-operative complications in children. Indian J Anaesth. 2012;56(5):496-501. [PubMed] DOI: 4103/0019-5049.103970
- Benyamin R, Trescot AM, Datta S, Buenaventura R, Adlaka R, Sehgal N, et al. Opioid complications and side effects. Pain Physician. 2008;11(2):105-20. [PubMed]
- Forero M, Adhikary SD, Lopez H, Tsui C, Chin KJ. The Erector Spinae Plane Block: A Novel Analgesic Technique in Thoracic Neuropathic Pain. Reg Anesth Pain Med. 2016;41(5):621-7. [PubMed] DOI: 1097/AAP.0000000000000451
- Merkel SI, Voepel-Lewis T, Shayevitz JR, Malviya S. The FLACC: a behavioral scale for scoring postoperative pain in young children. Pediatr Nurs. 1997;23(3):293-7. [PubMed]
- Cui Y, Wang Y, Yang J, Ran L, Zhang Q, Huang Q, et al. The Effect of Single-Shot Erector Spinae Plane Block (ESPB) on Opioid Consumption for Various Surgeries: A Meta-Analysis of Randomized Controlled Trials. J Pain Res. 2022;15:683-99. [PubMed] DOI: 2147/JPR.S346809
- Jaiswal V, Puri A. Erector spinae plane block: Relatively new block on horizon with a wide spectrum of application – A case series. Indian J Anaesth. 2018;62(10):809-13. [PubMed] DOI: 4103/ija.IJA_263_18
- Viderman D, Aubakirova M, Abdildin YG. Erector Spinae Plane Block in Abdominal Surgery: A Meta-Analysis. Front Med. 2022;9:812531. [PubMed] DOI: 3389/fmed.2022.812531
- Abu Elyazed MM, Mostafa SF, Abdelghany MS, Eid GM. Ultrasound-Guided Erector Spinae Plane Block in Patients Undergoing Open Epigastric Hernia Repair: A Prospective Randomized Controlled Study. Anesth Analg. 2019;129(1):235-40. [PubMed] DOI: 1213/ANE.0000000000004071
- Kang RA, Lee S, Kim GS, Jeong JS, Gwak MS, Kim JM, et al. Comparison of Analgesic Efficacy of Erector Spinae Plane Block and Posterior Quadratus Lumborum Block in Laparoscopic Liver Resection: A Randomized Controlled Trial. J Pain Res. 2021;14:3791-800. [PubMed] DOI: 2147/JPR.S343366
- Zhang J, He Y, Wang S, Chen Z, Zhang Y, Gao Y, et al. The erector spinae plane block causes only cutaneous sensory loss on ipsilateral posterior thorax: a prospective observational volunteer study. BMC Anesthesiol. 2020;20(1):88. [PubMed] DOI: 1186/s12871-020-01002-0
- Sakae TM, Mattiazzi APF, Fiorentin JZ, Brandão J, Benedetti RH, Takaschima A. Ultrasound-guided erector spinae plane block for open inguinal hernia repair: a randomized controlled trial. Braz J Anesthesiol. 2022;72(1):49-54. [PubMed] DOI: 1016/j.bjane.2021.04.032
- Jeong H, Choi JW, Sim WS, Kim DK, Bang YJ, Park S, et al. Ultrasound-guided erector spinae plane block for pain management after gastrectomy: a randomized, single-blinded controlled trial. Korean J Pain. 2022;35(3):303-10. [PubMed] DOI: 3344/kjp.2022.35.3.303