Hend Saad Rizk Farhat 1 , Hoda Alsaid Ahmed Ezz 2 , Amir Abo Zekri Elsyed 3 , Mohammad Fouad Algyar 4
Authors affiliations:
Background & objective: 40-60% of surgical patients experience severe postoperative pain. This study aims to look at serratus anterior plane block (SAPB) with erector spinae plane block (ESPB) with dexmedetomidine added to bupivacaine for the administration of intense agony after bosom a medical procedure.
Methodology: A randomized controlled trial involving 40 women over 20 years old booked for a medical procedure. Patients were divided into two groups: SAPB (received SAPB) and ESPB (received ESPB at T5). Blocks were performed after general sedation on the worked side with bupivacaine 0. 25% with 0.5 µg/kg dexmedetomidine in 30 mL.
Results: In comparison to the SAPB group, the ESPB group exhibited a delayed time to initial desire for salvage absence of pain (P < 0.001). In the first 24 hours, it consumed a much smaller amount of pethidine than the SAPB group (P = 0.011). At two, six, and twelve hours, the ESPB group numerical rating scale was significantly lower than the SAPB group (P < 0.05). At 45 and 60 min, the ESPB group pulse and mean blood vessel pressure were significantly lower than those of the SAPB group (P < 0.05). Postoperative queasiness and retching, bradycardia, and hypotension were unimportant between the two gatherings.
Conclusion: With dexmedetomidine added to bupivacaine, ESPB gives delayed absence of pain, lower torment scores and postoperative pain-relieving prerequisites, and better hemodynamics with practically no distinction in aftereffects compared to SAPB in in mastectomy patients.
Abbreviations: ESPB: Erector Spinae Plane Block, PONV: postoperative nausea and vomiting, SAPB: serratus anterior plane block.
Keywords: Serratus Anterior Plane; Erector Spinae Plane; Block; Dexmedetomidine; Bupivacaine; Mastectomy
Citation: Farhat HSR, Ezz HAA, Elsyed AAZ, Algyar MF. Ultrasound guided serratus anterior plane block versus erector spinae plane block with bupivacaine plus dexmedetomidine for postoperative pain after mastectomy. Anaesth. pain intensive care 2025;29(5):345-351. DOI: 10.35975/apic.v29i5.2872
Received: November 24, 2024; Revised: January 20, 2025; Accepted: February 05, 2025
Approximately 40 to 60% of breast surgery patients suffer from severe acute postoperative pain, with more than 10% experiencing severe pain for six to twelve months (postmastectomy pain syndrome).1 Unfortunate control of intense postoperative torment is related with expanded bleakness, postponed wound recuperating, delayed emergency clinic stays, expanded results of narcotic use, constant agony, and high medical care costs.2
Intraoperative and postoperative torment is ordinarily dealt with narcotics; nonetheless, it is related with antagonistic impacts, including delayed sedation, respiratory melancholy, and postoperative nausea and vomiting (PONV).3
Local sedatives have a restricted term of activity, so adjuvants, for example, narcotics, alpha 2 agonists, neostigmine, or magnesium ought to be added.4
Dexmedetomidine has pain relieving properties that might relate to excitement of α2 receptors, hindrance of nerve conduction through C and A δ strands, and neighborhood enkephalin discharge.5, 6
Local sedation (LS) is infused under ultrasonic direction hastily in the serratus front muscle, which permits an anticipated and somewhat lengthy territorial sedation, which would be reasonable for surgeries performed on the chest wall.
The serrated anterior plane block (SAPB) has been utilized to give dependable absence of pain in patients going through bosom a medical procedure.7 Plane B is a powerful methodology for bosom a medical procedure absence of pain because of its effortlessness of organization, insignificant gamble of secondary effects, and capacity to give huge help with discomfort.2
The erector spinae plane block (ESPB) is one of the arising territorial procedures for postoperative agony the board. BSE has been effectively utilized in numerous surgeries like mastectomy, thoracotomy, percutaneous nephrolithotomy, lumbar combinations, hernia fix, cesarean area and furthermore in all out hip arthroplasty.8, 9
ESPB can be managed singularly during a changed extremist mastectomy. The sedation is like epidural chest block yet makes no hemodynamic side impacts, and ESPB has been found to lessen narcotic use after bosom a medical procedure.10
This study compared SAPB and ESPB, with dexmedetomidine added to bupivacaine for the management of postoperative pain after mastectomy.
Forty women, aged over 20 years, ASA status I or II, were enrolled in this randomized controlled preliminary study in preparation for a breast operation. The evaluation took place between July 2023 and July 2024 after endorsement by the Morals Advisory Group of Kafr Elsheikh College Emergency clinic, Kafr Elsheikh, Egypt. A composed informed assent was gotten from the cases.
power 3.1.9. 2 was utilized to calculate the test measure (College of Kiel, Germany). Based on the taking after variables, a test measure of 17 patients per group was determined: 90% research power and a 0.05 α error to demonstrate a 25% reduction in rescue analgesia (pethidine) required to 24 hours with ESPB compared with SAPB (average). difference 15.25 mg) during the postoperative period (primary endpoint) with a common standard deviation of 13 according to a previous study) [11]. Three additional cases were incorporated into each group to address the issue of dropping out. Consequently, a total of 20 patients were assigned to each group.
Exclusion criteria were patients who known allergy to local anesthetics, opioid or dexmedetomidine medications, advanced heart block, ventricular dysfunction, skin infection in at the site of injection, pre-existing chronic pain, coagulopathies, significant liver, or renal insufficiency.
Random numbers produced by a computer were utilized to randomly divide the patients into two equal groups. A different researcher, who was not involved in the study, opened the sealed package. The ESPB group was administered ESPB at T5 on the operated side along with 25% plus 0.5 µg/kg of dexmedetomidine in 30 mL, whereas the SAPB group received 0.25% bupivacaine and 0.5 μg/kg dexmedetomidine in 30 mL on the operated side. Because each block utilised a different approach, the research was opened.
All patients went through a total history, clinical assessment, and routine research facility tests. After cannula inclusion, all patients got premedication with intravenous midazolam (IV) 2 mg, and patients got the mediation procedure as indicated by concentrate on group task. In all cases, the standard strategy of general sedation was utilized. Standard checking procedures, counting beat oximetry, temperature appraisal, non-invasive circulatory strain estimation, 5-lead ECG, and capnography, were utilized. Acceptance of common anesthesia was accomplished utilizing intravenous propofol at a dose of 2 mg/kg and fentanyl at 1 µg/kg. Taking after this, endotracheal intubation was conducted with intravenous atracurium at a measurement of 0.5 mg/kg. Maintenance of sedation was accomplished with isoflurane administered in a mixture of 50% oxygen and air. Incremental doses of intravenous atracurium, specifically 0.01 mg/kg, were administered as needed. Patients were subsequently placed on mechanical ventilation to ensure end-tidal CO2 levels remained between 30-35 mmHg, with a respiratory rate set at 12 breaths per min, a tidal volume of 7 mL/kg, an inspiratory to expiratory time proportion of 1:2, and a positive end-expiratory weight of 5 cmH2O. Each quiet was managed bupivacaine at a concentration of 0.01 mg/kg and 0.5 µg/kg of dexmedetomidine, totaling 30 mL, irrespective of the block type used. All nerve blocks were executed using a 22-gauge Quincke echogenic spinal needle, guided by an in-plane technique with an ultrasound machine operating at a frequency of 8-13 MHz.
2.1. Serratus anterior plane block
Patients were set in a prostrate situation with the arm kidnapped. Three muscles were identified by placing the test in the middle of the axilla, at the fourth and fifth ribs: the serratus (profound and mediocre), the teres major (unrivalled), and the latissimus dorsi (shallow and back). A further milestone for identifying the shallow plane of the serrated first muscle is the dorsal thoracic course. In arrange to affirm the right area of the needle tip by envisioning the spread all through the serratus first muscles, 0.5 mL of saline was implanted, and the needle was embedded in a level method.
2.2. Erector spinae plane block
Patients were put within the horizontal decubitus position with the chosen location confronting upwards. The test was found 3 cm on a level plane absent from the T5 spinous prepare, and the transverse preparation was recognized. The needle was gradually embedded until its tip was situated inside the erector spinae muscle. To confirm the exact situating of the needle tip, 0.5 mL of typical saline was infused, encouraging the perception of the scattering beneath the erector spinae muscle.
In case the blood vessel diameter or heart rate (HR) went over 20% of normal values, an additional bolus of 0.5 µg/kg IV fentanyl was given. At the conclusion of the strategy, all sedation was stopped, and residual neuromuscular block was reversed with neostigmine 0.08 mg/kg and atropine 0.02 mg/kg, after which extubation was done, when breathing was adequate. The patients were then moved to the post-anesthesia care unit (PACU).
2.3. After medical procedure
Patients received 1 g paracetamol IV. A bolus of pethidine 0.5 mg/kg was injected if NRS > 3. NRS was estimated at zero hour, at 60 min, 2, 6, 12, 18 and 24 hours after medical procedure. Bradycardia (HR < 60) was treated with 0.01 mg/kg atropine. Hypotension (MBP < 20% of normal) was treated with a 200 mL intravenous liquid bolus. PONV was treated with ondansetron 0.1 mg/kg IV.
The analgesic period was characterized as the time from the time to block to the first use of rescue analgesic. The essential endpoint was the amount of rescue analgesic [pethidine (mg)] used in the initial 24 hours after the medical procedure. Optional endpoints were intraoperative fentanyl utilization, hemodynamic parameters, NRS and restlessness.
2.4. Sample size calculation
power 3.1.9. 2 was utilized to calculate the test measure (College of Kiel, Germany). Based on the taking after variables, a test measure of 17 patients per group was determined: 90% research power and a 0.05 α error to demonstrate a 25% reduction in rescue analgesia (pethidine) required in 24 hours with ESPB compared with SAPB (average). difference 15.25 mg) during the postoperative period (primary endpoint) with a common standard deviation of 13 according to a previous study.11 Three additional cases were incorporated into each group to address the issue of exclusion. Consequently, a total of 20 patients were assigned to each group.
2.5. Statistical analysis
Data analysis was conducted utilizing SPSS version 26 (IBM Inc., Chicago, IL, USA). The Shapiro-Wilk test, together with histograms, was utilized to evaluate the typicality of information dispersion. Quantitative parameters are presented as the mean and standard deviation (SD); and comparison between the two groups done with the unpaired Student's t-test. Nonparametric quantitative data is presented as the median and interquartile ratio (IQR) and surveyed utilizing the Mann-Whitney test. Categorical factors are displayed as n (%), and were analyzed utilizing either the Chi-square test or Fisher's exact test, depending on what was suitable. A two-tailed P-value < 0.05 was considered significant.
A total of 57 patients were evaluated for inclusion, 10 patients didn't meet the criteria, and 7 patients were dropped due to various reasons. The remaining patients were randomly divided into two equivalent groups (20 patients in each). All selected patients were followed up and investigated (Figure 1).
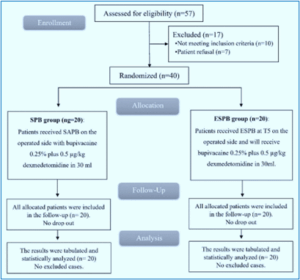
Figure 1: CONSORT study flow diagram
Demographic parameters including age, weight, education level, BMI, ASA status and the duration of the medical procedure were equivalent in the two gatherings (Table 1).
HR and NIBP measurements were not significantly different at various time points; at 15 min, 30 min, 75 min, and at the conclusion of the surgical procedure, showing notably lower values in the ESPB group compared to the SAPB group at 45 min and 60 min (P < 0.05) (Figure 2).
There were no noteworthy differences within the NRS scores in the recovery room or at 1 am, 6 pm, and 24 hours after the operation between the two groups. All things considered, the ESPB was associated with impressively lower NRS scores compared to the SAPB group at 02:00, 6:00, and 12:00 pm (P < 0.05), as presented in Table 2.
Within the ESPB group, the interval to remain pain free was longer than the SAPB group (P < 0.001). Moreover, the amount of pethidine used within the first 24 hours was essentially lower within the ESPB group compared to the SAPB group (P = 0.011), as displayed in Table 3.
Table 4 shows that there were no significant differences in the frequencies of PONV, bradycardia or hypotension between the two groups.
Patients have different levels of discomfort following breast surgery. In addition to raising patient morbidity and mortality during the postoperative phase, poorly managed postoperative pain can also raise the prevalence of chronic pain [12]. In our study, at 45 and 60 min, the ESPB group's HR and MAP were noticeably lower than those of the SAPB group. There was no statistically significant difference between the two groups at baseline, 15 min, 30 min, 75 min, or at the conclusion of the procedure. In line with what we found, Bedewy et al. (2024) discovered that, over a number of periods, ESPB was linked to a lower MAP than SAPB.13 Contrary to our findings, Gamal et al. [14] revealed that there were no appreciable variations in HR or MAP between the SAPB and ESPB groups. This discrepancy might be explained by the fact that, in contrast to Gamal et al., who used 20 mL of bupivacaine, our study used 30 mL of bupivacaine with dexmedetomidine as an adjuvant. At 2, 6, and 12 hours, the NRS in group ESPB was significantly lower than that in group SAPB; however, at PACU, at 1, 18
and 24 hours, there was no statistically significant difference between the two groups. Consistent with our findings, Bedewy et al. (2024) discovered that at most intervals, the group ESPB's pain score was noticeably lower than SAPB's.13 This was consistent with our findings. Sagar et al. (2022) observed that group ESPB's mean NRS score was considerably lower than group SAPB's.15 Contrary to what we found, Gamal et al. (2024) found no discernible variations in pain levels during rest or movement between the ESPB and SAPB groups on the first postoperative day.14 In our study, group ESPB took significantly longer than group SAPB to request rescue analgesia for the first occasion.
Group ESPB consumed a much lower total dosage of pethidine over the first 24 hours than group SAPB. Consistent with our findings, Bedewy et al. (2024) reported that, in comparison to groups SAPB, group ESPB showed a considerable decrease in overall opioid intake.13 This was consistent with our findings, Sagar et al. (2022) shown that Group ESPB's mean analgesia duration was noticeably longer than Group SAPB's. In comparison to Group SAPB, the patients in Group ESPB needed much less rescue analgesia overall throughout the course of the 24-hour postoperative period.15 Gamal et al. reported no statistically significant differences between the SAPB and ESPB groups in terms of the initial request for analgesia and total opioid use, which is in contrast to our findings.14
Bradycardia, hypotension, and PONV did not considerably contrast between the two groups within the current investigate. Contrary to our findings, Bedewy et al. found that around 10% of patients in gather SAPB experienced sickness, heaving, and other unfavorable impacts, such as hypotension, but none of the patients in gather ESPB detailed any postoperative issues.13
Our study's small sample size could be the cause of this discrepancy. In contrast to what we found, Sagar et al. has shown that there were no block-related effects, including hypotension.15 This discrepancy might be explained by variations in the population and the use of a control group. Since dexmedetomidine enhances the quality and duration of analgesia and lowers pain scores with fewer problems, resulting in early post-operative discharge, we utilized it as an adjuvant to bupivacaine with both ESPB and SAPB in patients undergoing mastectomy.16 Both the Dex and ESPB groups had analgesia for significantly longer periods of time than the control group. According to Hassan et al. (2023) the ESPB and Dex groups consumed much less opioids after surgery than the control group.17
One of the limitations of the study was a very small sample size, which could have led to negligible side effect data. Because the study was only carried out in one location, the findings could differ from those obtained elsewhere. We did not use a control group.
With dexmedetomidine added to bupivacaine, ESPB provides prolonged analgesia, lower pain scores and postoperative analgesic requirements, and better hemodynamic parameters, without any difference in the side effects, compared to SAPB in patients undergoing mastectomy.
7. Data availability
The numerical data generated during this research is available with the authors.
8. Conflict of interest
All authors declare that there was no conflict of interest.
9. Funding
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Ethical considerations
The Morals Advisory Group of Kafr Elsheikh College Emergency Clinic, Kafr Elsheikh, Egypt, gave its approval to this study.
11. Authors’ contribution
HSRF: Developed the original idea and the protocol, abstracted and analyzed data, wrote the manuscript, and is a guarantor.
AAE: Contributed to the development of the protocol, abstracted data.
HAE, and MFA: Prepared the manuscript.
Authors affiliations:
- Hend Saad Rizk Farhat, Department of Anesthesia, Intensive Care & Pain Management, Faculty of Medicine, Kafr Elsheikh University, Kafr Elsheikh, Egypt; Email: hendfarhat25@gmail.com
- Hoda Alsaid Ahmed Ezz, Department of Anesthesia, Intensive Care & Pain Management, Faculty of Medicine, Tanta University, Tanta, Egypt; Email: hodaezz714@yahoo.com
- Amir Abo Zekri Elsyed, Department of Anesthesia, Intensive Care & Pain Management, Faculty of Medicine, Kafr Elsheikh University, Kafr Elsheikh, Egypt; Email: aabouzkry@gmail.com
- Mohammad Fouad Algyar, Department of Anesthesia, Intensive Care & Pain Management, Faculty of Medicine, Kafr Elsheikh University, Kafr Elsheikh, Egypt; Email: dr.mohamedfouad78@gmail.com
ABSTRACT
Background & objective: 40-60% of surgical patients experience severe postoperative pain. This study aims to look at serratus anterior plane block (SAPB) with erector spinae plane block (ESPB) with dexmedetomidine added to bupivacaine for the administration of intense agony after bosom a medical procedure.
Methodology: A randomized controlled trial involving 40 women over 20 years old booked for a medical procedure. Patients were divided into two groups: SAPB (received SAPB) and ESPB (received ESPB at T5). Blocks were performed after general sedation on the worked side with bupivacaine 0. 25% with 0.5 µg/kg dexmedetomidine in 30 mL.
Results: In comparison to the SAPB group, the ESPB group exhibited a delayed time to initial desire for salvage absence of pain (P < 0.001). In the first 24 hours, it consumed a much smaller amount of pethidine than the SAPB group (P = 0.011). At two, six, and twelve hours, the ESPB group numerical rating scale was significantly lower than the SAPB group (P < 0.05). At 45 and 60 min, the ESPB group pulse and mean blood vessel pressure were significantly lower than those of the SAPB group (P < 0.05). Postoperative queasiness and retching, bradycardia, and hypotension were unimportant between the two gatherings.
Conclusion: With dexmedetomidine added to bupivacaine, ESPB gives delayed absence of pain, lower torment scores and postoperative pain-relieving prerequisites, and better hemodynamics with practically no distinction in aftereffects compared to SAPB in in mastectomy patients.
Abbreviations: ESPB: Erector Spinae Plane Block, PONV: postoperative nausea and vomiting, SAPB: serratus anterior plane block.
Keywords: Serratus Anterior Plane; Erector Spinae Plane; Block; Dexmedetomidine; Bupivacaine; Mastectomy
Citation: Farhat HSR, Ezz HAA, Elsyed AAZ, Algyar MF. Ultrasound guided serratus anterior plane block versus erector spinae plane block with bupivacaine plus dexmedetomidine for postoperative pain after mastectomy. Anaesth. pain intensive care 2025;29(5):345-351. DOI: 10.35975/apic.v29i5.2872
Received: November 24, 2024; Revised: January 20, 2025; Accepted: February 05, 2025
1. INTRODUCTION
Approximately 40 to 60% of breast surgery patients suffer from severe acute postoperative pain, with more than 10% experiencing severe pain for six to twelve months (postmastectomy pain syndrome).1 Unfortunate control of intense postoperative torment is related with expanded bleakness, postponed wound recuperating, delayed emergency clinic stays, expanded results of narcotic use, constant agony, and high medical care costs.2
Intraoperative and postoperative torment is ordinarily dealt with narcotics; nonetheless, it is related with antagonistic impacts, including delayed sedation, respiratory melancholy, and postoperative nausea and vomiting (PONV).3
Local sedatives have a restricted term of activity, so adjuvants, for example, narcotics, alpha 2 agonists, neostigmine, or magnesium ought to be added.4
Dexmedetomidine has pain relieving properties that might relate to excitement of α2 receptors, hindrance of nerve conduction through C and A δ strands, and neighborhood enkephalin discharge.5, 6
Local sedation (LS) is infused under ultrasonic direction hastily in the serratus front muscle, which permits an anticipated and somewhat lengthy territorial sedation, which would be reasonable for surgeries performed on the chest wall.
The serrated anterior plane block (SAPB) has been utilized to give dependable absence of pain in patients going through bosom a medical procedure.7 Plane B is a powerful methodology for bosom a medical procedure absence of pain because of its effortlessness of organization, insignificant gamble of secondary effects, and capacity to give huge help with discomfort.2
The erector spinae plane block (ESPB) is one of the arising territorial procedures for postoperative agony the board. BSE has been effectively utilized in numerous surgeries like mastectomy, thoracotomy, percutaneous nephrolithotomy, lumbar combinations, hernia fix, cesarean area and furthermore in all out hip arthroplasty.8, 9
ESPB can be managed singularly during a changed extremist mastectomy. The sedation is like epidural chest block yet makes no hemodynamic side impacts, and ESPB has been found to lessen narcotic use after bosom a medical procedure.10
This study compared SAPB and ESPB, with dexmedetomidine added to bupivacaine for the management of postoperative pain after mastectomy.
2. METHODOLOGY
Forty women, aged over 20 years, ASA status I or II, were enrolled in this randomized controlled preliminary study in preparation for a breast operation. The evaluation took place between July 2023 and July 2024 after endorsement by the Morals Advisory Group of Kafr Elsheikh College Emergency clinic, Kafr Elsheikh, Egypt. A composed informed assent was gotten from the cases.
power 3.1.9. 2 was utilized to calculate the test measure (College of Kiel, Germany). Based on the taking after variables, a test measure of 17 patients per group was determined: 90% research power and a 0.05 α error to demonstrate a 25% reduction in rescue analgesia (pethidine) required to 24 hours with ESPB compared with SAPB (average). difference 15.25 mg) during the postoperative period (primary endpoint) with a common standard deviation of 13 according to a previous study) [11]. Three additional cases were incorporated into each group to address the issue of dropping out. Consequently, a total of 20 patients were assigned to each group.
Exclusion criteria were patients who known allergy to local anesthetics, opioid or dexmedetomidine medications, advanced heart block, ventricular dysfunction, skin infection in at the site of injection, pre-existing chronic pain, coagulopathies, significant liver, or renal insufficiency.
Random numbers produced by a computer were utilized to randomly divide the patients into two equal groups. A different researcher, who was not involved in the study, opened the sealed package. The ESPB group was administered ESPB at T5 on the operated side along with 25% plus 0.5 µg/kg of dexmedetomidine in 30 mL, whereas the SAPB group received 0.25% bupivacaine and 0.5 μg/kg dexmedetomidine in 30 mL on the operated side. Because each block utilised a different approach, the research was opened.
All patients went through a total history, clinical assessment, and routine research facility tests. After cannula inclusion, all patients got premedication with intravenous midazolam (IV) 2 mg, and patients got the mediation procedure as indicated by concentrate on group task. In all cases, the standard strategy of general sedation was utilized. Standard checking procedures, counting beat oximetry, temperature appraisal, non-invasive circulatory strain estimation, 5-lead ECG, and capnography, were utilized. Acceptance of common anesthesia was accomplished utilizing intravenous propofol at a dose of 2 mg/kg and fentanyl at 1 µg/kg. Taking after this, endotracheal intubation was conducted with intravenous atracurium at a measurement of 0.5 mg/kg. Maintenance of sedation was accomplished with isoflurane administered in a mixture of 50% oxygen and air. Incremental doses of intravenous atracurium, specifically 0.01 mg/kg, were administered as needed. Patients were subsequently placed on mechanical ventilation to ensure end-tidal CO2 levels remained between 30-35 mmHg, with a respiratory rate set at 12 breaths per min, a tidal volume of 7 mL/kg, an inspiratory to expiratory time proportion of 1:2, and a positive end-expiratory weight of 5 cmH2O. Each quiet was managed bupivacaine at a concentration of 0.01 mg/kg and 0.5 µg/kg of dexmedetomidine, totaling 30 mL, irrespective of the block type used. All nerve blocks were executed using a 22-gauge Quincke echogenic spinal needle, guided by an in-plane technique with an ultrasound machine operating at a frequency of 8-13 MHz.
2.1. Serratus anterior plane block
Patients were set in a prostrate situation with the arm kidnapped. Three muscles were identified by placing the test in the middle of the axilla, at the fourth and fifth ribs: the serratus (profound and mediocre), the teres major (unrivalled), and the latissimus dorsi (shallow and back). A further milestone for identifying the shallow plane of the serrated first muscle is the dorsal thoracic course. In arrange to affirm the right area of the needle tip by envisioning the spread all through the serratus first muscles, 0.5 mL of saline was implanted, and the needle was embedded in a level method.
2.2. Erector spinae plane block
Patients were put within the horizontal decubitus position with the chosen location confronting upwards. The test was found 3 cm on a level plane absent from the T5 spinous prepare, and the transverse preparation was recognized. The needle was gradually embedded until its tip was situated inside the erector spinae muscle. To confirm the exact situating of the needle tip, 0.5 mL of typical saline was infused, encouraging the perception of the scattering beneath the erector spinae muscle.
In case the blood vessel diameter or heart rate (HR) went over 20% of normal values, an additional bolus of 0.5 µg/kg IV fentanyl was given. At the conclusion of the strategy, all sedation was stopped, and residual neuromuscular block was reversed with neostigmine 0.08 mg/kg and atropine 0.02 mg/kg, after which extubation was done, when breathing was adequate. The patients were then moved to the post-anesthesia care unit (PACU).
2.3. After medical procedure
Patients received 1 g paracetamol IV. A bolus of pethidine 0.5 mg/kg was injected if NRS > 3. NRS was estimated at zero hour, at 60 min, 2, 6, 12, 18 and 24 hours after medical procedure. Bradycardia (HR < 60) was treated with 0.01 mg/kg atropine. Hypotension (MBP < 20% of normal) was treated with a 200 mL intravenous liquid bolus. PONV was treated with ondansetron 0.1 mg/kg IV.
The analgesic period was characterized as the time from the time to block to the first use of rescue analgesic. The essential endpoint was the amount of rescue analgesic [pethidine (mg)] used in the initial 24 hours after the medical procedure. Optional endpoints were intraoperative fentanyl utilization, hemodynamic parameters, NRS and restlessness.
2.4. Sample size calculation
power 3.1.9. 2 was utilized to calculate the test measure (College of Kiel, Germany). Based on the taking after variables, a test measure of 17 patients per group was determined: 90% research power and a 0.05 α error to demonstrate a 25% reduction in rescue analgesia (pethidine) required in 24 hours with ESPB compared with SAPB (average). difference 15.25 mg) during the postoperative period (primary endpoint) with a common standard deviation of 13 according to a previous study.11 Three additional cases were incorporated into each group to address the issue of exclusion. Consequently, a total of 20 patients were assigned to each group.
2.5. Statistical analysis
Data analysis was conducted utilizing SPSS version 26 (IBM Inc., Chicago, IL, USA). The Shapiro-Wilk test, together with histograms, was utilized to evaluate the typicality of information dispersion. Quantitative parameters are presented as the mean and standard deviation (SD); and comparison between the two groups done with the unpaired Student's t-test. Nonparametric quantitative data is presented as the median and interquartile ratio (IQR) and surveyed utilizing the Mann-Whitney test. Categorical factors are displayed as n (%), and were analyzed utilizing either the Chi-square test or Fisher's exact test, depending on what was suitable. A two-tailed P-value < 0.05 was considered significant.
3. RESULTS
A total of 57 patients were evaluated for inclusion, 10 patients didn't meet the criteria, and 7 patients were dropped due to various reasons. The remaining patients were randomly divided into two equivalent groups (20 patients in each). All selected patients were followed up and investigated (Figure 1).
Figure 1: CONSORT study flow diagram
Demographic parameters including age, weight, education level, BMI, ASA status and the duration of the medical procedure were equivalent in the two gatherings (Table 1).
| Table 1: Demographic data and duration of surgery of the studied groups. | ||||
| Variables | Group SAPB
(n = 20) |
Group ESPB
(n = 20) |
P | |
| Age (years) | 48.95 ± 17.17 | 45.3 ± 12.93 | 0.452 | |
| Weight (kg) | 77.65 ±10.39 | 78.75 ± 11.6 | 0.754 | |
| Height (cm) | 167.85 ± 6.53 | 166.05 ± 4.67 | 0.323 | |
| BMI (kg/m2) | 27.66 ± 4.09 | 28.58 ± 4.05 | 0.477 | |
| ASA physical status | I | 13 (65%) | 14 (70%) | 0.736 |
| II | 7 (35%) | 6 (30%) | ||
| Duration of surgery (min) | 109.75 ± 18.6 | 107.25 ± 25.16 | 0.723 | |
| Data are presented as mean± SD or frequency (%). SAPB: Serratus plane block, ESPB: Erector spinae plane block, ASA: American Society of Anesthesiologists. BMI: Body mass index. | ||||
HR and NIBP measurements were not significantly different at various time points; at 15 min, 30 min, 75 min, and at the conclusion of the surgical procedure, showing notably lower values in the ESPB group compared to the SAPB group at 45 min and 60 min (P < 0.05) (Figure 2).
There were no noteworthy differences within the NRS scores in the recovery room or at 1 am, 6 pm, and 24 hours after the operation between the two groups. All things considered, the ESPB was associated with impressively lower NRS scores compared to the SAPB group at 02:00, 6:00, and 12:00 pm (P < 0.05), as presented in Table 2.
| Table 2: Comparative NRS of the studied groups | |||
| Time | Group SAPB
(n = 20) |
Group ESPB
(n = 20) |
P |
| PACU | 0(0 - 0) | 0(0 - 0) | 1 |
| 1 h | 2(1.75 - 2) | 1(0 - 1) | 0.747 |
| 2 h | 4(2 - 5.25) | 1(1 - 2) | 0.017* |
| 6 h | 4(4 - 5) | 2(2 - 4) | 0.015* |
| 12 h | 4(3 - 5) | 3.5(2 - 4) | 0.005* |
| 18 h | 4(3.75 - 4.25) | 4(3 - 4.25) | 0.582 |
| 24 h | 0(0 - 0) | 4(3 - 4) | 0.371 |
| Data presented as median (IQR). *: Significant as P ≤ 0.05. SAPB: Serratus plane block,
ESPB: Erector spinae plane block, PACU: post anesthesia care unit, NRS: Numerical rating scale. |
|||
Within the ESPB group, the interval to remain pain free was longer than the SAPB group (P < 0.001). Moreover, the amount of pethidine used within the first 24 hours was essentially lower within the ESPB group compared to the SAPB group (P = 0.011), as displayed in Table 3.
| Table 3: Comparative data of rescue analgesia in the first 24 hours | |||
| Variable | Group SAPB
(n = 20) |
Group ESPB
(n = 20) |
P |
| Time to first request of rescue analgesia (h) | 5.75 ± 1.25 | 7.4 ± 1.23 | < 0.001* |
| Total dose of pethidine consumption in
the first 24 hours (mg) |
126.15 ± 19.94 | 106.85 ± 25.59 | 0.011* |
| Data presented as mean ± SD. *: Significant as P ≤ 0.05; SAPB: Serratus plane block,
ESPB: Erector spinae plane block. |
|||
Table 4 shows that there were no significant differences in the frequencies of PONV, bradycardia or hypotension between the two groups.
| Table 4: Complication of surgery of the studied groups. | |||
| Complication | Group SAPB
(n = 20) |
Group ESPB
(n = 20) |
P-value |
| PONV | 4 (20) | 3 (15) | 1 |
| Bradycardia | 4 (20) | 5 (25) | 1 |
| Hypotension | 5 (25) | 7 (35) | 0.731 |
| Data presented as frequency (%). SAPB: Serratus plane block, ESPB: Erector spinae
plane block; PONV: Postoperative nausea and vomiting. |
|||
4. DISCUSSION
Patients have different levels of discomfort following breast surgery. In addition to raising patient morbidity and mortality during the postoperative phase, poorly managed postoperative pain can also raise the prevalence of chronic pain [12]. In our study, at 45 and 60 min, the ESPB group's HR and MAP were noticeably lower than those of the SAPB group. There was no statistically significant difference between the two groups at baseline, 15 min, 30 min, 75 min, or at the conclusion of the procedure. In line with what we found, Bedewy et al. (2024) discovered that, over a number of periods, ESPB was linked to a lower MAP than SAPB.13 Contrary to our findings, Gamal et al. [14] revealed that there were no appreciable variations in HR or MAP between the SAPB and ESPB groups. This discrepancy might be explained by the fact that, in contrast to Gamal et al., who used 20 mL of bupivacaine, our study used 30 mL of bupivacaine with dexmedetomidine as an adjuvant. At 2, 6, and 12 hours, the NRS in group ESPB was significantly lower than that in group SAPB; however, at PACU, at 1, 18
and 24 hours, there was no statistically significant difference between the two groups. Consistent with our findings, Bedewy et al. (2024) discovered that at most intervals, the group ESPB's pain score was noticeably lower than SAPB's.13 This was consistent with our findings. Sagar et al. (2022) observed that group ESPB's mean NRS score was considerably lower than group SAPB's.15 Contrary to what we found, Gamal et al. (2024) found no discernible variations in pain levels during rest or movement between the ESPB and SAPB groups on the first postoperative day.14 In our study, group ESPB took significantly longer than group SAPB to request rescue analgesia for the first occasion.
Group ESPB consumed a much lower total dosage of pethidine over the first 24 hours than group SAPB. Consistent with our findings, Bedewy et al. (2024) reported that, in comparison to groups SAPB, group ESPB showed a considerable decrease in overall opioid intake.13 This was consistent with our findings, Sagar et al. (2022) shown that Group ESPB's mean analgesia duration was noticeably longer than Group SAPB's. In comparison to Group SAPB, the patients in Group ESPB needed much less rescue analgesia overall throughout the course of the 24-hour postoperative period.15 Gamal et al. reported no statistically significant differences between the SAPB and ESPB groups in terms of the initial request for analgesia and total opioid use, which is in contrast to our findings.14
Bradycardia, hypotension, and PONV did not considerably contrast between the two groups within the current investigate. Contrary to our findings, Bedewy et al. found that around 10% of patients in gather SAPB experienced sickness, heaving, and other unfavorable impacts, such as hypotension, but none of the patients in gather ESPB detailed any postoperative issues.13
Our study's small sample size could be the cause of this discrepancy. In contrast to what we found, Sagar et al. has shown that there were no block-related effects, including hypotension.15 This discrepancy might be explained by variations in the population and the use of a control group. Since dexmedetomidine enhances the quality and duration of analgesia and lowers pain scores with fewer problems, resulting in early post-operative discharge, we utilized it as an adjuvant to bupivacaine with both ESPB and SAPB in patients undergoing mastectomy.16 Both the Dex and ESPB groups had analgesia for significantly longer periods of time than the control group. According to Hassan et al. (2023) the ESPB and Dex groups consumed much less opioids after surgery than the control group.17
5. LIMITATIONS
One of the limitations of the study was a very small sample size, which could have led to negligible side effect data. Because the study was only carried out in one location, the findings could differ from those obtained elsewhere. We did not use a control group.
6. CONCLUSION
With dexmedetomidine added to bupivacaine, ESPB provides prolonged analgesia, lower pain scores and postoperative analgesic requirements, and better hemodynamic parameters, without any difference in the side effects, compared to SAPB in patients undergoing mastectomy.
7. Data availability
The numerical data generated during this research is available with the authors.
8. Conflict of interest
All authors declare that there was no conflict of interest.
9. Funding
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Ethical considerations
The Morals Advisory Group of Kafr Elsheikh College Emergency Clinic, Kafr Elsheikh, Egypt, gave its approval to this study.
11. Authors’ contribution
HSRF: Developed the original idea and the protocol, abstracted and analyzed data, wrote the manuscript, and is a guarantor.
AAE: Contributed to the development of the protocol, abstracted data.
HAE, and MFA: Prepared the manuscript.
12. REFERENCES
- De Cassai A, Bonvicini D, Correale C, Sandei L, Tulgar S, Tonetti T. Erector spinae plane block: a systematic qualitative review. Minerva Anestesiol. 2019;85:308–19. [PubMed] DOI: 23736/S0375-9393.18.13341-4
- Yesiltas S, Türköz A, Çalım M, Yılmaz S, Esen A, Daşkaya H, et al. Comparison of serratus plane block alone and in combination with pectoral type 1 block for breast cancer surgery: a randomized controlled study. Hippokratia. 2021;25:8–14. [PubMed]
- Meissner W, Huygen F, Neugebauer EAM, Osterbrink J, Benhamou D, Betteridge N, et al. Management of acute pain in the postoperative setting: the importance of quality indicators. Curr Med Res Opin. 2018;34:187–96. [PubMed] DOI: 1080/03007995.2017.1391081
- Swain A, Nag DS, Sahu S, Samaddar DP. Adjuvants to local anesthetics: current understanding and future trends. World J Clin Cases. 2017;5:307–23. [PubMed] DOI: 12998/wjcc.v5.i8.307
- Tang C, Xia Z. Dexmedetomidine in perioperative acute pain management: a non-opioid adjuvant analgesic. J Pain Res. 2017;10:1899–904. [PubMed] DOI: 2147/JPR.S139387
- Zhao Y, He J, Yu N, Jia C, Wang S. Mechanisms of dexmedetomidine in neuropathic pain. Front Neurosci. 2020;14:330–50. [PubMed] DOI: 3389/fnins.2020.00330
- Blanco R, Parras T, McDonnell JG, Prats‑Galino A. Serratus plane block: a novel ultrasound-guided thoracic wall nerve block. Anaesthesia. 2013;68:1107–13. [PubMed] DOI: 1111/anae.12344
- Hamed MA, Yassin HM, Botros JM, Abdelhady MA. Analgesic efficacy of erector spinae plane block compared with intrathecal morphine after elective cesarean section: a prospective randomized controlled study. J Pain Res. 2020;13:597–604. [PubMed] DOI: 2147/JPR.S242568
- Lennon MJ, Isaac S, Currigan D, O’Leary S, Khan RJK, Fick DP. Erector spinae plane block combined with local infiltration analgesia for total hip arthroplasty: a randomized, placebo‑controlled, clinical trial. J Clin Anesth. 2021;69:110–3. [PubMed] DOI: 1016/j.jclinane.2020.110153
- Wang X, Ran G, Chen X, Xie C, Wang J, Liu X, et al. The effect of ultrasound‑guided erector spinae plane block combined with dexmedetomidine on postoperative analgesia in patients undergoing modified radical mastectomy: a randomized controlled trial. Pain Ther. 2021;10:475–84. [PubMed] DOI: 1007/s40122-020-00234-9
- Gad M, Elmetwally M. Efficacy of adding dexmedetomidine as adjuvant with levobupivacaine in ultrasound‑guided serratus plane block for modified radical mastectomy surgery. Res Opin Anesth Intensive Care. 2019;6:234–42. Full Text
- Nogueira S, Rodrigues D, Barros M, Menezes J, Guimarães‑Pereira L. Chronic pain after breast surgery: incidence, risk factors and impact on quality of life. Rev Esp Anestesiol Reanim. 2024;89:12–6. [PubMed] DOI: 1016/j.redare.2024.01.002
- Bedewy A, Mohamed MS, Sultan HM, Khalil MS. Comparison between erector spinae plane block versus serratus anterior plane block regarding analgesia and stress response after modified radical mastectomy: randomized controlled trial. Anesth Pain Med. 2024;14:15–26. [PubMed] DOI: 5812/aapm-142189
- Wagih GB, Abo‑Ollo MM, Alamrawy WZ, Hozien AI. Serratus anterior plane block (posterior approach) versus erector spinae plane block in modified radical mastectomy; a randomized comparative trial. Egypt J Anaesth. 2024;40:160–70. DOI: 1080/11101849.2024.2331353
- Sagar S, Loha S, Paswan A, Pratap A, Prakash S, Rath A. Comparison of erector spinae plane block and serratus anterior plane block for modified radical mastectomy: a prospective randomized study. J Anesth Res Surg Sci. 2022;30:265–71. Full Text
- Das R, Das RK, Sahoo S, Nanda S. Role of dexmedetomidine as an anaesthetic adjuvant in breast cancer surgery as a day‑care procedure: a randomized controlled study. Indian J Anaesth. 2018;62:182–7. [PubMed] DOI: 4103/ija.IJA_752_17
- Hassan ME, Abdelgalil AS. Efficacy of dexmedetomidine as an adjuvant in erector spinae plane block in breast cancer surgery: a randomized controlled trial. Anaesth Pain Intensive Care. 2023;27:16–22. DOI: 35975/apic.v27i1.2109