Dora Hamad AlHarkan *
Author’s Affiliation:
*Dora Hamad AlHarkan, MD, Department of Ophthalmology, Medical College, Qassim University, Qassim, Saudi Arabia.
Correspondence: Dr. Dora Hamad AlHarkan; Email: dhhrkan@qu.edu.sa; Phone: 00966554882552.
This is a case of persistent pyogenic granuloma (PG) following strabismus surgery in a young female. Although she was prescribed a routine post-operative medication, frequent steroids, and topical antibiotic eye drops and ointments, two weeks after surgery, she developed an inflamed PG at the surgical site. Frequent steroid drops and Tobramycin/dexamethasone eye ointment were prescribed. The lesion did not regress after two months of using topical medications, so surgery was scheduled. However, two weeks after the surgery decision, the patient reported an improvement and regression of the lesion. The lesion disappeared in four weeks. The patient confesses that she did not use the topical ointment before and just started using it when we scheduled her for the second surgery because she was scared of surgery. Fear of surgery seems to improve compliance with medical treatment.
Keywords: Antibiotics; Conjunctival Tumor, Infection; Pyogenic Granuloma; Strabismus Surgery
Citation: AlHarkan DH. Fear of surgery causes complete resolution of a post-strabismus surgery persistent pyogenic granuloma: a case report. Anaesth. pain intensive care 2025;29(5):433-436. DOI: 10.35975/apic.v29i5.2863
Received: April 12, 2025; Revised: May 12, 2025; Accepted: May 13, 2025
Ocular pyogenic granuloma (PG), a lobular capillary hemangioma, is a benign lesion that occurs secondary to ocular trauma or irritation to the conjunctiva, and it is common mainly in younger people and children.1 The trauma-induced genetic mutation results in vascular proliferation as endothelial cell clumps in histopathology.1 Eye diseases and their associated hospitalization and procedures are common globally.2-4 Surgery and handling tissues, suture material, and bleeding could trigger the development of PG. Its incidence is 2.1% after strabismus surgery, and it is highly responding to topical steroids and timolol drops.5
Extended therapy often has poor compliance, especially in teenage patients preoccupied with many other activities. When patients are given the option of remedy through surgery, their compliance with medical treatment, which earlier was not good, could improve.
This is a case of a teenage girl who had persistent PG post-strabismus surgery for esotropia. It did not improve with topical medication, but due to the fear of surgery, she dramatically improved after having good compliance with topical medication.
A 15-year-old girl presented two weeks after strabismus surgery for esotropia with complaints of a mass arising from the wound of surgery in her right eye. The timeline of the appearance of the lesion and history of surgical procedures to treat esotropia is given in Table 1.
She underwent a bilateral medial rectus muscle recession of 6.0 mm using a fornix-based incision. Post-operative medication included prednisolone acetate 1% eye drops to be applied for both eyes in a tapering dose every one week over four weeks (every six hours, every eight hours, every twelve hours, and every twenty-four hours), moxifloxacin eye drops every eight hours for two weeks, and Tobramycin/Dexamethasone eye ointment is to be applied once at night for four weeks for both eyes. One day postoperatively, she was seen, and by orthoptic work-up, she was orthophoria with quiet eyes and mild subconjunctival injection and the wound site with no signs of infection. Two weeks postoperatively, the patient presented to the clinic complaining of a mass lesion pointing from the wound site of the right eye (Figure 1).

Figure 1: Pyogenic granuloma in the right eye two weeks following muscle surgery to treat esotropia
She had no pain, discharge, tenderness, or signs of infection. A slit-lamp examination showed a lobulated mass measured almost 10.00 mm by 10.00 mm. The wound was intact, and no scleral show or pointing sutures. The patient was inquired about the use of post-operative medication, and she responded that she had good compliance. She was diagnosed with a PG. The dose of prednisolone acetate eye drops was increased to every two hours while awake for two days, then every four hours while awake, to be tapered four times, three times, two times, and once, one week for each to the right eye. She was also educated about the use of tobramycin/dexamethasone eye ointment at night. Two months later, the lesion was mildly increased in size with the same redness. So, she was booked for surgical excision. After fixing the date of surgery, two weeks later, she reported that the redness improved, and the lesion started to shrink. One month later, the lesion had almost disappeared with a small residual (Figure 2).
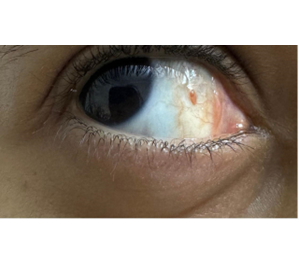
Figure 2: The mass on the bulbar conjunctiva of the right eye was resolved within four weeks of medical treatment
The patient confirmed that she had never used the medications, and she just started using it after booking for surgery. Although her family was educated (the mother is a teacher, her brother is an optometrist, and her sister is a family physician), they were not aware of her poor compliance with medication. PG did not recur two months after the stoppage of medication.
This case report highlights that poor compliance with post-operative medications could be the most common cause of PG, which was not reported before in the literature and is secondary to irritation caused by the sutures at the wound site. In the present case, the teenage child did not reveal the stoppage of the topical application of prescribed medication, and her family was not aware of that. When the surgical approach was decided, two months after no improvement of the lesion, the fear of surgery resulted in judicious usage of the medication and complete resolution of the lesion noticed within four weeks.
Adherence to using topical post-operative medications is challenging. It is known that topical ocular medications usually cause discomfort because of the chemical composition of the medication. This might affect the patient's compliance, especially if there is a wound in the eye post-surgery or if the patient is an uncooperative child or teenager. Other factors can affect compliance, including the number of prescribed medications, frequency of dosing, the age of the patient, the caregiver compliance, patient or caregiver's belief about the medication, blurring of vision from using the ointment, the financial status of the family, trust of the physician, and the degree of understanding of the patient of how to use the medication.6 However, patients with eye conditions with medical and surgical treatment options often continue medical treatment to avoid surgery.
Usually, management of PG focuses on topical medications (topical steroids or topical beta-blockers), but surgical excision is indicated if the lesion is large or persistent. Other modalities of management include cryotherapy and laser ablation, which are sometimes complemented by immunosuppressant mechanisms like antimetabolite applications and steroid usage after excision.7,8
The development of PG after horizontal muscle surgery in the present case is uncommon. A previously published case of infected PG mimicking conjunctival abscess post-strabismus surgery in a young child that presented typically at the same time, two weeks after strabismus surgery.9 That child improved significantly with the proper use of topical steroids, which raises doubts about the compliance of the post-operative usage of the medications. In this case, signs, that indicate poor compliance with the post-operative medications include persistent redness in all follow-up visits and an increase in the size of the lesion, although she was prescribed frequent topical steroids. Although her family was educated and given written instructions on how to use the drops, and her medications were freely given because she was treated in a government hospital, she did not use the medication properly. Adherence to topical medication post-strabismus surgery has not been investigated before. The only available reports are about adherence to post-cataract surgery, to antiglaucoma medication, or to anti-inflammatory medication for uveitis.6,10,11 Poor compliance with post-cataract surgery has been shown to be 30%.6 Adherence to antiglaucoma medications was reported to be 54%.[8] Further studies are needed to investigate patient adherence to medications post-strabismus surgery.
In conclusion, PG can be prevented by properly educating patients about how to use and apply the medication, simplifying the dose regimen, and warning them about the possible complications of PG if medications are not used.
5. Conflict of interest
The author declares that there was no conflict of interest.
6. Ethical issues
Written informed consent was obtained from the patient to publish this report for the academic purposes.
7. Authors’ contribution
DHA was the sole author of this paper.
Author’s Affiliation:
*Dora Hamad AlHarkan, MD, Department of Ophthalmology, Medical College, Qassim University, Qassim, Saudi Arabia.
Correspondence: Dr. Dora Hamad AlHarkan; Email: dhhrkan@qu.edu.sa; Phone: 00966554882552.
ABSTRACT
This is a case of persistent pyogenic granuloma (PG) following strabismus surgery in a young female. Although she was prescribed a routine post-operative medication, frequent steroids, and topical antibiotic eye drops and ointments, two weeks after surgery, she developed an inflamed PG at the surgical site. Frequent steroid drops and Tobramycin/dexamethasone eye ointment were prescribed. The lesion did not regress after two months of using topical medications, so surgery was scheduled. However, two weeks after the surgery decision, the patient reported an improvement and regression of the lesion. The lesion disappeared in four weeks. The patient confesses that she did not use the topical ointment before and just started using it when we scheduled her for the second surgery because she was scared of surgery. Fear of surgery seems to improve compliance with medical treatment.
Keywords: Antibiotics; Conjunctival Tumor, Infection; Pyogenic Granuloma; Strabismus Surgery
Citation: AlHarkan DH. Fear of surgery causes complete resolution of a post-strabismus surgery persistent pyogenic granuloma: a case report. Anaesth. pain intensive care 2025;29(5):433-436. DOI: 10.35975/apic.v29i5.2863
Received: April 12, 2025; Revised: May 12, 2025; Accepted: May 13, 2025
1. INTRODUCTION
Ocular pyogenic granuloma (PG), a lobular capillary hemangioma, is a benign lesion that occurs secondary to ocular trauma or irritation to the conjunctiva, and it is common mainly in younger people and children.1 The trauma-induced genetic mutation results in vascular proliferation as endothelial cell clumps in histopathology.1 Eye diseases and their associated hospitalization and procedures are common globally.2-4 Surgery and handling tissues, suture material, and bleeding could trigger the development of PG. Its incidence is 2.1% after strabismus surgery, and it is highly responding to topical steroids and timolol drops.5
Extended therapy often has poor compliance, especially in teenage patients preoccupied with many other activities. When patients are given the option of remedy through surgery, their compliance with medical treatment, which earlier was not good, could improve.
This is a case of a teenage girl who had persistent PG post-strabismus surgery for esotropia. It did not improve with topical medication, but due to the fear of surgery, she dramatically improved after having good compliance with topical medication.
2. CASE REPORT
A 15-year-old girl presented two weeks after strabismus surgery for esotropia with complaints of a mass arising from the wound of surgery in her right eye. The timeline of the appearance of the lesion and history of surgical procedures to treat esotropia is given in Table 1.
| Table 1: Timeline of events in the life of a teenage patient with PG secondary to muscle surgery to treat large angle esotropia and its spontaneous resolution with medical treatment. | ||
| S. No | Event | Time |
| 1 | Date of birth | 2009 |
| 2 | Large angle esotropia | Since early childhood |
| 3 | Orthoptic evaluation of esotropia at pediatric ophthalmology unit (Left esotropia 60 PD) | September 2021 |
| 4 | Botulinum toxin (BOTOX Allergan®) injection (7.5 International Units (IU)/ 0.1 ml) for both medial rectus muscles | October 2021 |
| 5 | Left eye esotropia 45 PD for near fixation and 40 PD for far point fixation | January 2022 |
| 6 | BOTOX injection (7.5 (IU)/ 0.1 ml) was injected for both medial rectus muscles | March 2023 |
| 7 | Bilateral medial rectus muscle recession of 6.0 mm | October 2024 |
| 8 | Topical Prednisolone acetate 1% eye drops tapering dose over four weeks, Moxifloxacin eye drops for two weeks, and tobramycin/dexamethasone eye ointment for one month | Post-operative medication |
| 9 | One day postoperative orthoptic assessment quiet eye, orthophoria | October 2024 |
| 10 | Two weeks post-surgery presented with pyogenic granuloma in the right eye Topical frequent prednisolone acetate 1% eye drops and Tobramycin/dexamethasone eye ointment |
November 2024 |
| 12 | Two months after medical treatment, the PG did not regress, so she was scheduled for surgery | Jan 2025 |
| 13 | Two weeks after the decision of surgery, the patient reported regression of the lesion, then two weeks later, the mass was wholly resolved, and medical treatment ensured compliance | January 2025 |
She underwent a bilateral medial rectus muscle recession of 6.0 mm using a fornix-based incision. Post-operative medication included prednisolone acetate 1% eye drops to be applied for both eyes in a tapering dose every one week over four weeks (every six hours, every eight hours, every twelve hours, and every twenty-four hours), moxifloxacin eye drops every eight hours for two weeks, and Tobramycin/Dexamethasone eye ointment is to be applied once at night for four weeks for both eyes. One day postoperatively, she was seen, and by orthoptic work-up, she was orthophoria with quiet eyes and mild subconjunctival injection and the wound site with no signs of infection. Two weeks postoperatively, the patient presented to the clinic complaining of a mass lesion pointing from the wound site of the right eye (Figure 1).
Figure 1: Pyogenic granuloma in the right eye two weeks following muscle surgery to treat esotropia
She had no pain, discharge, tenderness, or signs of infection. A slit-lamp examination showed a lobulated mass measured almost 10.00 mm by 10.00 mm. The wound was intact, and no scleral show or pointing sutures. The patient was inquired about the use of post-operative medication, and she responded that she had good compliance. She was diagnosed with a PG. The dose of prednisolone acetate eye drops was increased to every two hours while awake for two days, then every four hours while awake, to be tapered four times, three times, two times, and once, one week for each to the right eye. She was also educated about the use of tobramycin/dexamethasone eye ointment at night. Two months later, the lesion was mildly increased in size with the same redness. So, she was booked for surgical excision. After fixing the date of surgery, two weeks later, she reported that the redness improved, and the lesion started to shrink. One month later, the lesion had almost disappeared with a small residual (Figure 2).
Figure 2: The mass on the bulbar conjunctiva of the right eye was resolved within four weeks of medical treatment
The patient confirmed that she had never used the medications, and she just started using it after booking for surgery. Although her family was educated (the mother is a teacher, her brother is an optometrist, and her sister is a family physician), they were not aware of her poor compliance with medication. PG did not recur two months after the stoppage of medication.
3. DISCUSSION
This case report highlights that poor compliance with post-operative medications could be the most common cause of PG, which was not reported before in the literature and is secondary to irritation caused by the sutures at the wound site. In the present case, the teenage child did not reveal the stoppage of the topical application of prescribed medication, and her family was not aware of that. When the surgical approach was decided, two months after no improvement of the lesion, the fear of surgery resulted in judicious usage of the medication and complete resolution of the lesion noticed within four weeks.
Adherence to using topical post-operative medications is challenging. It is known that topical ocular medications usually cause discomfort because of the chemical composition of the medication. This might affect the patient's compliance, especially if there is a wound in the eye post-surgery or if the patient is an uncooperative child or teenager. Other factors can affect compliance, including the number of prescribed medications, frequency of dosing, the age of the patient, the caregiver compliance, patient or caregiver's belief about the medication, blurring of vision from using the ointment, the financial status of the family, trust of the physician, and the degree of understanding of the patient of how to use the medication.6 However, patients with eye conditions with medical and surgical treatment options often continue medical treatment to avoid surgery.
Usually, management of PG focuses on topical medications (topical steroids or topical beta-blockers), but surgical excision is indicated if the lesion is large or persistent. Other modalities of management include cryotherapy and laser ablation, which are sometimes complemented by immunosuppressant mechanisms like antimetabolite applications and steroid usage after excision.7,8
The development of PG after horizontal muscle surgery in the present case is uncommon. A previously published case of infected PG mimicking conjunctival abscess post-strabismus surgery in a young child that presented typically at the same time, two weeks after strabismus surgery.9 That child improved significantly with the proper use of topical steroids, which raises doubts about the compliance of the post-operative usage of the medications. In this case, signs, that indicate poor compliance with the post-operative medications include persistent redness in all follow-up visits and an increase in the size of the lesion, although she was prescribed frequent topical steroids. Although her family was educated and given written instructions on how to use the drops, and her medications were freely given because she was treated in a government hospital, she did not use the medication properly. Adherence to topical medication post-strabismus surgery has not been investigated before. The only available reports are about adherence to post-cataract surgery, to antiglaucoma medication, or to anti-inflammatory medication for uveitis.6,10,11 Poor compliance with post-cataract surgery has been shown to be 30%.6 Adherence to antiglaucoma medications was reported to be 54%.[8] Further studies are needed to investigate patient adherence to medications post-strabismus surgery.
4. CONCLUSION
In conclusion, PG can be prevented by properly educating patients about how to use and apply the medication, simplifying the dose regimen, and warning them about the possible complications of PG if medications are not used.
5. Conflict of interest
The author declares that there was no conflict of interest.
6. Ethical issues
Written informed consent was obtained from the patient to publish this report for the academic purposes.
7. Authors’ contribution
DHA was the sole author of this paper.
8. REFERENCES
- Kaleeny JD, Janis JE. Pyogenic granuloma diagnosis and management: a practical review. Plast Reconstr Surg Glob Open. 2024;12(9):e6160. [PubMed] DOI: 1097/GOX.0000000000006160
- Alrawashdeh HM, Naser AY, Alwafi H, Alyami MH, Khatatbeh M, Ahmed LA, et al. Trends in hospital admission due to diseases of the eye and adnexa in the past two decades in England and Wales: an ecological study. Int J Gen Med. 2022;15:1097–1110. [PubMed] DOI: 2147/IJGM.S344380
- Hassanin FF, Naser AY, Aalam WA, Hanbazazh M. Eye and adnexa hospitalization in Australia: an ecological study. Medicine (Baltimore). 2024;103(27):e38829. [PubMed] DOI: 1097/MD.0000000000038829
- Naqeeb MR, Naser AY. Postprocedural disorders of eye and adnexa admissions profile. Clin Optom (Auckl). 2023;15:261–270. [PubMed] DOI: 2147/OPTO.S437044
- Espinoza GM, Lueder GT. Conjunctival pyogenic granulomas after strabismus surgery. Ophthalmology. 2005;112(7):1283–1286. [PubMed] DOI: 1016/j.ophtha.2005.01.048
- Matossian C. Noncompliance with prescribed eyedrop regimens among patients undergoing cataract surgery—prevalence, consequences, and solutions. US Ophthalmic Rev. 2020;13:18. DOI: 17925/USOR.2020.13.1.18
- Bin Dlaim MS, Alhussein GA, Alqahtani RS, Almanea LT. Conservative management of giant pyogenic granuloma post strabismus surgery: a case report and literature review. Cureus. 2023;15(7):e41321. [PubMed] DOI: 7759/cureus.41321
- Huang YT, Lin SC, Huang LY, Chuang HY, Lin YJ, Chien KH, et al. Incidence, risk factors and management of postoperative complications in horizontal strabismus surgery. Semin Ophthalmol. 2024;39(2):143–149. [PubMed] DOI: 1080/08820538.2023.2275620
- AlHarkan DH, AlOdan HA. Infected conjunctival pyogenic granuloma at strabismus surgery site mimicking conjunctival abscess. Saudi J Ophthalmol. 2019;33(1):109–111. [PubMed] DOI: 1016/j.sjopt.2018.07.001
- Javidi H, Poonit N, Patel RP, Barry RJ, Rauz S, Murray PI. Adherence to topical medication in patients with inflammatory eye disease. Ocul Immunol Inflamm. 2021;29(5):890–895. [PubMed] DOI: 1080/09273948.2019.1699122
- Zaharia AC, Dumitrescu OM, Radu M, Rogoz RE. Adherence to therapy in glaucoma treatment—a review. J Pers Med. 2022;12(4). [PubMed] DOI: 3390/jpm12040514