Ony W. Angkejaya 1 , Sam Syahrony 2 , Sri Yunita 3 , Nurul H. DJ F. Ahmad 4 , Mujahidah R. Abdullah 5 , Christiana R. Titaley 6
Author affiliations:
Background & objective: Phlebotomy or venipuncture is a procedure that can cause moderate to severe pain in patients. This pain can be prevented with pharmacological and/or non-pharmacological methods. One of the pharmacological methods to reduce pain is local application of local anesthetic preparation. Topical lidocaine and Eutectic Mixture of Local Anesthetics (EMLA) cream containing 2.5% lidocaine and 2.5% prilocaine are local anesthetics that can be applied before phlebotomy. We compared alkalinized 2.46% lidocaine with 5% EMLA cream on the intensity of pain on venipuncture.
Methodology: This study used the analytical pre-experimental (pre-experiment) Randomized Control Trial (RCT) method with a group pretest-posttest design approach. The study measured the intervention by comparing the EMLA 5% group with the 2.64% lidocaine group. Lidocaine was alkalinized in 70% alcohol. Both drugs were applied topically before phlebotomy, and the numeric rating scales (NRS) were compared in student volunteers of the Medical Faculty of Pattimura University, Ambon, Maluku, Indonesia.
Results: The analysis of 20 paired respondents who were given a solution of 2.64% lidocaine alkalinized in 70% alcohol topically before phlebotomy on the first day and 5% EMLA cream topically before phlebotomy on the 10th day showed very significant results with P = 0.002.
Conclusion: The application of 5% EMLA cream topically has a greater analgesic effect, compared to 2.64% lidocaine alkalinized in 70% alcohol, when measured with NRS.
Abbreviations: EMLA: Eutectic Mixture of Local Anesthetics, RCT: Randomized Control Trial, NRS: Numeric Rating Scale, IASP: International Association for Study of Pain, VRS: Verbal Rating Scale, AVF: Arteriovenous Fistula
Keywords: EMLA; Lidocaine; Local Anesthetic; Numeric Rating Scale; Phlebotomy; Pain; Venipuncture; Verbal Rating Scale
Citation: Angkejaya OW, Syahrony S, Yunita S, Ahmad NHDJF, Abdullah MR, Titaley C. Comparison of analgesic effects of alkalinized 2.46% lidocaine versus 5% EMLA cream applied topically before phlebotomy. Anaesth. pain intensive care 2025;29(4):277-280. DOI: 10.35975/apic.v29i4.2851
Received: May 09, 2024; Revised: October 26, 2024; Accepted: January 01, 2025
Phlebotomy or Venipuncture is crucial for examining and treating persons in healthcare settings. The procedure involves accessing a vein to collect blood samples and administering intravenous medicines for quick results. Venipuncture can often cause anxiety and pain.1
The International Association for the Study of Pain (IASP) defines pain as an unpleasant sensory and emotional experience triggered by tissue damage.2
Local anesthetic is a medication that temporarily numbs a small body area before minor surgery. It can also be used to decrease pain before performing venipuncture.3 One of the medications for local anesthetic is lidocaine. Lidocaine inhibits Na+ channels, suppressing action potential and electric signal conduction in afferent sensory neurons. Alkalinization of lidocaine solution with sodium bicarbonate creates a nonionized lipophilic form, allowing the molecule to perform the necessary anesthetic effect.4
Another method that can be used is applying EMLA. It is a lipid emulsion created by mixing prilocaine (2.5%) and lignocaine (2.5%) at room temperature.5 Previous research suggests that using EMLA cream under occlusion for more than 60 minutes can penetrate the epidermis and reduce pain during venipuncture. It also has excellent cutaneous absorption.6
Since there is limited data on alkalinizing lidocaine and EMLA cream for venipuncture. This study aims to compare the efficacy of topical alkalinizing lidocaine and EMLA cream for pain relief before undergoing venipuncture.
This research will utilize a pre-experimental randomized controlled trial (RCT) analytical method with a group pretest-posttest design approach. It has been approved by the Research Ethics Committee of the Medical Faculty of Pattimura University, with registration number 023/FK-KOM.ETIK/VII/2024.
The study aimed to measure the effects of two different interventions by comparing the EMLA group with the 2.64% alkalized lidocaine in 70% alcohol applied topically before phlebotomy. The sampling technique employed was purposive sampling, and the minimum sample size is calculated using the Federer formula. A total of 20 samples was required, and the subjects were students from the Medical Faculty.
To prepare a 100 mL of 2.64% alkalinized lidocaine solution in 70% alcohol, the process began with isolating 73.6 mL of 95% alcohol using syringes. Next, 26.4 mL of 10% lidocaine solution was added and mixed into the alcohol solution. This lidocaine and alcohol solution were poured into the container. Subsequently, 0.5 mL of 8.4% sodium bicarbonate solution was taken using a 1 mL syringe and added dropwise at a rate of 1 drop per second while gently shaking the container to ensure homogeneity and prevent precipitation. Finally, the container is sealed tightly to prevent evaporation, labeled appropriately, and the 100 mL of 2.64% alkalinized lidocaine solution in 70% alcohol solution is ready to use.
Subjects were divided into two groups and received two different interventions alternatively, with a 10-day interval between them. The first intervention involved phlebotomy with local anesthesia using a solution of 10% lidocaine, alkalized with 8.4% sodium bicarbonate, and mixed with 95% alcohol. The second intervention involved phlebotomy with EMLA cream, which contained 2.5% lidocaine and 2.5% prilocaine.
Pain intensity was assessed with the NRS based on the patient's feedback after venipuncture. The collected data was analyzed using the Wilcoxon statistical test.
Statistical distribution of the NRS in the phlebotomy procedure with the administration of 2.64% lidocaine alkalinized in 70% alcohol topically.
The results of this study indicated that respondents who received topical lidocaine before phlebotomy reported moderate pain on the NRS, with 9 (45%) scoring between 4-7. Additionally, 8 (40%) reported mild pain with scores ranging from 1-3, while 3 (15%) experienced severe pain, scoring between 8-10.
In contrast, respondents who received 5% EMLA cream topically, 13 (65%) experienced mild pain, 4 (20%) reported moderate pain, and 3 (15%) indicated that they did not feel any pain at all.
The results of the analysis in 20 paired respondents who were given a solution of alkalinized lidocaine topically before phlebotomy on the first day and EMLA cream 5% topically before phlebotomy on day 10 showed very significant results from Wilcoxon test with a P = 0.002. cream 5% topically had a greater effect on NRS changes, compared to lidocaine.
The bar chart compares the distribution of pain levels during phlebotomy procedures for two types of pain management EMLA Cream 5% (black bars) and alkalized lidocaine (grey bars).
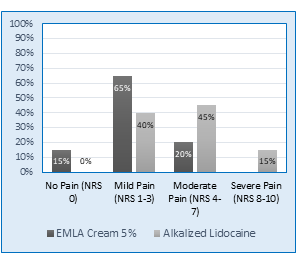
Figure 1: Comparative NRS scores in two study groups
Based on these results, the administration of EMLA cream 5% topically had a greater effect on NRS changes, compared to lidocaine 2.64% which was alkalized in 70% alcohol with a minimum-maximum value (0-2).
Studies by Oluwadun et al,7 found that EMLA cream (76.5%) and 10% lidocaine cream (70.6%) significantly reduced mild pain during cannulation compared to placebo (55.9%), as measured by the verbal rating scale (VRS). Additionally, other randomized controlled trials showed that EMLA cream was more effective than lidocaine tape in alleviating pain during arteriovenous fistula (AVF) punctures in patients on chronic maintenance dialysis.8
Based on these results, the administration of EMLA
cream, with 2.5% lignocaine and 2.5% prilocaine, effectively reduces intravenous cannulation pain in children and should be included in routine premedication for venipuncture.9
EMLA increases the threshold for nerve excitation, suppressing nerve impulse initiation and providing analgesia by targeting dermal free nerve endings. In this study, EMLA effectively lowered the pain threshold for referred muscle pain.7
Lidocaine and prilocaine are solid at room temperature, but mixing them in equimolar proportions lowers their melting point, resulting in a liquid formulation. This allows for a higher concentration of anesthetic in EMLA oil droplets, enhancing skin permeability and improving anesthetic effect.8
This research was conducted at a single location with a limited sample size, which restricts the generalizability of its findings to the broader population. Future studies should aim to include a larger sample size and multiple locations to enhance the validity of the results.
Topical administration of EMLA 5% cream has better analgesic effect on NRS changes, compared to 2.64% lidocaine alkalinized with 70% alcohol. Lidocaine and prilocaine, when mixed equimolar, form a liquid at room temperature, reducing the need for solubilizing agents and enabling a higher anesthetic concentration in EMLA. This results in enhanced skin permeability and effective anesthesia.
7. Data availability
The numerical data generated during this research is available with the authors.
8. Conflict of interest
All authors declare that there was no conflict of interest.
9. Funding
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Authors’ contribution
OWA: Corresponding author, Concept, conduct of the study
SR: Responsible for synopsis writing, literature search, manuscript writing
SY: Responsible for data collection.
NHDJA: Responsible for results analysis with the statistician
Author affiliations:
- Ony W. Angkejaya, Departement of Anaesthesia, Intensive Care and Pain Management, Medical Faculty, Pattimura University, Ambon, Indonesia; E-mail: Lenovovonel1982@gmail.com
- Sam Syahrony, Departement of Anaesthesia, Intensive Care and Pain Management, Medical Faculty, Pattimura University, Ambon, Indonesia; E-mail: Syahronmaskat@gmail.com
- Sri Yunita, Departement of Anaesthesia, Intensive Care and Pain Management, Medical Faculty, Pattimura University, Ambon, Indonesia; E-mail: Sryunita1998@gmail.com
- Nurul H. DJ Ahmad, Departement of Anaesthesia, Intensive Care and Pain Management, Medical Faculty, Pattimura University, Ambon, Indonesia; E-mail: Nurul.hasyana@gmail.com
- Mujahidah R. Abdullah, Departement of Anaesthesia, Intensive Care and Pain Management, Medical Faculty, Pattimura University, Ambon, Indonesia; E-mail: Rofifahmujahidah@gmail.com
- Christiana Rialine Titaley, Departement of Public Health, Medical Faculty, Pattimura University, Ambon, Indonesia; E-mail: christiana_rialine@yahoo.com
ABSTRACT
Background & objective: Phlebotomy or venipuncture is a procedure that can cause moderate to severe pain in patients. This pain can be prevented with pharmacological and/or non-pharmacological methods. One of the pharmacological methods to reduce pain is local application of local anesthetic preparation. Topical lidocaine and Eutectic Mixture of Local Anesthetics (EMLA) cream containing 2.5% lidocaine and 2.5% prilocaine are local anesthetics that can be applied before phlebotomy. We compared alkalinized 2.46% lidocaine with 5% EMLA cream on the intensity of pain on venipuncture.
Methodology: This study used the analytical pre-experimental (pre-experiment) Randomized Control Trial (RCT) method with a group pretest-posttest design approach. The study measured the intervention by comparing the EMLA 5% group with the 2.64% lidocaine group. Lidocaine was alkalinized in 70% alcohol. Both drugs were applied topically before phlebotomy, and the numeric rating scales (NRS) were compared in student volunteers of the Medical Faculty of Pattimura University, Ambon, Maluku, Indonesia.
Results: The analysis of 20 paired respondents who were given a solution of 2.64% lidocaine alkalinized in 70% alcohol topically before phlebotomy on the first day and 5% EMLA cream topically before phlebotomy on the 10th day showed very significant results with P = 0.002.
Conclusion: The application of 5% EMLA cream topically has a greater analgesic effect, compared to 2.64% lidocaine alkalinized in 70% alcohol, when measured with NRS.
Abbreviations: EMLA: Eutectic Mixture of Local Anesthetics, RCT: Randomized Control Trial, NRS: Numeric Rating Scale, IASP: International Association for Study of Pain, VRS: Verbal Rating Scale, AVF: Arteriovenous Fistula
Keywords: EMLA; Lidocaine; Local Anesthetic; Numeric Rating Scale; Phlebotomy; Pain; Venipuncture; Verbal Rating Scale
Citation: Angkejaya OW, Syahrony S, Yunita S, Ahmad NHDJF, Abdullah MR, Titaley C. Comparison of analgesic effects of alkalinized 2.46% lidocaine versus 5% EMLA cream applied topically before phlebotomy. Anaesth. pain intensive care 2025;29(4):277-280. DOI: 10.35975/apic.v29i4.2851
Received: May 09, 2024; Revised: October 26, 2024; Accepted: January 01, 2025
1. INTRODUCTION
Phlebotomy or Venipuncture is crucial for examining and treating persons in healthcare settings. The procedure involves accessing a vein to collect blood samples and administering intravenous medicines for quick results. Venipuncture can often cause anxiety and pain.1
The International Association for the Study of Pain (IASP) defines pain as an unpleasant sensory and emotional experience triggered by tissue damage.2
Local anesthetic is a medication that temporarily numbs a small body area before minor surgery. It can also be used to decrease pain before performing venipuncture.3 One of the medications for local anesthetic is lidocaine. Lidocaine inhibits Na+ channels, suppressing action potential and electric signal conduction in afferent sensory neurons. Alkalinization of lidocaine solution with sodium bicarbonate creates a nonionized lipophilic form, allowing the molecule to perform the necessary anesthetic effect.4
Another method that can be used is applying EMLA. It is a lipid emulsion created by mixing prilocaine (2.5%) and lignocaine (2.5%) at room temperature.5 Previous research suggests that using EMLA cream under occlusion for more than 60 minutes can penetrate the epidermis and reduce pain during venipuncture. It also has excellent cutaneous absorption.6
Since there is limited data on alkalinizing lidocaine and EMLA cream for venipuncture. This study aims to compare the efficacy of topical alkalinizing lidocaine and EMLA cream for pain relief before undergoing venipuncture.
2. METHODOLOGY
This research will utilize a pre-experimental randomized controlled trial (RCT) analytical method with a group pretest-posttest design approach. It has been approved by the Research Ethics Committee of the Medical Faculty of Pattimura University, with registration number 023/FK-KOM.ETIK/VII/2024.
The study aimed to measure the effects of two different interventions by comparing the EMLA group with the 2.64% alkalized lidocaine in 70% alcohol applied topically before phlebotomy. The sampling technique employed was purposive sampling, and the minimum sample size is calculated using the Federer formula. A total of 20 samples was required, and the subjects were students from the Medical Faculty.
To prepare a 100 mL of 2.64% alkalinized lidocaine solution in 70% alcohol, the process began with isolating 73.6 mL of 95% alcohol using syringes. Next, 26.4 mL of 10% lidocaine solution was added and mixed into the alcohol solution. This lidocaine and alcohol solution were poured into the container. Subsequently, 0.5 mL of 8.4% sodium bicarbonate solution was taken using a 1 mL syringe and added dropwise at a rate of 1 drop per second while gently shaking the container to ensure homogeneity and prevent precipitation. Finally, the container is sealed tightly to prevent evaporation, labeled appropriately, and the 100 mL of 2.64% alkalinized lidocaine solution in 70% alcohol solution is ready to use.
Subjects were divided into two groups and received two different interventions alternatively, with a 10-day interval between them. The first intervention involved phlebotomy with local anesthesia using a solution of 10% lidocaine, alkalized with 8.4% sodium bicarbonate, and mixed with 95% alcohol. The second intervention involved phlebotomy with EMLA cream, which contained 2.5% lidocaine and 2.5% prilocaine.
Pain intensity was assessed with the NRS based on the patient's feedback after venipuncture. The collected data was analyzed using the Wilcoxon statistical test.
3. RESULTS
Statistical distribution of the NRS in the phlebotomy procedure with the administration of 2.64% lidocaine alkalinized in 70% alcohol topically.
The results of this study indicated that respondents who received topical lidocaine before phlebotomy reported moderate pain on the NRS, with 9 (45%) scoring between 4-7. Additionally, 8 (40%) reported mild pain with scores ranging from 1-3, while 3 (15%) experienced severe pain, scoring between 8-10.
| Table 1: Demographic characteristics of all respondents (n = 20) | |
| Variable | N (%) |
| Gender | |
| · Male | 3 (15) |
| · Female | 17 (85) |
| Age | |
| · 17 | 3 (15) |
| · 18 | 11 (55) |
| · 19 | 2 (10) |
| · 20 | 2 (10) |
| · 21 | 2 (10) |
| Injection Location | |
| · Fossa antekubiti dextra | 8 (40) |
| · Fossa antekubiti sinistra | 10 (50) |
| · Manus sinistra | 2 (10) |
| History of Wounds at the Location of Phlebotomy | 0 (100) |
| History of drug and food allergies | 0 (100) |
In contrast, respondents who received 5% EMLA cream topically, 13 (65%) experienced mild pain, 4 (20%) reported moderate pain, and 3 (15%) indicated that they did not feel any pain at all.
| Table 2: Comparison of pain scores between the two groups | |||
| Pain Score (NRS) | EMLA 5% | Alkalinized Lidocaine | P-Value |
| 0 (No Pain) | 3 (15) | 0 (0) | |
| 1-3 (Mild Pain) | 13 (65) | 8 (40) | |
| 4-7 (Moderate Pain) | 4 (20) | 9 (45) | 0.002* |
| 8-10 (Severe Pain) | 0 (0) | 3 (15) | |
| Total | 20 (100) | 20 (100) | |
| Data presented as n (%); P < 0.05 considered as significant | |||
The results of the analysis in 20 paired respondents who were given a solution of alkalinized lidocaine topically before phlebotomy on the first day and EMLA cream 5% topically before phlebotomy on day 10 showed very significant results from Wilcoxon test with a P = 0.002. cream 5% topically had a greater effect on NRS changes, compared to lidocaine.
The bar chart compares the distribution of pain levels during phlebotomy procedures for two types of pain management EMLA Cream 5% (black bars) and alkalized lidocaine (grey bars).
Figure 1: Comparative NRS scores in two study groups
4. DISCUSSION
Based on these results, the administration of EMLA cream 5% topically had a greater effect on NRS changes, compared to lidocaine 2.64% which was alkalized in 70% alcohol with a minimum-maximum value (0-2).
Studies by Oluwadun et al,7 found that EMLA cream (76.5%) and 10% lidocaine cream (70.6%) significantly reduced mild pain during cannulation compared to placebo (55.9%), as measured by the verbal rating scale (VRS). Additionally, other randomized controlled trials showed that EMLA cream was more effective than lidocaine tape in alleviating pain during arteriovenous fistula (AVF) punctures in patients on chronic maintenance dialysis.8
Based on these results, the administration of EMLA
cream, with 2.5% lignocaine and 2.5% prilocaine, effectively reduces intravenous cannulation pain in children and should be included in routine premedication for venipuncture.9
EMLA increases the threshold for nerve excitation, suppressing nerve impulse initiation and providing analgesia by targeting dermal free nerve endings. In this study, EMLA effectively lowered the pain threshold for referred muscle pain.7
Lidocaine and prilocaine are solid at room temperature, but mixing them in equimolar proportions lowers their melting point, resulting in a liquid formulation. This allows for a higher concentration of anesthetic in EMLA oil droplets, enhancing skin permeability and improving anesthetic effect.8
5. LIMITATIONS
This research was conducted at a single location with a limited sample size, which restricts the generalizability of its findings to the broader population. Future studies should aim to include a larger sample size and multiple locations to enhance the validity of the results.
6. CONCLUSION
Topical administration of EMLA 5% cream has better analgesic effect on NRS changes, compared to 2.64% lidocaine alkalinized with 70% alcohol. Lidocaine and prilocaine, when mixed equimolar, form a liquid at room temperature, reducing the need for solubilizing agents and enabling a higher anesthetic concentration in EMLA. This results in enhanced skin permeability and effective anesthesia.
7. Data availability
The numerical data generated during this research is available with the authors.
8. Conflict of interest
All authors declare that there was no conflict of interest.
9. Funding
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Authors’ contribution
OWA: Corresponding author, Concept, conduct of the study
SR: Responsible for synopsis writing, literature search, manuscript writing
SY: Responsible for data collection.
NHDJA: Responsible for results analysis with the statistician
REFERENCES
- Hur MH, Choi HS. Effects of a thermoelectric element band on venipuncture-associated pain and anxiety: a randomized controlled trial. Asian Nurs Res. 2021;15(5):337-44. [PubMed] DOI: 1016/j.anr.2021.12.003
- Wang J, Doan LV. Clinical pain management: current practice and recent innovations in research. Cell Rep Med. 2024;5(10):101786. [PubMed] DOI: 1016/j.xcrm.2024.101786
- Bahar E, Yoon H. Lidocaine: a local anesthetic, its adverse effects and management. Medicina. 2021;57(8):782. [PubMed] DOI: 3390/medicina57080782
- Pereira e Silva R, Ponte C, Lopes F, Palma dos Reis J. Alkalinized lidocaine solution as a first-line local anesthesia protocol for intradetrusor injection of onabotulinum toxin A: results from a double-blinded randomized controlled trial. Neurourol Urodyn. 2020;39(8):2471-9. [PubMed] DOI: 1002/nau.24519
- Huang Y, Chai S, Wang D, Li W, Zhang X. Efficacy of eutectic mixture of local anesthetics on pain control during extracorporeal shock wave lithotripsy: a systematic review and meta-analysis. Med Sci Monit. 2020;26:e921063. [PubMed] DOI: 12659/MSM.921063
- Lillieborg S, Aanderud L. EMLA anesthetic cream for debridement of burns: a study of plasma concentrations of lidocaine and prilocaine and a review of the literature. Int J Burns Trauma. 2017;7(6):88-97. [PubMed]
- Kim JE, Kim JY, Lee HS, Seok S, Kil HK. Analgesic effect of trigger point injection and EMLA for shoulder pain in patients undergoing total laparoscopic hysterectomy. Medicine (Baltimore). 2019;98(2):e14087. [PubMed] DOI: 1097/MD.0000000000014087
- Fujimoto K, Adachi H, Yamazaki K, Nomura K, Saito A, Matsumoto Y, et al. Comparison of the pain-reducing effects of EMLA cream and lidocaine tape during arteriovenous fistula puncture in patients undergoing hemodialysis: a multi-center, open-label, randomized crossover trial. PLoS One. 2020;15(3):1-13. [PubMed] DOI: 1371/journal.pone.0230372