Tomoki Nishiyama, MD, PhD
Department of Anesthesiology, Shinagawa Shishokai Hospital, 1-29-7, Kita-Shinagawa, Shinagawa, Tokyo, 140-0001, (Japan)
Correspondence:
Tomoki Nishiyama, MD, PhD, Department of Anesthesiology, Shinagawa Shishokai Hospital, 1-29-7, Kita-Shinagawa, Shinagawa, Tokyo, 140-0001, (Japan); Tel: +81-3-5781-0700; E-mail: nishit-tky@umin.ac.jp
ABSTRACT
Objective:
Postoperative analgesic effects of paravertebral block in mastectomy is still controversial. The purpose of the present study was to investigate the effectiveness of paravertebral block when given in addition to general anesthesia (GA), and whether a larger single dose or multilevel injections at successive levels are more useful for postoperative analgesia in mastectomy with lymph node dissection.
Methodology:
This randomized controlled non-blind study was undertken at operating rooms and the indoor facilities at our university hospital. Sixty female patients aged 40 to 65 years, ASA physical status I and II, for partial mastectomy with axillary lymph node dissection were included in the study after ethical committee approval. The patients were divided into three groups; control, single or multilevel block groups.
Before GA, in the single block group, paravertebral block using 0.5% ropivacaine 15 ml was performed at T4 level, and in the multilevel group, paravertebral block was performed at T3, 4, and 5 levels with 0.5% ropivacaine 5 ml each. In the control group, no block was performed. GA was induced with midazolam, fentanyl, propofol, and vecuronium. Laryngeal mask airway #3 was inserted. Anesthesia was maintained with propofol infusion and intermittent fentanyl as necessary under 50% nitrous oxide in oxygen (total flow 4 L/min). For postoperative analgesia, pentazocine 15 mg was administered intramuscularly as patients’ request.
Measurements:
The dose of fentanyl used during surgery, frequency of pentazocine request in postoperative 24 hours, time to the first pentazocine administration, and postoperative pain measured by visual analogue scale (VAS, 0 to10) for 24 hours were compared among the groups.
Results:
Dose of fentanyl during surgery was significantly larger in the control group than the single and multilevel groups. Frequency of postoperative pentazocine administration was significantly larger in the control group than the single and multilevel groups. There were no differences in the dose of fentanyl and frequency of pentazocine administration between the single and multilevel groups.
Conclusion.
Single large dose paravertebral block at T4 is equally useful for postoperative analgesia in mastectomy with lymph nodes dissection when compared to multilevel blocks at T3 to T5.
Key words:
Mastectomy; Paravertebral block; Postoperative pain; Single level block; Multilevel level blocks
Citation:
Nishiyama T. Effects of single or multilevel injection of paravertebral block on postoperative analgesia in partial mastectomy with lymph nodes dissection. Anaesth Pain & Intensive Care 2015;19(4):463-467
INTRODUCTION
Breast cancer is a big health problem for women, and after mastectomy they may suffer from severe postoperative pain if not unrelieved.(1) It is customary to use opioids or non-steroidal anti-inflammatory agents (NSAIDs) in these patients for postoperative analgesia. However, analgesic effects of these agents are limited, and opioid use is associated with frequent nausea, vomiting and constipation.
There are many studies which investigated the effects of paravertebral block on postoperative pain in mastectomy. However, whether paravertebral block is better than parenteral administration of opioids or NSAIDs for postoperative analgesia is still controversial.(2-4). In addition one more question remains unsettled; whether multilevel injections for paravertebral block are necessary or a single injection is enough.(3,5,6)
The primary objective of the present study was to investigate whether adding paravertebral block to general anesthesia (GA) is more effective for postoperative analgesia. As a secondary objective we compared single or multilevel paravertebral block for postoperative analgesia in mastectomy with lymph nodes dissection.
METHODOLOGY After the approval of the ethics committee of the hospital and informed consent from the patients, 60 female patients aged 40 to 65 years, ASA physical status I and II, for partial mastectomy with axillary lymph nodes dissection were enrolled in this study. Those who had allergy to local anesthetics, liver, renal, heart, lung, or brain disease, those with known drug abuse, or those with body mass index > 30 were excluded. They were randomly divided into three groups; control, single, and multilevel groups with 20 patients each by a sealed envelope technique on the day of surgery.
No premedication was administered. Before induction of GA, in the single block group, paravertebral block was performed at T4 level using 0.5% ropivacaine 15 ml, and in the multilevel group, paravertebral block was performed at T3, 4, and T5 levels using 5 ml of 0.5% ropivacaine at each level. In both groups the block was performed with loss of resistance under ultrasonography guidance. In the control group no block was performed.
In all of the three groups, GA was induced with midazolam 0.05 mg/kg, fentanyl 2 μg/kg, propofol 2 mg/kg and vecuronium 0.1 mg/kg. Laryngeal mask airway #3 was inserted. Anesthesia was maintained with propofol 5 to 7 mg/kg/h and intermittent fentanyl 50 μg as necessary by each anesthesiologist who did not know the intervention before surgery under 50% nitrous oxide in oxygen (total flow 4L/min).
For postoperative analgesia, pentazocine 15 mg was administered intramuscularly as patients’ request.
The dose of fentanyl used during surgery, frequency of pentazocine request in postoperative 24 hours, time to the first pentazocine administration, and postoperative pain measured by visual analogue scale (VAS 0 to10) for 24 hours were compared among the groups. Time spent for the block was compared between the single and multilevel groups.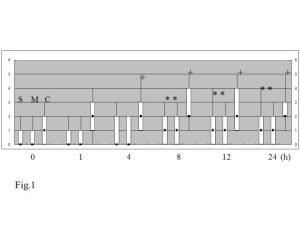 Figure 1: VAS score
Figure 1: VAS score
Longitudinal line shows VAS score (0 – 10), and horizontal line shows time.
S, single block group; M, multilevel group; C, control group
*: P < 0.05 vs. the control group; +: P < 0.05 vs. the value at time 0
Power analysis was performed to detect the intra- and inter-group differences of VAS scores with power of 0.80 and effect size of 0.3 using the G PowerTM software (University Mannheim, Germany). It showed that 55 patients were necessary, therefore, we enrolled 60 patients.
Statistical analysis was performed with factorial analysis of variance for demographic data, and the Kruskal Wallis test followed by Mann-Whitney U test for dose of fentanyl, frequency of pentazocine, and VAS score. The p value less than 0.05 was considered to be statistically significant.
RESULTS
Data were expressed as mean ± SD, median and range or number. Demographic data were not different among the groups (Table 1).
Table 1: Demographic data (Mean ± SD
Dose of fentanyl during surgery was significantly larger in the control group than the single and multilevel groups (Table 2).
Table 2: Analgesics used
Median with range in the parenthesis, *: P < 0.0001 vs. the Control group
Frequency of postoperative pentazocine administration was significantly larger in the control group than the single and multilevel groups (Table 2). There were no differences in the dose of fentanyl and frequency of pentazocine administration between the single and multilevel groups. Time spent for the block was 5.3 ± 1.1 min in the single block group and 12.2 ± 2.3 min in the multilevel group (P < 0.0001). Time to the first pentazocine administration was 3.5 ± 4.5 h in the control group, 13.7 ± 5.8 h in the single block group (P < 0.0001 vs. the control group), and 14.2 ± 3.7 h in the multilevel group (P < 0.0001 vs. the control group).
DISCUSSION
The present results showed that paravertebral block was effective to decrease anesthetics during surgery and for postoperative analgesia. Single injection was better than multilevel injections because the effects were the same but time for the block was shorter.
There are some limitations in this study. By design, we did not check loss of sensation by cold or pin prick stimuli, therefore, the success of the block was not confirmed. However, from the results, no patients showed quite different postoperative analgesic data, therefore, we assumed that the block was successful in all patients. Administration of fentanyl during surgery depended on the anesthesiologists not by strict criteria. Therefore, the difference of fentanyl dose was weak to confirm the effects of the block.
In the meta-analysis, paravertebral block had better postoperative analgesia than GA in breast surgery.(4). However, Abdallah et al(3) reported that paravertebral block from T1 to T5 with 5 ml of 0.5% ropivacaine each did not prolong the time to first request of postoperative rescue analgesic compared to GA. However, they included simple mastectomy, modified radical mastectomy, mastectomy with implant insertion, etc. The block from T1 to T5 might not be enough for some surgical procedures in their study. Paravertebral block at T3 to T6 was effective for mastectomy without axillary lymph node dissection,(5) while Buckenmaier et al(6) showed that the block at T1 to T6 was adequate for mastectomy with axillary lymph nodes dissection. Our results showed that blocks at T3 to T5 were enough for mastectomy with axillary lymph nodes dissection. Even a single block at T4 was as effective as multilevel blocks in our study. Sensory analgesia from 1 to 8 dermatomes after a single injection of 0.5% bupivacaine 15 ml for paravertebral block has been reported.(7) Therefore, single block at T4 with 15 ml might block the same area as the blocks at T3 to T5 with 5 ml each in our results.
Some studies showed that postoperative analgesia lasted for less than 6 hours with paravertebral block using bupivacaine or ropivacaine with or without epinephrine.(5,8-11) Longer duration of postoperative analgesia has also been reported. Boughey et al reported that paravertebral block at T1 to T6 with 3 to 6 ml 0.5% to 1% ropiavcaine and epinephrine at each level showed postoperative analgesia for at least 8 hours.(12) Single paravertebral block with 0.5% ropivacaine 20 ml with epinephrine had postoperative analgesia on the day of surgery but not on the next day.(13) Klein et al (14) showed that the effects continued for 72 hours. Our results showed postoperative analgesia for 12 to 13 hours by single or multilevel paravertebral block with 0.5% ropivacaine. From these reports and our results, duration of postoperative analgesia might depend on multiple factors, such as surgical procedure, surgical skills, and patients’ characteristics etc, but not on the level of the block and local anesthetic used.
We did not use continuous paravertebral block because it is reported that continuous paravertebral block has no merit over single shot paravertebral block in breast cancer surgery in postoperative analgesia.(6)
Paravertebral block has other advantages. It decreased nausea and vomiting in comparison with GA alone,(11,15) while it is shown that adding paravertebral block has no advantage in postoperative nausea, and vomiting compared with GA alone in breast cancer surgery.(2) Single paravertebral block at T3 with 0.5% bupivacaine reduced chronic pain 1 year after breast cancer surgery.(16) A retrospective study (17) showed paravertebral block with GA decreased cancer recurrence in patients received mastectomy and lymph nodes dissection than GA alone. We did not check these other effects in the present study.
CONCLUSION
In conclusion, single paravertebral block at T4 is equally useful for postoperative analgesia in mastectomy with lymph nodes dissection as are three separate multilevel blocks at T3 to T5 with smaller doses.
REFERENCES
Department of Anesthesiology, Shinagawa Shishokai Hospital, 1-29-7, Kita-Shinagawa, Shinagawa, Tokyo, 140-0001, (Japan)
Correspondence:
Tomoki Nishiyama, MD, PhD, Department of Anesthesiology, Shinagawa Shishokai Hospital, 1-29-7, Kita-Shinagawa, Shinagawa, Tokyo, 140-0001, (Japan); Tel: +81-3-5781-0700; E-mail: nishit-tky@umin.ac.jp
ABSTRACT
Objective:
Postoperative analgesic effects of paravertebral block in mastectomy is still controversial. The purpose of the present study was to investigate the effectiveness of paravertebral block when given in addition to general anesthesia (GA), and whether a larger single dose or multilevel injections at successive levels are more useful for postoperative analgesia in mastectomy with lymph node dissection.
Methodology:
This randomized controlled non-blind study was undertken at operating rooms and the indoor facilities at our university hospital. Sixty female patients aged 40 to 65 years, ASA physical status I and II, for partial mastectomy with axillary lymph node dissection were included in the study after ethical committee approval. The patients were divided into three groups; control, single or multilevel block groups.
Before GA, in the single block group, paravertebral block using 0.5% ropivacaine 15 ml was performed at T4 level, and in the multilevel group, paravertebral block was performed at T3, 4, and 5 levels with 0.5% ropivacaine 5 ml each. In the control group, no block was performed. GA was induced with midazolam, fentanyl, propofol, and vecuronium. Laryngeal mask airway #3 was inserted. Anesthesia was maintained with propofol infusion and intermittent fentanyl as necessary under 50% nitrous oxide in oxygen (total flow 4 L/min). For postoperative analgesia, pentazocine 15 mg was administered intramuscularly as patients’ request.
Measurements:
The dose of fentanyl used during surgery, frequency of pentazocine request in postoperative 24 hours, time to the first pentazocine administration, and postoperative pain measured by visual analogue scale (VAS, 0 to10) for 24 hours were compared among the groups.
Results:
Dose of fentanyl during surgery was significantly larger in the control group than the single and multilevel groups. Frequency of postoperative pentazocine administration was significantly larger in the control group than the single and multilevel groups. There were no differences in the dose of fentanyl and frequency of pentazocine administration between the single and multilevel groups.
Conclusion.
Single large dose paravertebral block at T4 is equally useful for postoperative analgesia in mastectomy with lymph nodes dissection when compared to multilevel blocks at T3 to T5.
Key words:
Mastectomy; Paravertebral block; Postoperative pain; Single level block; Multilevel level blocks
Citation:
Nishiyama T. Effects of single or multilevel injection of paravertebral block on postoperative analgesia in partial mastectomy with lymph nodes dissection. Anaesth Pain & Intensive Care 2015;19(4):463-467
INTRODUCTION
Breast cancer is a big health problem for women, and after mastectomy they may suffer from severe postoperative pain if not unrelieved.(1) It is customary to use opioids or non-steroidal anti-inflammatory agents (NSAIDs) in these patients for postoperative analgesia. However, analgesic effects of these agents are limited, and opioid use is associated with frequent nausea, vomiting and constipation.
There are many studies which investigated the effects of paravertebral block on postoperative pain in mastectomy. However, whether paravertebral block is better than parenteral administration of opioids or NSAIDs for postoperative analgesia is still controversial.(2-4). In addition one more question remains unsettled; whether multilevel injections for paravertebral block are necessary or a single injection is enough.(3,5,6)
The primary objective of the present study was to investigate whether adding paravertebral block to general anesthesia (GA) is more effective for postoperative analgesia. As a secondary objective we compared single or multilevel paravertebral block for postoperative analgesia in mastectomy with lymph nodes dissection.
METHODOLOGY After the approval of the ethics committee of the hospital and informed consent from the patients, 60 female patients aged 40 to 65 years, ASA physical status I and II, for partial mastectomy with axillary lymph nodes dissection were enrolled in this study. Those who had allergy to local anesthetics, liver, renal, heart, lung, or brain disease, those with known drug abuse, or those with body mass index > 30 were excluded. They were randomly divided into three groups; control, single, and multilevel groups with 20 patients each by a sealed envelope technique on the day of surgery.
No premedication was administered. Before induction of GA, in the single block group, paravertebral block was performed at T4 level using 0.5% ropivacaine 15 ml, and in the multilevel group, paravertebral block was performed at T3, 4, and T5 levels using 5 ml of 0.5% ropivacaine at each level. In both groups the block was performed with loss of resistance under ultrasonography guidance. In the control group no block was performed.
In all of the three groups, GA was induced with midazolam 0.05 mg/kg, fentanyl 2 μg/kg, propofol 2 mg/kg and vecuronium 0.1 mg/kg. Laryngeal mask airway #3 was inserted. Anesthesia was maintained with propofol 5 to 7 mg/kg/h and intermittent fentanyl 50 μg as necessary by each anesthesiologist who did not know the intervention before surgery under 50% nitrous oxide in oxygen (total flow 4L/min).
For postoperative analgesia, pentazocine 15 mg was administered intramuscularly as patients’ request.
The dose of fentanyl used during surgery, frequency of pentazocine request in postoperative 24 hours, time to the first pentazocine administration, and postoperative pain measured by visual analogue scale (VAS 0 to10) for 24 hours were compared among the groups. Time spent for the block was compared between the single and multilevel groups.
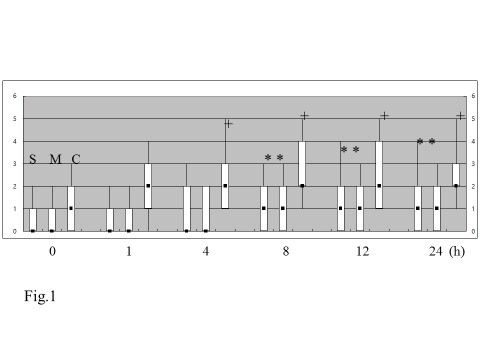 Figure 1: VAS score
Figure 1: VAS score
Longitudinal line shows VAS score (0 – 10), and horizontal line shows time.
S, single block group; M, multilevel group; C, control group
*: P < 0.05 vs. the control group; +: P < 0.05 vs. the value at time 0
Power analysis was performed to detect the intra- and inter-group differences of VAS scores with power of 0.80 and effect size of 0.3 using the G PowerTM software (University Mannheim, Germany). It showed that 55 patients were necessary, therefore, we enrolled 60 patients.
Statistical analysis was performed with factorial analysis of variance for demographic data, and the Kruskal Wallis test followed by Mann-Whitney U test for dose of fentanyl, frequency of pentazocine, and VAS score. The p value less than 0.05 was considered to be statistically significant.
RESULTS
Data were expressed as mean ± SD, median and range or number. Demographic data were not different among the groups (Table 1).
Table 1: Demographic data (Mean ± SD
| Parameters | Groups | ||
| Control | Single | Multilevel | |
| Age (years) | 54 ± 6 | 55 ± 5 | 55 ± 8 |
| Body weight (kg) | 59 ± 5 | 58 ± 4 | 58 ± 7 |
| Height (cm) | 155 ± 5 | 154 ± 4 | 157 ± 6 |
| Duration of surgery (min) | 122 ± 19 | 114 ± 21 | 111 ± 23 |
Dose of fentanyl during surgery was significantly larger in the control group than the single and multilevel groups (Table 2).
Table 2: Analgesics used
| Parameters | Groups | ||
| Control | Single | Multilevel | |
| Dose of fentanyl during surgery (μg) | 175 (100 – 250) | 50 (0 – 150)* | 50 (0 – 150)* |
| Frequency of pentazocine (times/24hours) | 1 (1 – 3) | 0 (0 – 1)* | 0 (0 – 1)* |
Frequency of postoperative pentazocine administration was significantly larger in the control group than the single and multilevel groups (Table 2). There were no differences in the dose of fentanyl and frequency of pentazocine administration between the single and multilevel groups. Time spent for the block was 5.3 ± 1.1 min in the single block group and 12.2 ± 2.3 min in the multilevel group (P < 0.0001). Time to the first pentazocine administration was 3.5 ± 4.5 h in the control group, 13.7 ± 5.8 h in the single block group (P < 0.0001 vs. the control group), and 14.2 ± 3.7 h in the multilevel group (P < 0.0001 vs. the control group).
DISCUSSION
The present results showed that paravertebral block was effective to decrease anesthetics during surgery and for postoperative analgesia. Single injection was better than multilevel injections because the effects were the same but time for the block was shorter.
There are some limitations in this study. By design, we did not check loss of sensation by cold or pin prick stimuli, therefore, the success of the block was not confirmed. However, from the results, no patients showed quite different postoperative analgesic data, therefore, we assumed that the block was successful in all patients. Administration of fentanyl during surgery depended on the anesthesiologists not by strict criteria. Therefore, the difference of fentanyl dose was weak to confirm the effects of the block.
In the meta-analysis, paravertebral block had better postoperative analgesia than GA in breast surgery.(4). However, Abdallah et al(3) reported that paravertebral block from T1 to T5 with 5 ml of 0.5% ropivacaine each did not prolong the time to first request of postoperative rescue analgesic compared to GA. However, they included simple mastectomy, modified radical mastectomy, mastectomy with implant insertion, etc. The block from T1 to T5 might not be enough for some surgical procedures in their study. Paravertebral block at T3 to T6 was effective for mastectomy without axillary lymph node dissection,(5) while Buckenmaier et al(6) showed that the block at T1 to T6 was adequate for mastectomy with axillary lymph nodes dissection. Our results showed that blocks at T3 to T5 were enough for mastectomy with axillary lymph nodes dissection. Even a single block at T4 was as effective as multilevel blocks in our study. Sensory analgesia from 1 to 8 dermatomes after a single injection of 0.5% bupivacaine 15 ml for paravertebral block has been reported.(7) Therefore, single block at T4 with 15 ml might block the same area as the blocks at T3 to T5 with 5 ml each in our results.
Some studies showed that postoperative analgesia lasted for less than 6 hours with paravertebral block using bupivacaine or ropivacaine with or without epinephrine.(5,8-11) Longer duration of postoperative analgesia has also been reported. Boughey et al reported that paravertebral block at T1 to T6 with 3 to 6 ml 0.5% to 1% ropiavcaine and epinephrine at each level showed postoperative analgesia for at least 8 hours.(12) Single paravertebral block with 0.5% ropivacaine 20 ml with epinephrine had postoperative analgesia on the day of surgery but not on the next day.(13) Klein et al (14) showed that the effects continued for 72 hours. Our results showed postoperative analgesia for 12 to 13 hours by single or multilevel paravertebral block with 0.5% ropivacaine. From these reports and our results, duration of postoperative analgesia might depend on multiple factors, such as surgical procedure, surgical skills, and patients’ characteristics etc, but not on the level of the block and local anesthetic used.
We did not use continuous paravertebral block because it is reported that continuous paravertebral block has no merit over single shot paravertebral block in breast cancer surgery in postoperative analgesia.(6)
Paravertebral block has other advantages. It decreased nausea and vomiting in comparison with GA alone,(11,15) while it is shown that adding paravertebral block has no advantage in postoperative nausea, and vomiting compared with GA alone in breast cancer surgery.(2) Single paravertebral block at T3 with 0.5% bupivacaine reduced chronic pain 1 year after breast cancer surgery.(16) A retrospective study (17) showed paravertebral block with GA decreased cancer recurrence in patients received mastectomy and lymph nodes dissection than GA alone. We did not check these other effects in the present study.
CONCLUSION
In conclusion, single paravertebral block at T4 is equally useful for postoperative analgesia in mastectomy with lymph nodes dissection as are three separate multilevel blocks at T3 to T5 with smaller doses.
REFERENCES
- Cepeda MS, Africano JM, Polo R, Alcala R, Carr DB. What decline in pain intensity is meaningful to patients with acute pain ? Pain 2003;105:151-157.
- Aufforth R, Jain J, Morreale J, Baumgarten R, Falk J, Wesen C. Paravertebral blocks in breast cancer surgery: Is there a difference in postoperative pain, nausea, and vomiting ? Ann Surg Oncol 2012;19:548-552.
- Abdallah FW, Morgan PJ, Cil T, McNaught A, Escallon JM, Semple JL, et al. Ultrasound-guided multilevel paravertebral blocks and total intravenous anesthesia improve the quality of recovery after ambulatory breast tumor resection. Anesthesiology 2014;120:703-713. [PubMed] [Free full text] doi: 10.1097/ALN.0000436117.52143.bc.
- Schnobel A, Reichl SU, Kranke P, Pogatzki-Zahn EM, Zahn PK. Efficacy and safety of paravertebral blocks in breast surgery: a meta-analysis of randomized controlled trials. Br J Anaesth 2010;105:842-852.[PubMed][Free full text] doi: 10.1093/bja/aeq265. Epub 2010 Oct 14.
- Das S, Bhattacharya P, Mandal MC, Mukhopadhyay S, Basu SR, Mandol BK. Multiple-injection thoracic paravertebral block as an alternative to general anaesthesia for elective breast surgeries: A randomized controlled trial. Indian J Anaesth 2012;56:27-33.[PubMed] [Free full text] doi: 10.4103/0019-5049.93340.
- Buckenmaier CC, Kwon KH, Howard RS, McKnight GM, Shiver CD, Fritz WT, et al. Double-blinded, placebo-controlled, prospective randomized trial evaluating the efficacy of paravertebral block with and without continuous paravertebral block analgesia in outpatient breast cancer surgery. Pain Med 2010;11:790-799.
- Arunakul P, Ruksa A. General anesthesia with thoracic paravertebral block for modified radical mastectomy. J Med Assoc Thai 2010;93:S149-S153.
- Moller JF, Nikolajsen L, Rodt SA, Ronning H, Carlsson PS. Thoracic paravertebral block for breast cancer surgery: A randomized double-blind study. Anesth Analg 2007;105:1848-1851. [PubMed] [Free full text]
- Boughey JC, Goravanchi F, Parris RN, Kee SS, Kowalski AM, Frenzel JC, et al. Prospective randomized trial of paravertebral block for patients undergoing breast cancer surgery. Am J Surg 2009;198:720-725.[PubMed] [Free full text] doi: 10.1016/j.amjsurg.2008.11.043.
- Goravanchi F, Kee SS, Kowalski AM, Berger JS, French KE. A case series of thoracic paravertebral blocks using a combination of ropivacaine, clonidine, epinephrine, and dexamethasone. J Clin Anesth 2012;24:664-667.
- Tahiri Y, Tran DeQH, Bouteaud J, Xu L, Lalonde D, Luc M, et al. General anaesthesia versus thoracic paravertebral block for breast surgery: A meta-analysis. J Plast Reconstr Aesthet Surg 2011;64:1261-1269.[PubMed] [Free full text] doi: 10.1016/j.bjps.2011.03.025. Epub 2011 Apr 12.
- Boughey JC, Goravanchi F, Parris RN, Kee SS, Frenzel JC, Hunt KK, et al. Improved postoperative pain control using thoracic paravertebral block for breast operations. Breast J 2009; 15: 483-488. [PubMed] [Free full text] doi: 10.1111/j.1524-4741.2009.00763.x. Epub 2009 Jul 13.
- Agarwal RR, Wallace AM, Madison SJ, Morgan AC, Mascha EJ, Ilfeld BM. Single-injection thoracic paravertebral block and postoperative analgesia after mastectomy: a retrospective cohort study. J Clin Anesth 2015;27:371-374.[PubMed] [Free full text] doi: 10.1016/j.jclinane.2015.04.003. Epub 2015 May 6.
- Klein SM, Bergh A, Steele SM, Georgiade GS, Greengrass RA. Thoracic paravertebral block for breast surgery. Anesth Analg 2000;90:1402-1405.[PubMed] [Free full text]
- Coopey SB, Specht MC, Warren L, Smith BL, Winograd JM, Fleischmann K. Use of prospective paravertebral block decreases length of stay in patients undergoing mastectomy plus immediate reconstruction. Ann Surg Oncol 2013;20:1282-1286.[PubMed] [Free full text] doi: 10.1245/s10434-012-2678-7. Epub 2012 Oct 14.
- Kairaluoma PM, Bachmann MS, Rosenberg PH, Pere PJ. Preincisional paravertebral block reduces the prevalence of chronic pain after breast surgery. Anesth Analg 2006;103:703-708. [PubMed] [Free full text]
- Exadaktylos AK, Buggy DJ, Moriarty DC, Mascha E, Sessler DI. Can anesthetic technique for primary breast cancer surgery affect recurrence or metastasis? Anesthesiology 2006;105:660-664.[PubMed] [Free full text]