Dora Hamad AlHarkan *
Author’s Affiliation:
* Dora Hamad AlHarkan, MD, Associate Professor, Department of Ophthalmology, College of Medicine, Qassim University, Qassim, Saudi Arabia: Email: dhhrkan@qu.edu.sa
Correspondence: Dr. Dora Hamad AlHarkan, Email: dhhrkan@qu.edu.sa; Phone: 00966554882552.
Background & objective: Strabismus is a misalignment of the eyes which can affect one or both eyes. It usually starts in early childhood, and it impacts on vision-related quality of life. Various factors have been described as to be leading to the development of strabismus in early childhood. The aim of this study was to present the rate and determinants of strabismus in children less than 12 years of age, attending our pediatric ophthalmology clinic of a hospital in central Saudi Arabia.
Methodology: It was a clinical-based prospective cross-sectional study of strabismus cases presented to a pediatric ophthalmology clinic in 2021. The incidence, demographic profile, indications for presentation, types of strabismus, angle, risk factors, association with refractive errors, amblyopia, and anisometropia, were reviewed. Descrtiptive statistics were used to present the study findings.
Results: Of the 300 children presenting to the pediatric ophthalmology unit, 154 (51.3%) were diagnosed with strabismus. Most of them (134; 87%) attended for vision impairment and cosmetic correction. Only 57 (37%) had been seen by the qualified ophthalmologists in the past. Esotropia (97; 63%) and Exotropia (40; 35.1%) were the main types of strabismus. Amblyopia was found in 25 (16.2%) children but was not significantly associated with esotropia or exotropia. (P = 0.6). The proposed mode of management included spectacles (70; 52.2%), patching (8; 6.0%), Botulin toxin injection (5; 3.7%), surgery (3; 2.2%), and monitoring strabismus angle (27; 17.9%).
Conclusions: Esotropia was the most common type of strabismus. The high incidence of amblyopia and the fact that many were not seen before by qualified ophthalmologists suggested an urgent need for a system for screening children for vision and strabismus and a referral protocol from secondary to tertiary care units in the study area.
Abbreviations: UCVA: uncorrected visual acuity, PVA: presented visual acuity,
Keywords: Childhood Blindness; cycloplegic refraction; refractive error; strabismus; visual impairment
Citation: AlHarkan DH. The magnitude and determinants of strabismus, among children under twelve years old, at a pediatric ophthalmology unit of a tertiary hospital in central Saudi Arabia. Anaesth. pain intensive care 2025;29(4):371-77. DOI: 10.35975/apic.v29i4.2822
Received: April 10, 2025; Revised: May 09, 2025; Accepted: May 09, 2025
Strabismus is a misalignment of the eyes which can affect one or both eyes. It usually starts in early childhood, and its impact on vision-related quality of life, overall development, and personality continues into adulthood. Early detection and treatment of strabismus in childhood has high success in alignment and gaining binocularity.1-3
Eye complications and hospitalization showed significant increase across different age groups during the past two decades.4-6 The prevalence of strabismus in Australian children from 2010 to 2018 was 2.6%.7 The prevalence of strabismus in children in the United Kingdom (UK) was reported to be 2.1%.8 A large proportion of manifest horizontal strabismus is of esotropia type, and the second most common is exotropia, which is mainly of intermittent type.9 Very few cases are of hypertropia type and associated with syndromes like Brown syndrome and Duane retraction syndrome.10
The importance of addressing strabismus was highlighted by developing the specialty of pediatric ophthalmology and strabismus subspecialty training in Saudi Arabia.11 In the absence of national vision and eye screening in Saudi Arabia and the lack of information on the community-based prevalence of strabismus, hospital-based information is useful for public health planning to address childhood blindness. In one such attempt, a previous study was carried out in Jeddah city of Saudi Arabia.12 In this study, the prevalence of strabismus in children attending an eye clinic with symptoms was 11.6%. The psychological negative impact of strabismus in their wards was as high as 36.2 out of 60 points in Qassim, the study area. As many as 63% of parents of children with strabismus expressed a moderate level of psychological impact.13
In the study area of Qassim province of Saudi Arabia, the estimated population of children < 15 years of age is 310,700.14 The pediatric ophthalmology unit is manned by a pediatric ophthalmologist with a clinical setup for comprehensive strabismus assessment since 2015. Surgical care was not yet part of the pediatric ophthalmology care in the Qassim region during the study period. A pilot preschool vision screening of 222 children in the kindergarten of Qassim region noted that 4.2% of children had strabismus.15 In this study, the magnitude and profile of children aged ≤ 12 years and attending a pediatric ophthalmology clinic of a tertiary hospital in 2021 was presented.
This was a clinical-based prospective cross-sectional study for consecutive children aged twelve years or less attending the pediatric ophthalmology clinic at Qassim University, Qassim region, Saudi Arabia, from January 2021 to December 2021, with a provisional diagnosis of strabismus. The pediatric ophthalmology team included a pediatric ophthalmologist, an optometrist, a nurse experienced in ophthalmic assessment, and a counselor.
The demographic profile of each patient included age at presentation, gender, and nationality. While obtaining a history of strabismus and related risk factors, parents were asked for information related to “TOFFEES” that included time of onset, Onset of strabismus – (acute or gradual), frequency of deviation-constant or intermittent, eye dominance-unilateral or alternating, progression/diurnal variation of strabismus or relation of strabismus to any gaze, presence of diplopia, head posture, developmental, systemic, or neurological issues, family history and birth history, treatment history, spectacle use and its effect on deviation and trauma (eye, face or head).16 The presence of accommodative spasm and the extent of near work were inquired.
The visual acuity uncorrected (UCVA) and presented (PVA) were checked using the Snellen chart with optotype E. If the child was not cooperative or of preverbal age, a fix and follow test was done using a LANG fixation cube. Amblyopia was defined as a difference of at least two lines on Snellen’s chart using the best corrected visual acuity between two eyes.
Ocular alignment by Hirschberg test, cover-uncover test, alternate cover test, or alternate prism cover test and evaluation in the nine cardinal gaze positions were tested. The anterior segment was examined using a slit lamp bio-microscope (Topcon, USA). The pupils were dilated using cyclopentolate 1% and phenylephrine 2.5% eyedrops. The posterior segment was evaluated using a 20-Diopter Volk lens and binocular indirect ophthalmoscope (Welch Allyn Retinoscope, US). The same ophthalmologist conducted cycloplegic refraction. The refractive status of each eye, spherical and cylindrical values, and the axis of astigmatism, as mentioned on the display of the spot screener, were noted. The spherical equivalent of each eye's refractive error was calculated using a formula of [spherical value + (cylindrical value/2)].
2.1. Sample size calculation
To calculate the sample size for the present study assuming that the prevalence of strabismus among 5000 children attending our pediatric ophthalmology clinics would be 56%, as it was reported by Agaje et al.15 To achieve a 95% confidence interval and an acceptable error margin of 6% with a clustering effect of 1.2, the required sample of children to be included in the assessment would be at least 300. OpenEpi software was used to calculate the sample size for a cross-sectional study.17
2.2. Ethical approval
The Institute Research Board of Qassim University approved this research (19-05-05). Since this was a part of the routine examination in the clinic, written informed consent was waived off. However, tenets of the Helsinki Declaration were strictly abided.
2.3. Statistical analysis
The data was collected on Microsoft XL for Mac (16.16.11). After cleaning the data and checking the consistency, the data was transferred into a spreadsheet of the Statistical Package for Social Studies (SPSS 24) (IBM, NY, USA). Univariate analysis using the parametric method was used to estimate frequencies and percentages for qualitative variables. The continuous variable not distributed normally was presented as median, interquartile range (IQR), and range.
Of the 300 consecutive children who attended the clinic during the study period, 17 had pseudostrabismus. 154 (51.3%) were with strabismus. For analysis and review profiles at presentation in this cohort, 154 children with strabismus were included. Of them, 114 (74%) were less than eight years old, 65 (42.2%) were boys, and 149 (96.8%) were Saudi nationals. Strabismus was in the left eye of 132 (85.7%) children and the right eye of 19 (12.3%) children. In 3 (1.9%) children, strabismus was in alternate eyes. Family history of strabismus was present in 7 (4.5%) and a history of premature birth was in 2 (1.3%) children. At presentation, 58 (37.7%) children were using spectacles. As many as 96 (62.3%) were seen by an ophthalmologist for the first time at the clinic. Presented vision in the worse eye was 20/20 to 20/60 in 84 (54.5%), <20/60 to 20/200 in 10 (6.5%) and <20/400 in 29 (18.8%) children. In 31 (20.1%) children, vision could not be evaluated. At presentation, 58 (37.7%) children were using spectacles. The dry and cycloplegic refraction in the right and left eyes of children with strabismus assessed at the pediatric ophthalmology clinic are given in Table 1.
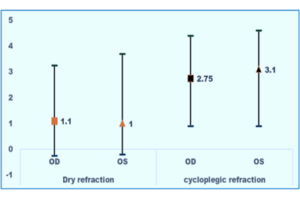
Figure 1: Comparison of dry and cycloplegic refraction in right and left eyes of children with strabismus;
X axis denotes eyes and the type of refraction performed in eyes with strabismus
Y-axis denotes the value in dioptre
OD: Oculus dexter; OS: Oculus sinister
Denote the median value of dry refraction (dioptre) in the right and left eyes
Denote the median value of cycloplegic refraction (dioptre) in the right and left eyes
The lower and upper ends of the high-low bar are the 25% and 75% values.
The median and interquartile range of dry and cycloplegic refraction in the right and left eye of = -8.0, P <0.001). The cycloplegic refraction was higher than dry refraction in the left eyes of children with strabismus. (Wilcoxon Z = -7.4, P <0.001).
Based on the underlying causes of strabismus, the children were grouped (Figure 2).
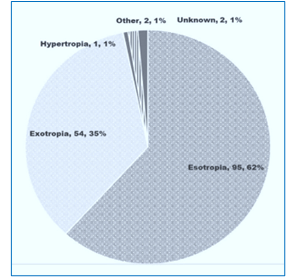
Figure 2: Types of strabismus in children
Nearly two-thirds of children had esotropia, and 35% had exotropia. Of the 154 children with strabismus, 100 (64.9%) had hyperopia, 19 (12.3%) had myopia, 15 (9.7%) had astigmatism, and 20 (13%) were emmetropic. The median angle of deviation in eyes with eso deviation for near-point fixation without refractive correction was 25ΔD (IQR 20.0; 35.4), and with correction of refractive error, it was 14.0 ΔD (IQR 6.0; 20.0). Among those with exodeviation, the median angle of deviation was -30.0 ΔD (IQR -35.0; -14.0) without correction of refractive error and 20.0 ΔD (IQR -29.0; -4.0).
Amblyopia was found in 25 (16.2%) of children with strabismus. Strabismic amblyopia was in 19 children, deprivation amblyopia in five children, and anisometropic strabismus in one child. Six children had a 2-line difference in visual acuity, three had a 3-line difference, two had a 4-line difference, two had a 5-line difference, and six had more than a 5-line difference. Patching was carried out in the past in 12 children to manage amblyopia. Of the 100 children with strabismus who needed refractive correction for managing strabismus, 58 were using spectacles. The mode of management by the pediatric ophthalmologist and team carried out in the unit is given in Table 2.
There could be 22 (14.3%) of the examined children who underwent invasive management (surgery and or BTX injections. Among children <8 years of age, esodeviation and exodeviation were noted in 77 (67.5%) and 34 (32.5%) children. Of the 8 to 12 years old, esodeviation and exodeviation were in 18 (45%) and 20 (50%) children. The risk of esodeviation was higher than exodeviation in <8 years old children but not statistically significant [relative risk (RR) = 1.3 (95% CI 0.8; 1.97), P = 0.24]. The deviation between eso and exo in boys was 43 and 19 boys and 52 and 35 girls. The risk of esodeviation was higher than exodeviation in boys than in girls but not statistically significant [RR = 1.28 (95% CI 0.84; 2.0), P = 0.24].
Based on cycloplegic spherical equivalent refraction in the worse eye, the child was grouped myopic, hyperopic, and emmetropic. The type of deviation was compared to the kind of refractive status (Figure: 3). The esodeviation and exo-deviation were more prevalent in hyperopia but were not significantly associated with the type of refractive error. (P = 0.78)
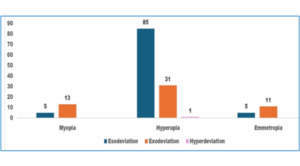
Figure 3: Cycloplegic refraction based on the refractive status of the child and type of strabismus. X-axis shows three types of refractive status of children
Y-axis shows the % of children; Blue bar shows % of children with esodeviation
Orange bar shows % of children with exodeviation; And pink bar shows % of children with vertical deviation in child.
Globally, eye complications and hospitalization showed significant figures during the past two decades.4-6 Nearly half of the children attending the pediatric ophthalmology clinic had strabismus. Six out of ten children with strabismus visited an ophthalmologist for the first time. Nearly two-thirds of children had esotropia. Three in ten children had myopia. The pediatric ophthalmology team could provide refractive services and medical management of strabismus, but 6% of cases were referred to hospitals with facilities for procedures and surgeries under general anesthesia.
This unique study highlights the profile of strabismus in children of the Qassim region evaluated by pediatric ophthalmology clinic team members during the initial period of its services. In the absence of a surgical facility in the same institution, strabismus, to a large extent, could be managed by providing refractive, orthoptic services and monitoring the impact of management. High rate of strabismus among those attending the clinic, universal vision and eye screening of preschoolers and school children, and referral from secondary to pediatric ophthalmology unit are urgently needed.
Among < 12-year-old children at the pediatric ophthalmology clinic, the strabismus rate was 44.5% in our study. This was less than 56.7% noted in <15 years old children attending an eye department of a university hospital in Ethiopia.15 The strabismus rate was as low as 6.2% among 6 to 15-year-old children in a university hospital in Pakistan.18 In Nigeria, in a university hospital, Musa et al. (2017) noted a strabismus rate of 9.1% among less than 16-year-old children.19 In the eastern province of Saudi Arabia, 1,350 children aged 1-15 years attending a private hospital had strabismus.20 In Hail City of Saudi Arabia, Anwar et al. (2018) reported a 17.1% rate of strabismus among 6 months to 19 years old children as reported by parents in interviews.21 In Arar city of Northern Saudi Arabia, the strabismus rate was 14.7% among 156 children and adolescents.22 The rate in Saudi Arabia seems to be higher. However, one should note the age group of participants and the method of collecting information while comparing the rates reported in different studies.
The proportion of esotropia and exotropia in our study was 63:30. Very few children had vertical deviation-related problems and were mainly associated with Browns syndrome and Duane retraction syndrome. Azam et al noted esotropia in 46% and exotropia in 29% of children.23 Singh et al while reviewing concomitant strabismus in 4 -19 years old children found that esotropia and exotropia proportion was 42.1% and 49% respectively.24 Contrasting to the findings of our study, a study by Wan et al focusing on children scheduled for strabismus surgery, the proportion of exotropia (63.5%) compared to esotropia (13.2%).25 This difference could be because most esotropia cases are managed by optical correction and orthoptic intervention. Exotropia is mainly managed by botulin injection and muscle surgery.26
No significant differences in horizontal strabismus by gender was identified, as noted by Laughten et al.27 This indirectly suggests gender equity in access to pediatric eye care services in the study area. In our study, the rate of esodeviation in young children compared to older school children was not significantly different from the exodeviation. Han et al., in a large cohort of Korean children, also noted identical rates of eso and exodeviation in 6 to 8 and 8 to 12-year-old children.28 Young children with esodeviation respond well to correction of hyperopia, and the chances of correcting amblyopia and achieving binocular vision are higher. This suggests universal vision and eye screening of children at younger ages.
Although esodeviation was the primary type of strabismus in the present study, it was statistically insignificant in children with hyperopia compared to myopia. A small number of myopia subgroups in children could have resulted in this observation. In reality, hyperopic children develop eso deviation as they accommodate markedly when performing near work. The PPP, therefore, includes correction of refractive error both for eso and exodeviation.26
Children with esodeviation had an interquartile range of 20 ΔD to 35ΔD of strabismus for near fixation without refraction correction. This matched another study in a tertiary eye hospital in central Saudi Arabia.29 The majority can be treated with refractive correction and patching.
In our study, half of children with strabismus presented to an ophthalmologist for the first time. This reflects a lack of universal vision and eye screening in the study area and referral protocol for sending children from primary eye care to secondary and tertiary eye care units. To avoid cold cases of trivial eye problems in children, the pediatric ophthalmology unit and adequate time for comprehensive assessment and management of sight-threatening conditions in children.
In our study, the proportion of male and female children with strabismus was 42.2:57.8. This matched the gender ratio of 55:45 in a study in India by Singh et al.24 This ratio, however, was 74:26 in a study at Arar, Saudi Arabia.22 Three-fourths of children with strabismus who attended a pediatric ophthalmology clinic were less than eight years of age. This is a promising observation. An early intervention causes a positive and sustained impact in treating strabismus and amblyopia.30
The coverage of refractive services could provide spectacles in only 58% of children with strabismus at the time of presentation. Vision screening through child health care and school health is a recommended strategy by the World Health Organization and should be urgently applied in the study area.31
The proposed mode of management for children with strabismus in our study shows that medical therapy, with proper power of glasses prescription and patching for treating amblyopia, is the most common way of managing strabismus cases. Strabismus management in children needs periodic evaluation and adjustment of treatment modalities. The role of pediatricians, general ophthalmologists, and primary health care units in the study area is crucial for follow-ups of such children by pediatric ophthalmology units.
There were a few limitations to the study. The hospital was newly established during the study period without a surgical facility. Therefore, many children with visual impairment and strabismus might have been sent directly to the tertiary eye hospital in the capital, Riyadh, where interventional procedures have been performed for the previous two decades. Therefore, hospital-based information from the present study may be underestimated and not true representative of issues in the community.
The cross-sectional study design restricted the ability to examine the causality across the study variables. Besides, this is a single center study; which restricts the generazability of the study findings. Future multi-center studies that involve follow-up are warranted to enhance the generazability of the study findings.
The high incidence of strabismus noted at the tertiary eye clinic of Qassim is a matter of great concern. Early detection through a regional vision and eye screening program of preschool and school children is urgently needed for early detection of strabismus and amblyogenic factors. Establishing a primary eye care and referral system from secondary to pediatric ophthalmology units will bring these cases to experts at a center with the required team and tools. Most of the cases could be managed with glasses and eye patching and only few needed surgical intervention. In absence of community based information on strabismus and risk factors, information from hospital-based data, although inferior for better planning, could be pointers for weak areas and strengthen the strategies that are internationally recommended and practiced.
7. Data availability
The numerical data generated during this research is available with the authors.
8. Conflict of interest
All authors declare that there was no conflict of interest.
9. Funding
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Authors’ contribution
Dora Hamad AlHarkan has been the sole author of this paper.
Author’s Affiliation:
* Dora Hamad AlHarkan, MD, Associate Professor, Department of Ophthalmology, College of Medicine, Qassim University, Qassim, Saudi Arabia: Email: dhhrkan@qu.edu.sa
Correspondence: Dr. Dora Hamad AlHarkan, Email: dhhrkan@qu.edu.sa; Phone: 00966554882552.
ABSTRACT
Background & objective: Strabismus is a misalignment of the eyes which can affect one or both eyes. It usually starts in early childhood, and it impacts on vision-related quality of life. Various factors have been described as to be leading to the development of strabismus in early childhood. The aim of this study was to present the rate and determinants of strabismus in children less than 12 years of age, attending our pediatric ophthalmology clinic of a hospital in central Saudi Arabia.
Methodology: It was a clinical-based prospective cross-sectional study of strabismus cases presented to a pediatric ophthalmology clinic in 2021. The incidence, demographic profile, indications for presentation, types of strabismus, angle, risk factors, association with refractive errors, amblyopia, and anisometropia, were reviewed. Descrtiptive statistics were used to present the study findings.
Results: Of the 300 children presenting to the pediatric ophthalmology unit, 154 (51.3%) were diagnosed with strabismus. Most of them (134; 87%) attended for vision impairment and cosmetic correction. Only 57 (37%) had been seen by the qualified ophthalmologists in the past. Esotropia (97; 63%) and Exotropia (40; 35.1%) were the main types of strabismus. Amblyopia was found in 25 (16.2%) children but was not significantly associated with esotropia or exotropia. (P = 0.6). The proposed mode of management included spectacles (70; 52.2%), patching (8; 6.0%), Botulin toxin injection (5; 3.7%), surgery (3; 2.2%), and monitoring strabismus angle (27; 17.9%).
Conclusions: Esotropia was the most common type of strabismus. The high incidence of amblyopia and the fact that many were not seen before by qualified ophthalmologists suggested an urgent need for a system for screening children for vision and strabismus and a referral protocol from secondary to tertiary care units in the study area.
Abbreviations: UCVA: uncorrected visual acuity, PVA: presented visual acuity,
Keywords: Childhood Blindness; cycloplegic refraction; refractive error; strabismus; visual impairment
Citation: AlHarkan DH. The magnitude and determinants of strabismus, among children under twelve years old, at a pediatric ophthalmology unit of a tertiary hospital in central Saudi Arabia. Anaesth. pain intensive care 2025;29(4):371-77. DOI: 10.35975/apic.v29i4.2822
Received: April 10, 2025; Revised: May 09, 2025; Accepted: May 09, 2025
1. INTRODUCTION
Strabismus is a misalignment of the eyes which can affect one or both eyes. It usually starts in early childhood, and its impact on vision-related quality of life, overall development, and personality continues into adulthood. Early detection and treatment of strabismus in childhood has high success in alignment and gaining binocularity.1-3
Eye complications and hospitalization showed significant increase across different age groups during the past two decades.4-6 The prevalence of strabismus in Australian children from 2010 to 2018 was 2.6%.7 The prevalence of strabismus in children in the United Kingdom (UK) was reported to be 2.1%.8 A large proportion of manifest horizontal strabismus is of esotropia type, and the second most common is exotropia, which is mainly of intermittent type.9 Very few cases are of hypertropia type and associated with syndromes like Brown syndrome and Duane retraction syndrome.10
The importance of addressing strabismus was highlighted by developing the specialty of pediatric ophthalmology and strabismus subspecialty training in Saudi Arabia.11 In the absence of national vision and eye screening in Saudi Arabia and the lack of information on the community-based prevalence of strabismus, hospital-based information is useful for public health planning to address childhood blindness. In one such attempt, a previous study was carried out in Jeddah city of Saudi Arabia.12 In this study, the prevalence of strabismus in children attending an eye clinic with symptoms was 11.6%. The psychological negative impact of strabismus in their wards was as high as 36.2 out of 60 points in Qassim, the study area. As many as 63% of parents of children with strabismus expressed a moderate level of psychological impact.13
In the study area of Qassim province of Saudi Arabia, the estimated population of children < 15 years of age is 310,700.14 The pediatric ophthalmology unit is manned by a pediatric ophthalmologist with a clinical setup for comprehensive strabismus assessment since 2015. Surgical care was not yet part of the pediatric ophthalmology care in the Qassim region during the study period. A pilot preschool vision screening of 222 children in the kindergarten of Qassim region noted that 4.2% of children had strabismus.15 In this study, the magnitude and profile of children aged ≤ 12 years and attending a pediatric ophthalmology clinic of a tertiary hospital in 2021 was presented.
2. METHODOLOGY
This was a clinical-based prospective cross-sectional study for consecutive children aged twelve years or less attending the pediatric ophthalmology clinic at Qassim University, Qassim region, Saudi Arabia, from January 2021 to December 2021, with a provisional diagnosis of strabismus. The pediatric ophthalmology team included a pediatric ophthalmologist, an optometrist, a nurse experienced in ophthalmic assessment, and a counselor.
The demographic profile of each patient included age at presentation, gender, and nationality. While obtaining a history of strabismus and related risk factors, parents were asked for information related to “TOFFEES” that included time of onset, Onset of strabismus – (acute or gradual), frequency of deviation-constant or intermittent, eye dominance-unilateral or alternating, progression/diurnal variation of strabismus or relation of strabismus to any gaze, presence of diplopia, head posture, developmental, systemic, or neurological issues, family history and birth history, treatment history, spectacle use and its effect on deviation and trauma (eye, face or head).16 The presence of accommodative spasm and the extent of near work were inquired.
The visual acuity uncorrected (UCVA) and presented (PVA) were checked using the Snellen chart with optotype E. If the child was not cooperative or of preverbal age, a fix and follow test was done using a LANG fixation cube. Amblyopia was defined as a difference of at least two lines on Snellen’s chart using the best corrected visual acuity between two eyes.
Ocular alignment by Hirschberg test, cover-uncover test, alternate cover test, or alternate prism cover test and evaluation in the nine cardinal gaze positions were tested. The anterior segment was examined using a slit lamp bio-microscope (Topcon, USA). The pupils were dilated using cyclopentolate 1% and phenylephrine 2.5% eyedrops. The posterior segment was evaluated using a 20-Diopter Volk lens and binocular indirect ophthalmoscope (Welch Allyn Retinoscope, US). The same ophthalmologist conducted cycloplegic refraction. The refractive status of each eye, spherical and cylindrical values, and the axis of astigmatism, as mentioned on the display of the spot screener, were noted. The spherical equivalent of each eye's refractive error was calculated using a formula of [spherical value + (cylindrical value/2)].
2.1. Sample size calculation
To calculate the sample size for the present study assuming that the prevalence of strabismus among 5000 children attending our pediatric ophthalmology clinics would be 56%, as it was reported by Agaje et al.15 To achieve a 95% confidence interval and an acceptable error margin of 6% with a clustering effect of 1.2, the required sample of children to be included in the assessment would be at least 300. OpenEpi software was used to calculate the sample size for a cross-sectional study.17
2.2. Ethical approval
The Institute Research Board of Qassim University approved this research (19-05-05). Since this was a part of the routine examination in the clinic, written informed consent was waived off. However, tenets of the Helsinki Declaration were strictly abided.
2.3. Statistical analysis
The data was collected on Microsoft XL for Mac (16.16.11). After cleaning the data and checking the consistency, the data was transferred into a spreadsheet of the Statistical Package for Social Studies (SPSS 24) (IBM, NY, USA). Univariate analysis using the parametric method was used to estimate frequencies and percentages for qualitative variables. The continuous variable not distributed normally was presented as median, interquartile range (IQR), and range.
3. RESULTS
Of the 300 consecutive children who attended the clinic during the study period, 17 had pseudostrabismus. 154 (51.3%) were with strabismus. For analysis and review profiles at presentation in this cohort, 154 children with strabismus were included. Of them, 114 (74%) were less than eight years old, 65 (42.2%) were boys, and 149 (96.8%) were Saudi nationals. Strabismus was in the left eye of 132 (85.7%) children and the right eye of 19 (12.3%) children. In 3 (1.9%) children, strabismus was in alternate eyes. Family history of strabismus was present in 7 (4.5%) and a history of premature birth was in 2 (1.3%) children. At presentation, 58 (37.7%) children were using spectacles. As many as 96 (62.3%) were seen by an ophthalmologist for the first time at the clinic. Presented vision in the worse eye was 20/20 to 20/60 in 84 (54.5%), <20/60 to 20/200 in 10 (6.5%) and <20/400 in 29 (18.8%) children. In 31 (20.1%) children, vision could not be evaluated. At presentation, 58 (37.7%) children were using spectacles. The dry and cycloplegic refraction in the right and left eyes of children with strabismus assessed at the pediatric ophthalmology clinic are given in Table 1.
| Table 1: Refractive status of children with strabismus at pediatric ophthalmology clinic | |||
| Refractive indices | Dry refraction | with cycloplegia | |
| Spherical OD (D) | Number Median (Min−Max) IQR |
105 0.5 (-8.0−6.25) -0.87; 2.1 |
153 2.0 (-10− 8.0) 0.25; 3.75 |
| Spherical OS (D) | Number Median (Min− Max) IQR |
104 0.5 (-10.0−6.5) -0.75; 3.0 |
154 2.0 (-11.0− 8.0) 0.44; 4.0 |
| Cylinder OD (D) | Number Median (Min− Max) IQR |
103 1.0 (-0.5−6.5) 0.5; 2.0 |
134 1.0 (-2.5−6.0) 0.5; 1.8 |
| Cylinder OS (D) | Number Median (Min− Max) IQR |
97 1.25 (-0.25−6.5) 0.75; 2.0 |
134 1.2 (-2.5−20) 0.7; 1.75 |
| Spherical equivalent OD | Number Median (Min− Max) IQR |
103 1.1 (-7.5−6.75) -0.25; 3.25 |
134 2.75 (-5.6−8.2) 0.9; 4.4 |
| Spherical equivalent OS | Number Median (Min− Max) IQR |
97 1.0 (-8.8−7.6) -0.19; 3.7 |
134 3.1 (-6.6−14.5) 0.9; 4.6 |
| IQR: Interquartile range; OD: Oculus dexter; OS: Oculus sinister | |||
Figure 1: Comparison of dry and cycloplegic refraction in right and left eyes of children with strabismus;
X axis denotes eyes and the type of refraction performed in eyes with strabismus
Y-axis denotes the value in dioptre
OD: Oculus dexter; OS: Oculus sinister
Denote the median value of dry refraction (dioptre) in the right and left eyes
Denote the median value of cycloplegic refraction (dioptre) in the right and left eyes
The lower and upper ends of the high-low bar are the 25% and 75% values.
The median and interquartile range of dry and cycloplegic refraction in the right and left eye of = -8.0, P <0.001). The cycloplegic refraction was higher than dry refraction in the left eyes of children with strabismus. (Wilcoxon Z = -7.4, P <0.001).
Based on the underlying causes of strabismus, the children were grouped (Figure 2).
Figure 2: Types of strabismus in children
Nearly two-thirds of children had esotropia, and 35% had exotropia. Of the 154 children with strabismus, 100 (64.9%) had hyperopia, 19 (12.3%) had myopia, 15 (9.7%) had astigmatism, and 20 (13%) were emmetropic. The median angle of deviation in eyes with eso deviation for near-point fixation without refractive correction was 25ΔD (IQR 20.0; 35.4), and with correction of refractive error, it was 14.0 ΔD (IQR 6.0; 20.0). Among those with exodeviation, the median angle of deviation was -30.0 ΔD (IQR -35.0; -14.0) without correction of refractive error and 20.0 ΔD (IQR -29.0; -4.0).
Amblyopia was found in 25 (16.2%) of children with strabismus. Strabismic amblyopia was in 19 children, deprivation amblyopia in five children, and anisometropic strabismus in one child. Six children had a 2-line difference in visual acuity, three had a 3-line difference, two had a 4-line difference, two had a 5-line difference, and six had more than a 5-line difference. Patching was carried out in the past in 12 children to manage amblyopia. Of the 100 children with strabismus who needed refractive correction for managing strabismus, 58 were using spectacles. The mode of management by the pediatric ophthalmologist and team carried out in the unit is given in Table 2.
| Table: 2 Management of children with strabismus by pediatric ophthalmologist | |
| Management strategy | Number (%) |
| Spectacles | 90 (58.4) |
| Patching | 11 (7.1) |
| Butulin A injection | 8 (5.2) |
| Extraocular muscle surgery | 2 (1.3) |
| Follow to monitor changes in strabismus angle | 11 (7.1) |
| Other ocular surgeries | 2 (1.3) |
| Other investigation and management | 10 (6.5) |
| Total | 154 (100) |
There could be 22 (14.3%) of the examined children who underwent invasive management (surgery and or BTX injections. Among children <8 years of age, esodeviation and exodeviation were noted in 77 (67.5%) and 34 (32.5%) children. Of the 8 to 12 years old, esodeviation and exodeviation were in 18 (45%) and 20 (50%) children. The risk of esodeviation was higher than exodeviation in <8 years old children but not statistically significant [relative risk (RR) = 1.3 (95% CI 0.8; 1.97), P = 0.24]. The deviation between eso and exo in boys was 43 and 19 boys and 52 and 35 girls. The risk of esodeviation was higher than exodeviation in boys than in girls but not statistically significant [RR = 1.28 (95% CI 0.84; 2.0), P = 0.24].
Based on cycloplegic spherical equivalent refraction in the worse eye, the child was grouped myopic, hyperopic, and emmetropic. The type of deviation was compared to the kind of refractive status (Figure: 3). The esodeviation and exo-deviation were more prevalent in hyperopia but were not significantly associated with the type of refractive error. (P = 0.78)
Figure 3: Cycloplegic refraction based on the refractive status of the child and type of strabismus. X-axis shows three types of refractive status of children
Y-axis shows the % of children; Blue bar shows % of children with esodeviation
Orange bar shows % of children with exodeviation; And pink bar shows % of children with vertical deviation in child.
4. DISCUSSION
Globally, eye complications and hospitalization showed significant figures during the past two decades.4-6 Nearly half of the children attending the pediatric ophthalmology clinic had strabismus. Six out of ten children with strabismus visited an ophthalmologist for the first time. Nearly two-thirds of children had esotropia. Three in ten children had myopia. The pediatric ophthalmology team could provide refractive services and medical management of strabismus, but 6% of cases were referred to hospitals with facilities for procedures and surgeries under general anesthesia.
This unique study highlights the profile of strabismus in children of the Qassim region evaluated by pediatric ophthalmology clinic team members during the initial period of its services. In the absence of a surgical facility in the same institution, strabismus, to a large extent, could be managed by providing refractive, orthoptic services and monitoring the impact of management. High rate of strabismus among those attending the clinic, universal vision and eye screening of preschoolers and school children, and referral from secondary to pediatric ophthalmology unit are urgently needed.
Among < 12-year-old children at the pediatric ophthalmology clinic, the strabismus rate was 44.5% in our study. This was less than 56.7% noted in <15 years old children attending an eye department of a university hospital in Ethiopia.15 The strabismus rate was as low as 6.2% among 6 to 15-year-old children in a university hospital in Pakistan.18 In Nigeria, in a university hospital, Musa et al. (2017) noted a strabismus rate of 9.1% among less than 16-year-old children.19 In the eastern province of Saudi Arabia, 1,350 children aged 1-15 years attending a private hospital had strabismus.20 In Hail City of Saudi Arabia, Anwar et al. (2018) reported a 17.1% rate of strabismus among 6 months to 19 years old children as reported by parents in interviews.21 In Arar city of Northern Saudi Arabia, the strabismus rate was 14.7% among 156 children and adolescents.22 The rate in Saudi Arabia seems to be higher. However, one should note the age group of participants and the method of collecting information while comparing the rates reported in different studies.
The proportion of esotropia and exotropia in our study was 63:30. Very few children had vertical deviation-related problems and were mainly associated with Browns syndrome and Duane retraction syndrome. Azam et al noted esotropia in 46% and exotropia in 29% of children.23 Singh et al while reviewing concomitant strabismus in 4 -19 years old children found that esotropia and exotropia proportion was 42.1% and 49% respectively.24 Contrasting to the findings of our study, a study by Wan et al focusing on children scheduled for strabismus surgery, the proportion of exotropia (63.5%) compared to esotropia (13.2%).25 This difference could be because most esotropia cases are managed by optical correction and orthoptic intervention. Exotropia is mainly managed by botulin injection and muscle surgery.26
No significant differences in horizontal strabismus by gender was identified, as noted by Laughten et al.27 This indirectly suggests gender equity in access to pediatric eye care services in the study area. In our study, the rate of esodeviation in young children compared to older school children was not significantly different from the exodeviation. Han et al., in a large cohort of Korean children, also noted identical rates of eso and exodeviation in 6 to 8 and 8 to 12-year-old children.28 Young children with esodeviation respond well to correction of hyperopia, and the chances of correcting amblyopia and achieving binocular vision are higher. This suggests universal vision and eye screening of children at younger ages.
Although esodeviation was the primary type of strabismus in the present study, it was statistically insignificant in children with hyperopia compared to myopia. A small number of myopia subgroups in children could have resulted in this observation. In reality, hyperopic children develop eso deviation as they accommodate markedly when performing near work. The PPP, therefore, includes correction of refractive error both for eso and exodeviation.26
Children with esodeviation had an interquartile range of 20 ΔD to 35ΔD of strabismus for near fixation without refraction correction. This matched another study in a tertiary eye hospital in central Saudi Arabia.29 The majority can be treated with refractive correction and patching.
In our study, half of children with strabismus presented to an ophthalmologist for the first time. This reflects a lack of universal vision and eye screening in the study area and referral protocol for sending children from primary eye care to secondary and tertiary eye care units. To avoid cold cases of trivial eye problems in children, the pediatric ophthalmology unit and adequate time for comprehensive assessment and management of sight-threatening conditions in children.
In our study, the proportion of male and female children with strabismus was 42.2:57.8. This matched the gender ratio of 55:45 in a study in India by Singh et al.24 This ratio, however, was 74:26 in a study at Arar, Saudi Arabia.22 Three-fourths of children with strabismus who attended a pediatric ophthalmology clinic were less than eight years of age. This is a promising observation. An early intervention causes a positive and sustained impact in treating strabismus and amblyopia.30
The coverage of refractive services could provide spectacles in only 58% of children with strabismus at the time of presentation. Vision screening through child health care and school health is a recommended strategy by the World Health Organization and should be urgently applied in the study area.31
The proposed mode of management for children with strabismus in our study shows that medical therapy, with proper power of glasses prescription and patching for treating amblyopia, is the most common way of managing strabismus cases. Strabismus management in children needs periodic evaluation and adjustment of treatment modalities. The role of pediatricians, general ophthalmologists, and primary health care units in the study area is crucial for follow-ups of such children by pediatric ophthalmology units.
5. LIMITATIONS
There were a few limitations to the study. The hospital was newly established during the study period without a surgical facility. Therefore, many children with visual impairment and strabismus might have been sent directly to the tertiary eye hospital in the capital, Riyadh, where interventional procedures have been performed for the previous two decades. Therefore, hospital-based information from the present study may be underestimated and not true representative of issues in the community.
The cross-sectional study design restricted the ability to examine the causality across the study variables. Besides, this is a single center study; which restricts the generazability of the study findings. Future multi-center studies that involve follow-up are warranted to enhance the generazability of the study findings.
6. CONCLUSION
The high incidence of strabismus noted at the tertiary eye clinic of Qassim is a matter of great concern. Early detection through a regional vision and eye screening program of preschool and school children is urgently needed for early detection of strabismus and amblyogenic factors. Establishing a primary eye care and referral system from secondary to pediatric ophthalmology units will bring these cases to experts at a center with the required team and tools. Most of the cases could be managed with glasses and eye patching and only few needed surgical intervention. In absence of community based information on strabismus and risk factors, information from hospital-based data, although inferior for better planning, could be pointers for weak areas and strengthen the strategies that are internationally recommended and practiced.
7. Data availability
The numerical data generated during this research is available with the authors.
8. Conflict of interest
All authors declare that there was no conflict of interest.
9. Funding
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Authors’ contribution
Dora Hamad AlHarkan has been the sole author of this paper.
11. REFERENCES
- Buffenn AN. Impact of strabismus on psychosocial health and quality of life: a systematic review. Surv Ophthalmol. 2021;66(6):1051-4. [PubMed] DOI: 1016/j.survophthal.2021.03.005
- Kraus C, Kuwera E. What is strabismus? JAMA. 2023;329(10):856. [PubMed] DOI: 1001/jama.2023.0052
- Ugli B, Nematillaevna K. Causes and treatment methods of strabismus. World Bull Public Health. 2022;17(1):45-7.
- Alrawashdeh HM, Naser AY, Alwafi H, AbuAlhommos AK, Jalal Z, Paudyal V, et al. Trends in hospital admissions for eye and adnexa diseases in England and Wales: an ecological study. Int J Gen Med. 2022;15:1097-110. [PubMed] DOI: 2147/IJGM.S344380
- Hassanin FF, Naser AY, Aalam WA, Hanbazazh M. Eye and adnexa hospitalization in Australia: an ecological study. Medicine (Baltimore). 2024;103(27):e38829. [PubMed] DOI: 1097/MD.0000000000038829
- Naqeeb MR, Naser AY. Postprocedural disorders of eye and adnexa admissions profile. Clin Optom. 2023;15:261-70. [PubMed] DOI: 2147/OPTO.S437044
- Hatt SR, Leske DA, Castañeda YS, et al. Association of strabismus with functional vision and eye-related quality of life in children. JAMA Ophthalmol. 2020;138(5):528-35. [PubMed] DOI: 1001/jamaophthalmol.2020.0539
- Christabelle FA. Development of vision and strabismus in childhood: prevalence and risk factors. Uni Technol Sydney, Australia; 2020.. Full Text
- Bommireddy T, Taylor K, Clarke MP. Assessing strabismus in children. Paediatr Child Health. 2020;30(1):14-8. DOI: 1016/j.paed.2019.10.003
- Dotan G, Jain S, Vagge A, Nelson LB. Diagnosis and management of strabismus syndromes. J Pediatr Ophthalmol Strabismus. 2022;59(4):210-2. [PubMed] DOI: 3928/01913913-20220622-01
- Khan AO, Al-Mesfer S. Pediatric ophthalmology and strabismus in Saudi Arabia. J AAPOS. 2004;8(6):513-4. [PubMed] DOI: 1016/j.jaapos.2004.05.001
- Qanat AS, Alsuheili A, Alzahrani AM, Faydhi AA, Albadri A, Alhibshi N. Types of strabismus among pediatric patients in a tertiary hospital in Jeddah. Cureus. 2020;12(12):e11978. [PubMed] DOI: 7759/cureus.11978
- Althiabi S, AlDarrab A, Alenezi SH, Alharbi BA, Aljbreen AJ, Alsalamah GF, et al. Psychosocial challenges parents of children with strabismus face in Qassim, Saudi Arabia: a cross-sectional study. Cureus. 2023;15(3):e36920. [PubMed] DOI: 7759/cureus.36920
- Ministry of Health. Primary health care centers in Qassim region. In: Statistical Book 2021. Chapter 2; 2021. Available from: https://www.moh.gov.sa/en/Ministry/Statistics/book/Documents/Statistical-Yearbook-2021.pdf
- Agaje BG, Delelegne D, Abera E, Desta K, Girum M, Mossie M, et al. Strabismus prevalence and associated factors in pediatric patients in southern Ethiopia: a cross-sectional study. J Int Med Res. 2020;48(10):300060520964339. [PubMed] DOI: 1177/0300060520964339
- Dadeya S, Kaur S. Basic examination of strabismus. 2021. Available from: https://www.researchgate.net/publication/349348910_Basic_Examination_of_Strabismus
- Dean AG, Sullivan KM, Soe MM. OpenEpi: open source epidemiologic statistics for public health. Version 2013. https://www.scienceopen.com/book?vid=61cdd360-9883-4330-8c18-3f0341b0f715
- Junejo A, Hassan M. Strabismus and its types in children aged 6–15 years at a public hospital in Karachi. J Dow Univ Health Sci. 2019;13:24-9. DOI: 36570/jduhs.2019.1.627
- Musa KO, Idowu OO, Salami MO, Olowoyeye AO. Spectrum of childhood strabismus seen at Lagos University Teaching Hospital, Lagos, Nigeria. Niger Q J Hosp Med. 2017;27(2):726-32. Full Text
- Al-Tamimi ER, Shakeel A, Yassin SA, Ali SI, Khan UA. Refractive errors, strabismus, and amblyopia in pediatric patients: a clinic-based study. J Fam Community Med. 2015;22(3):158-62. [PubMed] DOI: 4103/2230-8229.163031
- Anwar AA, Albalawi AMA, Alharbi AAH, Alanazi FHA, Alahmari HSH, Alharthi MHM, et al. Pattern of strabismus in children and adolescents in Hail, Saudi Arabia. J Health Med Nurs. 2018;54:28-33. Full Text
- Alenezi HM, Abo El-Fetoh NM, Alanaz WL, Alanazi NS, Alanazi MS, et al. Squint in children and adolescents in Arar, northern Saudi Arabia. Egypt J Hosp Med. 2018;70(2):298-302. DOI: 12816/0043093
- Fahim M. Prevalence and types of strabismus in pediatric patients aged 6–15 years in a tertiary eye hospital, Karachi. Biom Biostat Int J. 2019;8.
- Singh A, Chawla O, Verma R, Saxena V. Refractive errors and concomitant strabismus in children and adolescents: a hospital-based study. Delhi J Ophthalmol. 2022;32. DOI:7869/djo.711
- Wan X, Wan L, Jiang M, Ding Y, Wang Y, Zhang J. Strabismus surgery at a tertiary center in northern China: 2014–2019. BMC Ophthalmol. 2021;21(1):40. [PubMed] DOI: 1186/s12886-021-01805-w
- Sprunger DT, Lambert SR, Hercinovic A, et al. Esotropia and exotropia preferred practice pattern. Ophthalmology. 2023;130(3):P179-221. [PubMed] DOI: 1016/j.ophtha.2022.11.002
- Laughton SC, Hagen MM, Yang W, von Bartheld CS. Gender differences in horizontal strabismus: meta-analysis shows clinic bias toward females. J Glob Health. 2023;13:04085. [PubMed] DOI: 7189/jogh.13.04085
- Han KE, Baek SH, Kim SH, Lim KH. Strabismus prevalence and risk factors in Korean youth: KNHANES 2008–2011. PLoS One. 2018;13(2):e0191857. [PubMed] DOI: 1371/journal.pone.0191857
- AlHarkan D. Profile of children with strabismus managed non-surgically in central Saudi Arabia. Majmaah J Health Sci. 2020;8(1):1-8. DOI: 5455/mjhs.2020.01.002
- Aljohani S, Aldakhil S, Alrasheed SH, Tan QQ, Alshammeri S. Clinical characteristics of amblyopia in children under 17 in Qassim, Saudi Arabia. Clin Ophthalmol. 2022;16:2677-84. [PubMed] DOI: 2147/OPTH.S379550
- EMR-IAPB. Guidelines for school eye health in the Eastern Mediterranean Region. 2009. Full Text