Ahmed Abdalwahab 1, Mohammed Mansour 2, Yahya M. Hammad 3, Mohammed O. Ismael 4, Doaa F. Abdelfattah 5
Author affiliations:
Background & objective: The superiority of external oblique intercostal plane (EOIP) block over oblique subcostal transversus abdominis plane (OSTAP) block for intra and postoperative analgesia in laparoscopic cholecystectomy has not been established. Therefore, this study compared the efficacy of the analgesic effect between EOIP block and OSTAP block in patients undergoing laparoscopic cholecystectomy.
Methodology: This randomized controlled clinical trial was conducted on adult patients who underwent elective laparoscopic cholecystectomy from 2023 to 2024. Patients were randomly allocated into two groups at a 1:1 ratio. Group A (n = 20) included patients who received ultrasound-guided bilateral EOIP block, and Group B (n = 20) included patients who received ultrasound-guided OSTAP block.
Results: Group A had a longer time to rescue analgesia (7.05 ± 0.76 vs. 4.95 ± 0.83 min, P < 0.001), and consumed a significantly lower total dose of nalbuphine (0.1 ± 0.02 vs. 0.12 ± 0.02 mg/kg; P = 0.025). The pain score was lower in Group A, particularly at 4 and 6 hours postoperatively (P < 0.001).
Conclusions: Ultrasound-guided bilateral EOIP block provides superior analgesia than OSTAP with a longer time to rescue analgesia, lower opioid consumption, and improved early postoperative pain scores in patients undergoing laparoscopic cholecystectomy.
Abbreviations: EOIP: external oblique intercostal plane, IQR: interquartile ranges. LP: Laparoscopic cholecystectomy, OSTAP: oblique subcostal transversus abdominis plane, VAS: visual analog scale,
Keywords: external oblique intercostal plane block; laparoscopic cholecystectomy; Pain; subcostal transversus abdominis plane block; ultrasound-guided analgesia
Citation: Abdalwahab A, Mansour M, Hammad YM, Ismael MO, Abdelfattah DF. Bilateral ultrasound-guided external oblique intercostal plane block versus bilateral subcostal transversus abdominis plane block in laparoscopic cholecystectomy: a randomized controlled trial. Anaesth. pain intensive care 2025;29(4):363-70. DOI: 10.35975/apic.v29i4.2821
Received: March 02, 2025; Revised: April 20, 2025; Accepted: May 01, 2025
Laparoscopic cholecystectomy (LC) has become the standard approach for the surgical management of gallbladder stones.1-3 Postoperative pain, which can be either visceral or somatic, is still a significant clinical issue after LC. Visceral pain occurs due to gallbladder resection and carbon dioxide (CO2) irritation of the diaphragm, and somatic pain occurs from incision sites.2
Postoperative pain is a significant contributing factor to increased morbidity and mortality after LC and halts same-day discharge.3,4 Therefore, several analgesic techniques were used to ameliorate the deleterious effects of postoperative pain and improve patient outcomes.5 Ultrasound-guided transversus abdominis plane block is one of the methods used for postoperative analgesia, especially for controlling somatic pain in abdominal surgeries. In this technique, local anesthetic is injected into the fascial plane between the transversus abdominis and internal oblique muscles.6
Studies have shown that the subcostal approach for TAP (OSTAP) block could have beneficial analgesic effects on the area above the umbilicus because it blocks the area supplied by T7-12.7,8 External oblique intercostal plane block (EOIP block), in which the local anesthetic is injected in the tissue plane between the external oblique and intercostal muscles between the sixth and seventh ribs, is a modification of fascial plane blocks that target the upper lateral abdominal walls.9 We hypothesize that the external oblique intercostal plane block might be more efficient than the oblique subcostal TAP block in terms of intra- and postoperative analgesia in LC. Therefore, our study compared the efficacy of the analgesic effect between EOIP block and OSTAP block in patients undergoing LC.
We conducted a randomized clinical trial on adult patients who underwent elective LC from May 2023 to May 2024 at Cairo University Hospital, Cairo, Egypt. The study was conducted on adult patients aged between 18 and 60 years, with American Society of Anesthesiologists (ASA) classes I and II. Patients with neurological or psychological disorders, end-organ failure, bleeding abnormalities, infections at the injection sites, or allergies to amide local anesthetics were excluded.
The Research Ethics Committee of the Faculty of Medicine, Cairo University approved the research. Patients signed informed consent before participation.
The trial was registered in the Pan African Clinical Trial Registry (PACTR202406698979681).
The study was conducted per the Declaration of Helsinki.10 We reported the trial results according to the CONSORT guideline.11
According to a previous study, the total tramadol consumption in the first 24 hours after surgery was 199 ± 27.7 mg in patients receiving OSTAP who underwent LC.12 Using an opioid conversion table, this dose is equivalent to 19.9 ± 2.77 mg nalbuphine.13 A total sample of 34 was needed to detect a 5 mg difference in nalbuphine consumption, and we used a more conservative common standard deviation of 5. The sample size was calculated to achieve a study power of 80% and an alpha error of 0.05. The number of envelopes was increased to 40 (20 per group) to compensate for possible dropouts. The sample size was calculated via MedCalc Software V14.
Patients were randomly allocated via blocked randomization with a block size between 4 and 6. The randomization sequence was generated via (www.randomization.com) by the principal investigator. The randomization sequence was concealed in sealed envelopes and opened by an independent nurse. Patients were randomized into two groups at a 1:1 ratio. Group A (n = 20) included patients who received ultrasound-guided bilateral EOIP block, and Group B (n = 20) included patients who received ultrasound-guided OSTAP block. Patients were blinded to the allocated treatment.
Preoperative assessment was performed for all patients scheduled for LC, including proper medical and surgical history, chest, airway, and planned regional block examination site. All preoperative investigations were revised to assess enrollment eligibility. Patients were educated about the visual analog scale (VAS) and how to quantify pain intensity.
Intraoperatively, patients were connected to a noninvasive blood pressure monitor, electrocardiogram, and pulse oximeter, and baseline readings were recorded prior to induction of anesthesia, five minutes after endotracheal intubation, five minutes after the sensory block, before the skin incision, and then every 10 minutes. Induction and maintenance of anesthesia followed the same protocol in both groups.
All patients received 1 gm of paracetamol and 30 mg of ketorolac IV for control of visceral pain. A dose of 0.5 µg/kg fentanyl was given as rescue analgesia at any time of the surgery if needed in the case of increased mean arterial blood pressure (MAP) and heart rate by 30% or more above the baseline reading, despite adequate ventilation, hypnosis, muscle relaxation, and hydration.
2.1. External oblique intercostal plane block
The patients were placed supine, and the skin was prepared. The ultrasound transducer was placed between the anterior axillary and midclavicular lines at the level of the 6th rib. The anesthesiologist injected 20 ml of 0.25% bupivacaine bilaterally into the external oblique intercostal plane via a 22G, 80 mm block needle (Figure 1).
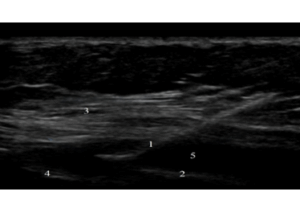
Figure 1: Ultrasound image of external oblique intercostal plane block showing the following:
2.2. Oblique subcostal transversus abdominis plane block
The transducer was placed 2 cm below the xiphoid process and then moved along the subcostal edge to locate the rectus abdominis muscle and the transversus abdominis. A 21G × 150 mm needle was used to inject 20 ml of 0.25% bupivacaine along the subcostal line within the transversus abdominis plane on both sides (Figure 2).
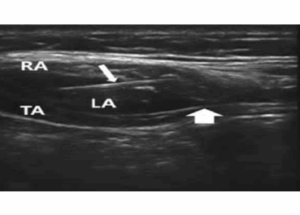
Figure 2: Ultrasound image of oblique subcostal transversus abdominis plane block showing the block needle (small arrow), transversus abdominis plane (big arrow), rectus abdominis muscle (RA) and transversus abdominis muscle (TA).
Surgery was started with a standard protocol in both groups 15 minutes after the injections. Neuromuscular block reversal and extubation followed the same protocol in both groups. The block was considered unsuccessful if the heart rate or MAP increased by more than 30% of the baseline reading after skin incision; in this case, the patient was given 0.1 mg/kg nalbuphine as an analgesic.
2.3. Data and outcomes
The VAS was used to assess pain intensity at 30 min, 2 h, 4 h, 6 h, 12 h, and 24 h postoperatively. Patients received nalbuphine 0.05 mg/kg as rescue analgesia if the pain score was ³ 4.
In addition to recording the hemodynamic parameters and pain scores, the total fentanyl and nalbuphine administered, the block failure rate, the time taken to perform a successful block, and the incidence of complications were recorded.
The primary outcome was the total dose of IV nalbuphine received during the first 24 hours. The secondary outcomes were the visual analog scale score, intraoperative fentanyl consumption, block failure, time to a successful block, and postoperative complications (intravascular injection, intestinal perforation, and pneumothorax).
2.4. Statistical analysis
Statistical analyses were performed via SPSS v26 (IBM Inc., Chicago, IL, USA) and Stata 18 (Stata Corp, College Station, TX, USA). The normality of the data distribution was assessed via the Shapiro‒Wilk test and histograms. For quantitative parametric variables, the results are presented as the means and standard deviations (SDs), and comparisons between the two groups were made via unpaired Student's t-tests. Nonparametric quantitative data are reported as medians and interquartile ranges (IQRs) and were analyzed with the Mann‒Whitney test. Qualitative variables are expressed as frequencies and percentages (%), with analyses conducted via the chi-square test or Fisher's exact test, as appropriate. Repeated measures analysis was conducted via the random effects model, and the β coefficient and its 95% confidence interval (CI) were reported. A two-tailed P value of < 0.05 was considered statistically significant.
Fifty-nine patients were assessed for eligibility; 13 did not meet the criteria, and six refused to participate in the study. The remaining patients were randomly allocated into two groups (A and B). Flowchart of the study is presented in Figure 3. The mean age was 39 years in Group A and 38 years in Group B (P = 0.720), and females were the predominant sex (16 (80%) vs. 18 (90%); P = 0.661).
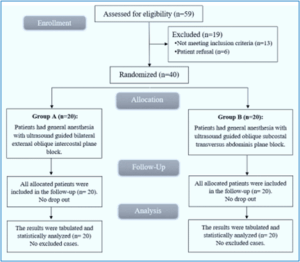
Figure 3: CONSORT flowchart of the enrolled patients
Body mass index, ASA physical status, and duration of surgery were not significantly different between the study groups (Table 1).
The intraoperative heart rate was lower in Groups A but statistically insignificant at baseline, 5 min after intubation, 5 min after block, skin incision, 10 min, 20 min, 80 min, 90 min and the end of surgery (Figure 4).
The intraoperative heart rate was significantly lower at 30 min (71.2 ± 8.88 vs. 78.45 ± 12.96 b/min), 40 min (68.6 ± 9.63 vs. 78.3 ± 16.9 b/min), 50 min (66.1 ± 9.2 vs. 72.55 ± 8.38 b/min), 60 min (64.78 ± 7.89 vs. 70.35 ± 8.48 b/min) and 70 min (61.57 ± 7.09 vs. 67.88 ± 8.49 b/min) in Group A than in Group B. A random effect model revealed that the overall trend of the heart rate was greater in Group B (β: 13.7 (95% CI: 7.5- 19.9); P < 0.001) (Figure 4).
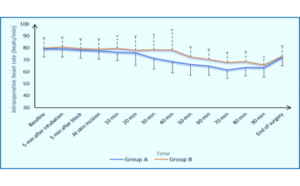
Figure 4: Comparison of the intraoperative heart rates
The intraoperative MAP was lower in Groups A but insignificantly different at baseline, 5 min after intubation, 5 min after block, skin incision, 10 min, 20 min, 80 min, 90 min and the end of surgery (Figure 5). The intraoperative MAP was significantly lower at 30 min (101.75 ± 4.84 vs. 107.3 ± 10.16 mmHg), 40 min (99.05 ± 4.94 vs. 106.1 ± 12.82 mmHg), 50 min (96.35 ± 4.7 vs. 101.8 ± 2.97 mmHg), 60 min (96.78 ± 5.3 vs. 99.85 ± 3.17 mmHg) and 70 min (95.93 ± 5.2 vs. 99.13 ± 3.28 mmHg) in Group A than Group B. Repeated measures analysis revealed greater MAP in Group B thanin Group A (β: 9.8 (95% CI: 5.1–14.5); P < 0.001) (Figure 5).
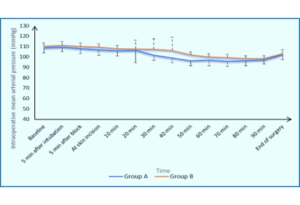
Figure 5: Comparison of intraoperative blood pressure data of two Groups
Time to a successful block, fentanyl requirements, and consumption were comparable between the two groups. The time to rescue analgesia was longer in Group A than Group B (P < 0.001), and nalbuphine consumption was lower in Group A (P = 0.025) (Table 2).
The VAS score was significantly lower at 4 h and 6 h in Group A than in Group B (P < 0.001 and 0.021, respectively). The random effects model indicated a greater pain score in Group B (β: 0.82 (95% CI: 0.5–1.2); P < 0.001) Figure 6.
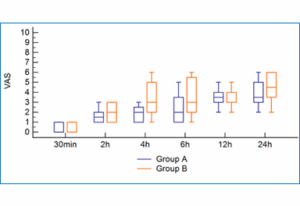
Figure 6: Comparison of the VAS pain scores between two Groups
This study compared the efficacy of intra- and postoperative analgesia between EOIP block and OSTAP block in laparoscopic cholecystectomy. The study revealed that the intraoperative heart rate and MAP were lower in the EOIP block group than in the OSTAP group. Furthermore, the time to first request for rescue analgesia was significantly longer in EOIP block, and the total dose of nalbuphine consumed and the postoperative VAS score were lower with EOIP block compared to OSTAP block.
Compared with our findings, Yahya et al. conducted a randomized controlled study on 72 patients with ASA I and II, who were scheduled for bariatric surgery and compared EOIP block and pre-incisional local infiltration with a local anesthetic agent. 14 They reported that EOIP block significantly reduced the intraoperative heart rate and MAP. Helwa and associates evaluated EOIP block for upper abdominal operations and reported that fentanyl consumption was significantly lower in the EOIP block group than in the control group.15
The beneficial effects of EOIP block reported in this study on increasing the time to rescue analgesia and reducing nalbuphine consumption have been reported in other studies. Korkusuz and associates conducted a randomized controlled study on 80 patients scheduled for LC and compared EOIP block to a control group. They reported that the total amount of opioids consumed was significantly lower in the EOIP block group.9 On the other hand, Selim and associates reported that the time to request rescue analgesia and the total dose of opioids consumed were not significantly different between the EOIP block and OSTAP block groups.16 Their study included 34 patients in each group, and postoperative paracetamol d tramadol were used.
In contrast to our findings, Selim et al. reported that the VAS score was not significantly different between the EOIP block and OSTAP groups at various time intervals.16
The findings of this study suggest that ultrasound-guided bilateral EOIP block is an effective technique for providing analgesia in patients undergoing LC. This approach has shown promise in enhancing patient comfort and minimizing postoperative pain. To build on these findings, further studies should be conducted in other centers to compare the results and validate the efficacy of this technique. Additionally, research should involve larger sample sizes to ensure the accuracy and generalization of the results.
Furthermore, comparisons with other analgesic blocks will help determine the relative effectiveness of this technique. Finally, expanding research to include various surgical procedures will provide insights into the versatility and applicability of ultrasound-guided bilateral EOIP block beyond LC. This comprehensive approach will contribute to improving pain management strategies in surgical settings.
This study is limited by its single-center experience, and the generalization of the results to other centers may not be applicable. The technique was evaluated in patients who underwent LC, and its application in other surgical procedures needs further investigation. The procedure could also be affected by the experience of the treating physicians, and establishing training standards is required to compare the outcomes between different centers appropriately.
Another important limitation is the relatively small sample size of 20 patients per group, which may limit the statistical power to detect smaller but potentially clinically relevant differences, particularly in secondary outcomes. Although our sample size was calculated based on expected differences in opioid consumption, the study may not have been adequately powered for all measured endpoints. Larger, multicenter studies are therefore necessary to validate these findings, improve generalizability, and further explore the comparative efficacy of EOIP block in broader surgical populations.
Additionally, the absence of a control group receiving either a sham block or standard systemic analgesia limits the interpretation of the absolute efficacy of both EOIP block and OSTAP block. Without a non-block comparator, it is difficult to determine the extent to which each block contributes to analgesia beyond what would be achieved with systemic medications alone. Future studies should incorporate a third arm involving standard systemic opioid-based analgesia or a placebo block to allow a more comprehensive assessment of the analgesic value and clinical utility of EOIP block and OSTAP block in laparoscopic cholecystectomy.
Ultrasound-guided bilateral external oblique intercostal plane block provides superior analgesia than oblique subcostal transversus abdominis plane block with better intraoperative hemodynamics, a longer time to rescue analgesia, and a lower total opioid dose and postoperative pain score for patients undergoing laparoscopic cholecystectomy.
7. Data availability
Numerical data generated in this study is available with the authors.
8. Conflicts of interests
The authors declare that they have no competing interests
9. Funding
No external or industry funding was involved.
10. Ethical approval
The research was approved by the Research Ethics Committee of the Faculty of Medicine, Cairo University. Written informed consent was obtained from every patient or her guardian.
11. Trial registration
The trial was registered in the Pan African Clinical Trial Registry (PACTR202406698979681).
12. Authors contribution
AA: Assembled the data for the study
MM: Assistance in preparing the manuscript and interpreting the data
YH: Preparing the manuscript and assistance in interpreting the data
MI: Study design and collection of the data
DA: Revision of the manuscript and data collection
All authors approved the final work.
Author affiliations:
- Ahmed Abdalwahab, Department of Anesthesia, Faculty of Medicine Cairo University, Cairo, Egypt; Email: dr.ahmedabdalwahab@gmail.com; {ORCID:0009-0007-7814-8805}
- Mohammed Mansour, Department of Anesthesia, Faculty of Medicine Cairo University, Cairo, Egypt; Email: shazamansour@yahoo.com
- Yahya Hammad, Department of Anesthesia, Faculty of Medicine Cairo University, Cairo, Egypt; Email: yahya196cm@gmail.com
- Mohammed Ismael, Department of Anesthesia, Faculty of Medicine Cairo University, Cairo, Egypt; Email: dr.mohammed.os96@gmail.com
- Doaa Abdelfattah, Department of Anesthesia, Faculty of Medicine Cairo University, Cairo, Egypt; Email: fz.doaa@hotmail.com
ABSTRACT
Background & objective: The superiority of external oblique intercostal plane (EOIP) block over oblique subcostal transversus abdominis plane (OSTAP) block for intra and postoperative analgesia in laparoscopic cholecystectomy has not been established. Therefore, this study compared the efficacy of the analgesic effect between EOIP block and OSTAP block in patients undergoing laparoscopic cholecystectomy.
Methodology: This randomized controlled clinical trial was conducted on adult patients who underwent elective laparoscopic cholecystectomy from 2023 to 2024. Patients were randomly allocated into two groups at a 1:1 ratio. Group A (n = 20) included patients who received ultrasound-guided bilateral EOIP block, and Group B (n = 20) included patients who received ultrasound-guided OSTAP block.
Results: Group A had a longer time to rescue analgesia (7.05 ± 0.76 vs. 4.95 ± 0.83 min, P < 0.001), and consumed a significantly lower total dose of nalbuphine (0.1 ± 0.02 vs. 0.12 ± 0.02 mg/kg; P = 0.025). The pain score was lower in Group A, particularly at 4 and 6 hours postoperatively (P < 0.001).
Conclusions: Ultrasound-guided bilateral EOIP block provides superior analgesia than OSTAP with a longer time to rescue analgesia, lower opioid consumption, and improved early postoperative pain scores in patients undergoing laparoscopic cholecystectomy.
Abbreviations: EOIP: external oblique intercostal plane, IQR: interquartile ranges. LP: Laparoscopic cholecystectomy, OSTAP: oblique subcostal transversus abdominis plane, VAS: visual analog scale,
Keywords: external oblique intercostal plane block; laparoscopic cholecystectomy; Pain; subcostal transversus abdominis plane block; ultrasound-guided analgesia
Citation: Abdalwahab A, Mansour M, Hammad YM, Ismael MO, Abdelfattah DF. Bilateral ultrasound-guided external oblique intercostal plane block versus bilateral subcostal transversus abdominis plane block in laparoscopic cholecystectomy: a randomized controlled trial. Anaesth. pain intensive care 2025;29(4):363-70. DOI: 10.35975/apic.v29i4.2821
Received: March 02, 2025; Revised: April 20, 2025; Accepted: May 01, 2025
1. INTRODUCTION
Laparoscopic cholecystectomy (LC) has become the standard approach for the surgical management of gallbladder stones.1-3 Postoperative pain, which can be either visceral or somatic, is still a significant clinical issue after LC. Visceral pain occurs due to gallbladder resection and carbon dioxide (CO2) irritation of the diaphragm, and somatic pain occurs from incision sites.2
Postoperative pain is a significant contributing factor to increased morbidity and mortality after LC and halts same-day discharge.3,4 Therefore, several analgesic techniques were used to ameliorate the deleterious effects of postoperative pain and improve patient outcomes.5 Ultrasound-guided transversus abdominis plane block is one of the methods used for postoperative analgesia, especially for controlling somatic pain in abdominal surgeries. In this technique, local anesthetic is injected into the fascial plane between the transversus abdominis and internal oblique muscles.6
Studies have shown that the subcostal approach for TAP (OSTAP) block could have beneficial analgesic effects on the area above the umbilicus because it blocks the area supplied by T7-12.7,8 External oblique intercostal plane block (EOIP block), in which the local anesthetic is injected in the tissue plane between the external oblique and intercostal muscles between the sixth and seventh ribs, is a modification of fascial plane blocks that target the upper lateral abdominal walls.9 We hypothesize that the external oblique intercostal plane block might be more efficient than the oblique subcostal TAP block in terms of intra- and postoperative analgesia in LC. Therefore, our study compared the efficacy of the analgesic effect between EOIP block and OSTAP block in patients undergoing LC.
2. METHODOLOGY
We conducted a randomized clinical trial on adult patients who underwent elective LC from May 2023 to May 2024 at Cairo University Hospital, Cairo, Egypt. The study was conducted on adult patients aged between 18 and 60 years, with American Society of Anesthesiologists (ASA) classes I and II. Patients with neurological or psychological disorders, end-organ failure, bleeding abnormalities, infections at the injection sites, or allergies to amide local anesthetics were excluded.
The Research Ethics Committee of the Faculty of Medicine, Cairo University approved the research. Patients signed informed consent before participation.
The trial was registered in the Pan African Clinical Trial Registry (PACTR202406698979681).
The study was conducted per the Declaration of Helsinki.10 We reported the trial results according to the CONSORT guideline.11
According to a previous study, the total tramadol consumption in the first 24 hours after surgery was 199 ± 27.7 mg in patients receiving OSTAP who underwent LC.12 Using an opioid conversion table, this dose is equivalent to 19.9 ± 2.77 mg nalbuphine.13 A total sample of 34 was needed to detect a 5 mg difference in nalbuphine consumption, and we used a more conservative common standard deviation of 5. The sample size was calculated to achieve a study power of 80% and an alpha error of 0.05. The number of envelopes was increased to 40 (20 per group) to compensate for possible dropouts. The sample size was calculated via MedCalc Software V14.
Patients were randomly allocated via blocked randomization with a block size between 4 and 6. The randomization sequence was generated via (www.randomization.com) by the principal investigator. The randomization sequence was concealed in sealed envelopes and opened by an independent nurse. Patients were randomized into two groups at a 1:1 ratio. Group A (n = 20) included patients who received ultrasound-guided bilateral EOIP block, and Group B (n = 20) included patients who received ultrasound-guided OSTAP block. Patients were blinded to the allocated treatment.
Preoperative assessment was performed for all patients scheduled for LC, including proper medical and surgical history, chest, airway, and planned regional block examination site. All preoperative investigations were revised to assess enrollment eligibility. Patients were educated about the visual analog scale (VAS) and how to quantify pain intensity.
Intraoperatively, patients were connected to a noninvasive blood pressure monitor, electrocardiogram, and pulse oximeter, and baseline readings were recorded prior to induction of anesthesia, five minutes after endotracheal intubation, five minutes after the sensory block, before the skin incision, and then every 10 minutes. Induction and maintenance of anesthesia followed the same protocol in both groups.
All patients received 1 gm of paracetamol and 30 mg of ketorolac IV for control of visceral pain. A dose of 0.5 µg/kg fentanyl was given as rescue analgesia at any time of the surgery if needed in the case of increased mean arterial blood pressure (MAP) and heart rate by 30% or more above the baseline reading, despite adequate ventilation, hypnosis, muscle relaxation, and hydration.
2.1. External oblique intercostal plane block
The patients were placed supine, and the skin was prepared. The ultrasound transducer was placed between the anterior axillary and midclavicular lines at the level of the 6th rib. The anesthesiologist injected 20 ml of 0.25% bupivacaine bilaterally into the external oblique intercostal plane via a 22G, 80 mm block needle (Figure 1).
Figure 1: Ultrasound image of external oblique intercostal plane block showing the following:
- Block needle
- The 6th rib
- External oblique muscle
- Intercostal muscle
2.2. Oblique subcostal transversus abdominis plane block
The transducer was placed 2 cm below the xiphoid process and then moved along the subcostal edge to locate the rectus abdominis muscle and the transversus abdominis. A 21G × 150 mm needle was used to inject 20 ml of 0.25% bupivacaine along the subcostal line within the transversus abdominis plane on both sides (Figure 2).
Figure 2: Ultrasound image of oblique subcostal transversus abdominis plane block showing the block needle (small arrow), transversus abdominis plane (big arrow), rectus abdominis muscle (RA) and transversus abdominis muscle (TA).
Surgery was started with a standard protocol in both groups 15 minutes after the injections. Neuromuscular block reversal and extubation followed the same protocol in both groups. The block was considered unsuccessful if the heart rate or MAP increased by more than 30% of the baseline reading after skin incision; in this case, the patient was given 0.1 mg/kg nalbuphine as an analgesic.
2.3. Data and outcomes
The VAS was used to assess pain intensity at 30 min, 2 h, 4 h, 6 h, 12 h, and 24 h postoperatively. Patients received nalbuphine 0.05 mg/kg as rescue analgesia if the pain score was ³ 4.
In addition to recording the hemodynamic parameters and pain scores, the total fentanyl and nalbuphine administered, the block failure rate, the time taken to perform a successful block, and the incidence of complications were recorded.
The primary outcome was the total dose of IV nalbuphine received during the first 24 hours. The secondary outcomes were the visual analog scale score, intraoperative fentanyl consumption, block failure, time to a successful block, and postoperative complications (intravascular injection, intestinal perforation, and pneumothorax).
2.4. Statistical analysis
Statistical analyses were performed via SPSS v26 (IBM Inc., Chicago, IL, USA) and Stata 18 (Stata Corp, College Station, TX, USA). The normality of the data distribution was assessed via the Shapiro‒Wilk test and histograms. For quantitative parametric variables, the results are presented as the means and standard deviations (SDs), and comparisons between the two groups were made via unpaired Student's t-tests. Nonparametric quantitative data are reported as medians and interquartile ranges (IQRs) and were analyzed with the Mann‒Whitney test. Qualitative variables are expressed as frequencies and percentages (%), with analyses conducted via the chi-square test or Fisher's exact test, as appropriate. Repeated measures analysis was conducted via the random effects model, and the β coefficient and its 95% confidence interval (CI) were reported. A two-tailed P value of < 0.05 was considered statistically significant.
3. RESULTS
Fifty-nine patients were assessed for eligibility; 13 did not meet the criteria, and six refused to participate in the study. The remaining patients were randomly allocated into two groups (A and B). Flowchart of the study is presented in Figure 3. The mean age was 39 years in Group A and 38 years in Group B (P = 0.720), and females were the predominant sex (16 (80%) vs. 18 (90%); P = 0.661).
Figure 3: CONSORT flowchart of the enrolled patients
Body mass index, ASA physical status, and duration of surgery were not significantly different between the study groups (Table 1).
| Table 1: Comparison of the baseline data between patients of two groups | |||
| Variables | Group A
(n = 20) |
Group B
(n = 20) |
P value |
| Age (years) | 39.1 ± 9.82 | 37.9 ± 11.17 | 0.720 |
| Females | 16 (80%) | 18 (90%) | 0.661 |
| Weight (kg) | 77.25 ± 11.22 | 79.85 ± 7.58 | 0.396 |
| Height (cm) | 167.55 ± 7.24 | 167.75 ± 5.88 | 0.924 |
| BMI (kg/m2) | 27.55 ± 3.91 | 28.43 ± 2.93 | 0.426 |
| ASA physical status
· I · II |
12 (60%) 8 (40%) |
11 (55%) 9 (45%) |
0.749 |
| Duration of surgery (min) | 81.75 ± 15.33 | 85 ± 11.58 | 0.454 |
| BMI: Body Mass Index, ASA: American Society of Anesthesiologists
The data are presented as the means and standard deviations or counts and percentages. P < 0.05 considered significant |
|||
The intraoperative heart rate was lower in Groups A but statistically insignificant at baseline, 5 min after intubation, 5 min after block, skin incision, 10 min, 20 min, 80 min, 90 min and the end of surgery (Figure 4).
The intraoperative heart rate was significantly lower at 30 min (71.2 ± 8.88 vs. 78.45 ± 12.96 b/min), 40 min (68.6 ± 9.63 vs. 78.3 ± 16.9 b/min), 50 min (66.1 ± 9.2 vs. 72.55 ± 8.38 b/min), 60 min (64.78 ± 7.89 vs. 70.35 ± 8.48 b/min) and 70 min (61.57 ± 7.09 vs. 67.88 ± 8.49 b/min) in Group A than in Group B. A random effect model revealed that the overall trend of the heart rate was greater in Group B (β: 13.7 (95% CI: 7.5- 19.9); P < 0.001) (Figure 4).
Figure 4: Comparison of the intraoperative heart rates
The intraoperative MAP was lower in Groups A but insignificantly different at baseline, 5 min after intubation, 5 min after block, skin incision, 10 min, 20 min, 80 min, 90 min and the end of surgery (Figure 5). The intraoperative MAP was significantly lower at 30 min (101.75 ± 4.84 vs. 107.3 ± 10.16 mmHg), 40 min (99.05 ± 4.94 vs. 106.1 ± 12.82 mmHg), 50 min (96.35 ± 4.7 vs. 101.8 ± 2.97 mmHg), 60 min (96.78 ± 5.3 vs. 99.85 ± 3.17 mmHg) and 70 min (95.93 ± 5.2 vs. 99.13 ± 3.28 mmHg) in Group A than Group B. Repeated measures analysis revealed greater MAP in Group B thanin Group A (β: 9.8 (95% CI: 5.1–14.5); P < 0.001) (Figure 5).
Figure 5: Comparison of intraoperative blood pressure data of two Groups
Time to a successful block, fentanyl requirements, and consumption were comparable between the two groups. The time to rescue analgesia was longer in Group A than Group B (P < 0.001), and nalbuphine consumption was lower in Group A (P = 0.025) (Table 2).
| Table 2: Comparison of the intraoperative data between patients of Group A and Group B | |||
| Variables | Group A
(n = 20) |
Group B
(n = 20) |
P value |
| Time to perform successful block (min) | 5.9 ± 1.8 | 6.25 ± 1.41 | 0.498 |
| Need for fentanyl consumption | 4 (20%) | 5 (25%) | 0.537 |
| Fentanyl consumption ((µg/kg) | 0.1 ± 0.21 | 0.13 ± 0.22 | 0.714 |
| Time to first request of rescue analgesia (h) | 7.05 ± 0.76 | 4.95 ± 0.83 | < 0.001 |
| Total dose of nalbuphine consumption (mg/kg) | 0.1 ± 0.02 | 0.12 ± 0.02 | 0.025 |
| The data are presented as the means and standard deviations or counts and percentages.
P < 0.05 considered significant |
|||
The VAS score was significantly lower at 4 h and 6 h in Group A than in Group B (P < 0.001 and 0.021, respectively). The random effects model indicated a greater pain score in Group B (β: 0.82 (95% CI: 0.5–1.2); P < 0.001) Figure 6.
Figure 6: Comparison of the VAS pain scores between two Groups
4. DISCUSSION
This study compared the efficacy of intra- and postoperative analgesia between EOIP block and OSTAP block in laparoscopic cholecystectomy. The study revealed that the intraoperative heart rate and MAP were lower in the EOIP block group than in the OSTAP group. Furthermore, the time to first request for rescue analgesia was significantly longer in EOIP block, and the total dose of nalbuphine consumed and the postoperative VAS score were lower with EOIP block compared to OSTAP block.
Compared with our findings, Yahya et al. conducted a randomized controlled study on 72 patients with ASA I and II, who were scheduled for bariatric surgery and compared EOIP block and pre-incisional local infiltration with a local anesthetic agent. 14 They reported that EOIP block significantly reduced the intraoperative heart rate and MAP. Helwa and associates evaluated EOIP block for upper abdominal operations and reported that fentanyl consumption was significantly lower in the EOIP block group than in the control group.15
The beneficial effects of EOIP block reported in this study on increasing the time to rescue analgesia and reducing nalbuphine consumption have been reported in other studies. Korkusuz and associates conducted a randomized controlled study on 80 patients scheduled for LC and compared EOIP block to a control group. They reported that the total amount of opioids consumed was significantly lower in the EOIP block group.9 On the other hand, Selim and associates reported that the time to request rescue analgesia and the total dose of opioids consumed were not significantly different between the EOIP block and OSTAP block groups.16 Their study included 34 patients in each group, and postoperative paracetamol d tramadol were used.
In contrast to our findings, Selim et al. reported that the VAS score was not significantly different between the EOIP block and OSTAP groups at various time intervals.16
The findings of this study suggest that ultrasound-guided bilateral EOIP block is an effective technique for providing analgesia in patients undergoing LC. This approach has shown promise in enhancing patient comfort and minimizing postoperative pain. To build on these findings, further studies should be conducted in other centers to compare the results and validate the efficacy of this technique. Additionally, research should involve larger sample sizes to ensure the accuracy and generalization of the results.
Furthermore, comparisons with other analgesic blocks will help determine the relative effectiveness of this technique. Finally, expanding research to include various surgical procedures will provide insights into the versatility and applicability of ultrasound-guided bilateral EOIP block beyond LC. This comprehensive approach will contribute to improving pain management strategies in surgical settings.
5. LIMITATIONS
This study is limited by its single-center experience, and the generalization of the results to other centers may not be applicable. The technique was evaluated in patients who underwent LC, and its application in other surgical procedures needs further investigation. The procedure could also be affected by the experience of the treating physicians, and establishing training standards is required to compare the outcomes between different centers appropriately.
Another important limitation is the relatively small sample size of 20 patients per group, which may limit the statistical power to detect smaller but potentially clinically relevant differences, particularly in secondary outcomes. Although our sample size was calculated based on expected differences in opioid consumption, the study may not have been adequately powered for all measured endpoints. Larger, multicenter studies are therefore necessary to validate these findings, improve generalizability, and further explore the comparative efficacy of EOIP block in broader surgical populations.
Additionally, the absence of a control group receiving either a sham block or standard systemic analgesia limits the interpretation of the absolute efficacy of both EOIP block and OSTAP block. Without a non-block comparator, it is difficult to determine the extent to which each block contributes to analgesia beyond what would be achieved with systemic medications alone. Future studies should incorporate a third arm involving standard systemic opioid-based analgesia or a placebo block to allow a more comprehensive assessment of the analgesic value and clinical utility of EOIP block and OSTAP block in laparoscopic cholecystectomy.
6. CONCLUSION
Ultrasound-guided bilateral external oblique intercostal plane block provides superior analgesia than oblique subcostal transversus abdominis plane block with better intraoperative hemodynamics, a longer time to rescue analgesia, and a lower total opioid dose and postoperative pain score for patients undergoing laparoscopic cholecystectomy.
7. Data availability
Numerical data generated in this study is available with the authors.
8. Conflicts of interests
The authors declare that they have no competing interests
9. Funding
No external or industry funding was involved.
10. Ethical approval
The research was approved by the Research Ethics Committee of the Faculty of Medicine, Cairo University. Written informed consent was obtained from every patient or her guardian.
11. Trial registration
The trial was registered in the Pan African Clinical Trial Registry (PACTR202406698979681).
12. Authors contribution
AA: Assembled the data for the study
MM: Assistance in preparing the manuscript and interpreting the data
YH: Preparing the manuscript and assistance in interpreting the data
MI: Study design and collection of the data
DA: Revision of the manuscript and data collection
All authors approved the final work.
13. REFERENCES
- Kim H, Lee H. Effects of a preoperative patient-controlled analgesia education program using smart learning in laparoscopic cholecystectomy patients. Pain Manag Nurs. 2024;25(6):e428-e435. [PubMed] DOI: 1016/j.pmn.2024.06.003
- Datta P, Roy A. Role of intraperitoneal instillation of bupivacaine after laparoscopic cholecystectomy for postoperative pain management: a randomized controlled trial. Int Surg J. 2020;7(10):3239. DOI: 18203/2349-2902.isj20203986
- Vijayaraghavalu S, Sekar EB. A comparative study on the postoperative analgesic effects of intraperitoneal bupivacaine vs normal saline following laparoscopic cholecystectomy. Cureus. 2021;13(3):e14151. [PubMed] DOI: 7759/cureus.14151
- Petersen PL, Stjernholm P, Kristiansen VB, Torup H, Hansen EG, Mitchell AU, et al. Effect of transversus abdominis plane block after laparoscopic cholecystectomy in day-case surgery: a randomized clinical trial. Anesth Analg. 2012;115:527-33. [PubMed] DOI: 1213/ANE.0b013e318261f16e
- Dost B, De Cassai A, Balzani E, Geraldini F, Tulgar S, Ahıskalıoğlu A, et al. Analgesic benefits of preoperative vs postoperative transversus abdominis plane block for laparoscopic cholecystectomy: a meta-analysis. BMC Anesthesiol. 2023;23(1):408. [PubMed] DOI: 1186/s12871-023-02369-6
- Rahimzadeh P, Faiz SHR, Latifi-Naibin K, Alimian M. Preemptive vs postoperative ultrasound-guided bilateral TAP block on pain relief after laparoscopic cholecystectomy. Sci Rep. 2022;12(1):623. [PubMed] DOI: 1038/s41598-021-04552-6
- Suseela IM, Anandan K, Aravind A, Kaniyil S. Subcostal TAP block vs port-site infiltration with bupivacaine in laparoscopic cholecystectomy. Indian J Anaesth. 2018;62:497-501. [PubMed] DOI: 4103/ija.IJA_55_18
- Ma JF, Jiang YF, Tang S, Wang BF, Lian Q, Xie Z, et al. Analgesic efficacy of ultrasound-guided subcostal TAP block. Medicine (Baltimore). 2017;96(10):e6309. [PubMed] DOI: 1097/MD.0000000000006309
- Korkusuz M, Basaran B, Et T, Bilge A, Yarımoğlu R, Yildirim H. Bilateral external oblique intercostal plane block in laparoscopic cholecystectomy. Saudi Med J. 2023;44:1037-46. [PubMed] DOI: 15537/smj.2023.44.10.20230350
- World Medical Association. Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310:2191-4. [PubMed] DOI: 1001/jama.2013.281053
- Schulz KF, Altman DG, Moher D. CONSORT 2010 statement: updated guidelines for reporting parallel group randomized trials. Ann Intern Med. 2010;152:726-32. [PubMed] DOI: 7326/0003-4819-152-11-201006010-00232
- Altıparmak B, Korkmaz Toker M, Uysal AI, Kuşçu Y, Gümüş Demirbilek S. ESP block vs oblique subcostal TAP block for postoperative analgesia in laparoscopic cholecystectomy: a randomized trial. J Clin Anesth. 2019;57:31-6. [PubMed] DOI: 1016/j.jclinane.2019.03.012
- McPherson ML. Demystifying opioid conversion calculations: a guide for effective dosing. Bethesda (MD): Am Soc Health-Syst Pharm; 2018.
- Abdelrahman B, Yahya MM, Hammad NM. Comparison between External Oblique Intercostal Plane Block (EOI) and Pre-Incisional Local Infiltration on Intra and Acute Post-Operative Pain Control in Adult Patients Undergoing Bariatric Surgeries: Randomized Controlled Prospective Comparative Study. Med J Cairo Univ. 2024; 92(03): 57-63. DOI: 21608/mjcu.2024.353086
- Helwa AM, Rady AA, Hafez D, Yousef I, Safan AG. Efficacy of ultrasound-guided external oblique intercostal plane block in upper abdominal surgeries: a randomized trial. Egypt J Hosp Med. 2024;96(1):2698-705. DOI: 21608/ejhm.2024.372537
- Selim ÇM, Halide S, Cem ÇE, Onur K, Sedat H, Senem U. Unilateral EOIPB vs subcostal TAP block in laparoscopic cholecystectomy: a randomized prospective study. Surg Innov. 2024;31:381-8. [PubMed] DOI: 1177/15533506241256529