Omar Al Misnid 1, 2
Author’s affiliations:
Regional blocks for the anterolateral chest wall are challenging in regard to the anatomical basics and innervation, the limitation of evidence, lack of guidelines, and wide discrepancy in practice among health practitioners. Despite the challenges, new fascial plane blocks have been used recently more often as analgesic techniques. In very few occasions these techniques have been reported in literature as surgical blocks in certain cases where General anesthesia was not the favorable choice. In this case, we present a challenging case which was postponed due to her high risk for general anesthesia due to multiple comorbidities and for status optimization. At the same time, her procedure was time sensitive to diagnose her medical illness and initiate the proper management.
Keywords: Regional Anesthesia; Pain Management; Fascia Plane Block; Nerve Block
Citation: Misnid OA. Regional anesthesia for axillary lymph node excisional biopsy in a patient with anterior mediastinal mass. Anaesth. pain intensive care 2025;29(3):711-714. DOI: 10.35975/apic.v29i3.2779
Received: February 11, 2025; Revised: February 15, 2025; Accepted: February 16, 2025
Airway management in patients with difficult airway is a highly challenging task, especially if there is partial or complete compression of the trachea. The anesthetist has to think out of the box solutions to facilitate the planned surgery, while ensuring the safety of the patient. Regional anesthesia comprises of peripheral nerve or plexus blocks, which has been employed with success in theses complex cases. We present this case report to highlight the alternatives when general anesthesia is judged to be too risky for the patient.
A 42-year-old female patient presented with multiple swellings in her upper body mainly in her neck and axillae for the last few months, accompanied with night sweats, shortness of breath, cough, dysphagia, chocking at night and weight loss. The patient at presentation looked in distress, and upon examination she had generalized lymphadenopathy with compressive symptoms. Initial work-up was requested including laboratory investigations, chest X-ray (Figure 1), CT chest with contrast, echocardiography, and lymph node biopsy. Laboratory work-up including complete blood count, renal profile, liver function tests, was unremarkable, except for low hemoglobin, which was 96 g/L. CT chest with contrast showed multiple compartmental soft tissue masses involving the superior, anterior, and middle mediastinum.
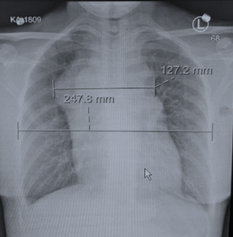
Figure 1: Chest X-ray PA view
The largest mass measured 5.3 x 5.5 cm with mass effect on great thoracic vessels, the right side of pericardium, the anterior carina, and the right main stem bronchus (Figure 2). In addition, there was right lower lobe consolidation with mild bilateral pleural effusion, moderate pericardial effusion and bilateral axillary nodular masses, which suggested a diagnosis of lymphoma (Figure 2).
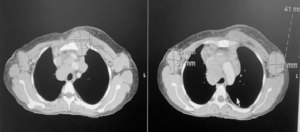
Figure 2: CT scan chest showing multiple compartmental soft tissue masses involving the superior, anterior, and middle mediastinum
The echocardiography showed moderate size pericardial effusion with elevated intrapericardial pressure without tamponade. The patient needed a definitive diagnosis to start the proper medical management as previous needle biopsy suggested lymphoma but was not conclusive. The patient was booked for left axillary lymph node excisional biopsy with high-risk consent for general anesthesia with intensive care unit (ICU) bed standby postoperatively. On the day of surgery, the primary anesthesiologist reviewed the patient carefully with a probability to postpone the procedure due to non-availability of ICU bed and patient risk of mass effect and active pneumonia. A detailed discussion was held among the patient, the surgeon, the anesthesiologist, and the primary team, about the risks, the benefits, and the alternative approaches. The patient and the medical team agreed with the primary anesthesiologist plan to go for the ultrasound guided pectoralis (PECS) block.
In the operating room, the patient was placed in the supine position with slight back up to ensure patient comfort and cooperation during the regional block. The standard monitors were applied, including pulse oximetry, non-invasive blood pressure, and ECG with two peripheral intravenous cannulas secured. Left sided ultrasound guided in-plane approach and 22G 50 mm block needle was used to under Sonoplex probe, to perform PECS II under aseptic technique (Figure 3).
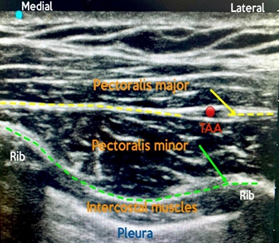
Figure 3: PECS II Sono-anatomy. TAA, branch of thoracoacromial artery; green, plane for first injection (20 mL); yellow, plane for second injection (10 mL)
A mixture of lidocaine 1% and ropivacaine 0.25% was used for the blocks; a total of 10 mL was injected between the pectoralis major and minor, and another 20 mL was injected below the pectoralis minor. Post block, the patient's position was changed to Trendelenburg position with right side up for about 15 min with continuous communication and reassurance to the patient. The patient's position was adjusted for surgical exposure, and just before skin incision the surgical area was tested for pain with surgical forceps to ensure that the patient was pain free. A skin incision was made and a lymph node on measuring 5x3x4 cm was dissected with good hemostasis and no complication. Throughout the procedure the patient’s pain score remained 0 out of 10 and her vital signs showed no changes. The surgery was done without the use of sedation or local infiltration and the patient remained pain free and fully awake throughout the procedure. Afterwards, the patient was fully awake and vitally stable, and transferred to the post-anesthesia care unit (PACU), where she was monitored for two hours. She remained hemodynamically stable with zero pain score. After monitoring for 2 hours in the PACU, the patient was transferred to the oncology ward in a stable condition.
In certain cases, avoiding general anesthesia could be safer and this patient had quite a few reasons why we must avoid general anesthesia if feasible. Anesthesia for awake surgeries involving the axillary area can be very challenging and requires collaborative teamwork. In addition, such cases are particularly challenging to be done with a single injection regional block, although pure local anesthesia infiltration is a well-known technique, no described regional anesthesia block or technique has been identified to be ideal or superior for such surgeries and only very few cases reported in literatures. While actually some data recommends against the use of any regional techniques due to the anatomical challenges in the axilla and no technique could reliably provide sufficient analgesia to the axillary region.1 The innervation of axillary area consists of multiple contributions from nerves and groups of nerves. The intercostobrachial nerve (ICBN), which is responsible for most of cutaneous supply of the axilla, and with contribution from the brachial plexus (BP) by providing additional cutaneous innervation from medial brachial cutaneous nerve (MBCN) and deep somatic innervation within the axilla mainly through the lateral and medial pectoral nerves.2 Other nerves arising from brachial plexus and contributing to anterolateral chest wall are the thoracodorsal nerve, and the long thoracic nerve, which innervate latissimus dorsi, and serratus anterior muscles, respectively.3 The axilla is also innervated by the other lateral cutaneous branches of the thoracic intercostal nerve (LCNs) in addition to ICBN (T2).
In addition to pure local anesthetic infiltration, such surgeries could be performed with regional techniques keeping in mind the essential coverage of ICBN, medial and lateral pectoral nerves (MPN and LPN) and LCNs. For ICBN block, there are several reliable regional blocks that could cover this nerve like; targeting ICBN itself, high thoracic paravertebral, PECS II, or serratus anterior blocks. While MPN and LPN could be blocked, if we do PECS I, PECS II (two pectoral fascial compartments) or supraclavicular BP block, the LCNs will be blocked in case of paravertebral, PECS II or serratus anterior block. In this case PECS II was done as the primary anesthesia with no sedation.3
In literature, regional block was used in few cases as the primary anesthesia for different procedures on the chest wall and axilla; e.g., breast surgery, axillary dissection, transthoracic arteriovenous graft repair and cardiovascular implantable electronic device with or without sedation. In one case report, the author described a case of axillary clearance under regional blocks (supraclavicular BP and ICBN blocks).2 In another case, breast conserving surgery with axillary dissection was done using PECS II, with sedation in form of dexmedetomidine infusion.4 While in another case PECS II was used as the sole anesthetic for removal of a large axillary tumor.5 A combination of PECS I, serratus anterior plane (SAP), and parasternal intercostal plane blocks with sedation in the form of propofol infusion was used for modified radical mastectomy and axillary lymph node dissection.6 Viewing such literature reinforces the limit of evidence, lack of guidelines, and wide discrepancy in the practice among anesthesiologists toward regional block preferences and opinions for surgeries involving the anterolateral chest wall and specifically the axilla.
In addition to the complexity of regional anesthesia for surgeries in the axillary area; fascial plane blocks, in general, are still one of the new evolving debatable topics regarding their value, reliability and effectiveness; particularly in case of PECS block, where there is much data in favor of recent development of such techniques.7 On the other hand, few studies have shown no benefits and even some showed an increase in the reported pain scores with PECS group.7 Such discrepancies might be due to these blocks being relatively recently introduced with lack of a particular end point target. In addition to the numerous factors which could affect the fascial plane blocks, Elsharkawy et al. described the basics of facial plane and how many factors could influence the effectiveness, the quality and the spread of the block.8 Site of injection, multi injectional sites, volume of local anesthesia, biomechanical properties of the fascia, types of fasciae and fascial layers; all could influence the dermatomal spread and quality of the block.8
To better understand the value of these factors, for example the site of injection in PECS II, injecting lateral to thoracoacromial branch and close to anterior axillary line for the superficial injection and injecting between the level of third and fourth rib over the anterior axillary line for the deeper one will result in more reliable block.3,9
In this case report we do not only suggest the potential of PECS block to provide a decrease in the intraoperative and postoperative opioid consumption and lower pain scores, but we also see a potential for it to be used as the primary anesthesia for selected surgeries. In addition to the factors which influence the success of facial plane block, carefully choosing which block to perform for a specific procedure is crucial to ensure a total pain free experience. For example, PECS II block is a great block in certain chest wall surgeries; however, it is a pure somatic block and doesn’t provide visceral block. For cases where visceral coverage also needed one should think of other blocks like; erector spinae plane or midpoint transverse process to pleura blocks.3
An efficient perioperative care of a patient starts with carful preoperative assessment and discussion with all involved medical teams, and of course the patient, to formulate the best possible plan and care. Fascial plane blocks have potential to provide not only sensory block, but surgical block too, when we understand and implement them to the right procedures and patients. In the axilla with its complex innervation, fascial plane blocks could offer a proper surgical coverage and maybe with fewer side effects and complications in high risk patients.
4. Ethical considerations
Written consent was obtained from the patient to use his pictures for the academic purpose.
5. Conflict of interests
The author declares no conflict of interests.
6. Author’s contribution
Omar Al Misnid is the sole author of this case report.
Author’s affiliations:
- Assistant Professor, Department of Emergency, Critical Care & Anesthesia, College of Medicine, Qassim University, Buraydah, Saudi Arabia.
- Assistant Professor, Department of Anesthesia, Medical City, Qassim University, Buraydah, Saudi Arabia; Email: o.almisnid@qu.edu.sa; {ORCID:0000-0002-4147-9463}
ABSTRACT
Regional blocks for the anterolateral chest wall are challenging in regard to the anatomical basics and innervation, the limitation of evidence, lack of guidelines, and wide discrepancy in practice among health practitioners. Despite the challenges, new fascial plane blocks have been used recently more often as analgesic techniques. In very few occasions these techniques have been reported in literature as surgical blocks in certain cases where General anesthesia was not the favorable choice. In this case, we present a challenging case which was postponed due to her high risk for general anesthesia due to multiple comorbidities and for status optimization. At the same time, her procedure was time sensitive to diagnose her medical illness and initiate the proper management.
Keywords: Regional Anesthesia; Pain Management; Fascia Plane Block; Nerve Block
Citation: Misnid OA. Regional anesthesia for axillary lymph node excisional biopsy in a patient with anterior mediastinal mass. Anaesth. pain intensive care 2025;29(3):711-714. DOI: 10.35975/apic.v29i3.2779
Received: February 11, 2025; Revised: February 15, 2025; Accepted: February 16, 2025
1. INTRODUCTION
Airway management in patients with difficult airway is a highly challenging task, especially if there is partial or complete compression of the trachea. The anesthetist has to think out of the box solutions to facilitate the planned surgery, while ensuring the safety of the patient. Regional anesthesia comprises of peripheral nerve or plexus blocks, which has been employed with success in theses complex cases. We present this case report to highlight the alternatives when general anesthesia is judged to be too risky for the patient.
2. CASE REPORT
A 42-year-old female patient presented with multiple swellings in her upper body mainly in her neck and axillae for the last few months, accompanied with night sweats, shortness of breath, cough, dysphagia, chocking at night and weight loss. The patient at presentation looked in distress, and upon examination she had generalized lymphadenopathy with compressive symptoms. Initial work-up was requested including laboratory investigations, chest X-ray (Figure 1), CT chest with contrast, echocardiography, and lymph node biopsy. Laboratory work-up including complete blood count, renal profile, liver function tests, was unremarkable, except for low hemoglobin, which was 96 g/L. CT chest with contrast showed multiple compartmental soft tissue masses involving the superior, anterior, and middle mediastinum.
Figure 1: Chest X-ray PA view
The largest mass measured 5.3 x 5.5 cm with mass effect on great thoracic vessels, the right side of pericardium, the anterior carina, and the right main stem bronchus (Figure 2). In addition, there was right lower lobe consolidation with mild bilateral pleural effusion, moderate pericardial effusion and bilateral axillary nodular masses, which suggested a diagnosis of lymphoma (Figure 2).
Figure 2: CT scan chest showing multiple compartmental soft tissue masses involving the superior, anterior, and middle mediastinum
The echocardiography showed moderate size pericardial effusion with elevated intrapericardial pressure without tamponade. The patient needed a definitive diagnosis to start the proper medical management as previous needle biopsy suggested lymphoma but was not conclusive. The patient was booked for left axillary lymph node excisional biopsy with high-risk consent for general anesthesia with intensive care unit (ICU) bed standby postoperatively. On the day of surgery, the primary anesthesiologist reviewed the patient carefully with a probability to postpone the procedure due to non-availability of ICU bed and patient risk of mass effect and active pneumonia. A detailed discussion was held among the patient, the surgeon, the anesthesiologist, and the primary team, about the risks, the benefits, and the alternative approaches. The patient and the medical team agreed with the primary anesthesiologist plan to go for the ultrasound guided pectoralis (PECS) block.
In the operating room, the patient was placed in the supine position with slight back up to ensure patient comfort and cooperation during the regional block. The standard monitors were applied, including pulse oximetry, non-invasive blood pressure, and ECG with two peripheral intravenous cannulas secured. Left sided ultrasound guided in-plane approach and 22G 50 mm block needle was used to under Sonoplex probe, to perform PECS II under aseptic technique (Figure 3).
Figure 3: PECS II Sono-anatomy. TAA, branch of thoracoacromial artery; green, plane for first injection (20 mL); yellow, plane for second injection (10 mL)
A mixture of lidocaine 1% and ropivacaine 0.25% was used for the blocks; a total of 10 mL was injected between the pectoralis major and minor, and another 20 mL was injected below the pectoralis minor. Post block, the patient's position was changed to Trendelenburg position with right side up for about 15 min with continuous communication and reassurance to the patient. The patient's position was adjusted for surgical exposure, and just before skin incision the surgical area was tested for pain with surgical forceps to ensure that the patient was pain free. A skin incision was made and a lymph node on measuring 5x3x4 cm was dissected with good hemostasis and no complication. Throughout the procedure the patient’s pain score remained 0 out of 10 and her vital signs showed no changes. The surgery was done without the use of sedation or local infiltration and the patient remained pain free and fully awake throughout the procedure. Afterwards, the patient was fully awake and vitally stable, and transferred to the post-anesthesia care unit (PACU), where she was monitored for two hours. She remained hemodynamically stable with zero pain score. After monitoring for 2 hours in the PACU, the patient was transferred to the oncology ward in a stable condition.
3. DISCUSSION
In certain cases, avoiding general anesthesia could be safer and this patient had quite a few reasons why we must avoid general anesthesia if feasible. Anesthesia for awake surgeries involving the axillary area can be very challenging and requires collaborative teamwork. In addition, such cases are particularly challenging to be done with a single injection regional block, although pure local anesthesia infiltration is a well-known technique, no described regional anesthesia block or technique has been identified to be ideal or superior for such surgeries and only very few cases reported in literatures. While actually some data recommends against the use of any regional techniques due to the anatomical challenges in the axilla and no technique could reliably provide sufficient analgesia to the axillary region.1 The innervation of axillary area consists of multiple contributions from nerves and groups of nerves. The intercostobrachial nerve (ICBN), which is responsible for most of cutaneous supply of the axilla, and with contribution from the brachial plexus (BP) by providing additional cutaneous innervation from medial brachial cutaneous nerve (MBCN) and deep somatic innervation within the axilla mainly through the lateral and medial pectoral nerves.2 Other nerves arising from brachial plexus and contributing to anterolateral chest wall are the thoracodorsal nerve, and the long thoracic nerve, which innervate latissimus dorsi, and serratus anterior muscles, respectively.3 The axilla is also innervated by the other lateral cutaneous branches of the thoracic intercostal nerve (LCNs) in addition to ICBN (T2).
In addition to pure local anesthetic infiltration, such surgeries could be performed with regional techniques keeping in mind the essential coverage of ICBN, medial and lateral pectoral nerves (MPN and LPN) and LCNs. For ICBN block, there are several reliable regional blocks that could cover this nerve like; targeting ICBN itself, high thoracic paravertebral, PECS II, or serratus anterior blocks. While MPN and LPN could be blocked, if we do PECS I, PECS II (two pectoral fascial compartments) or supraclavicular BP block, the LCNs will be blocked in case of paravertebral, PECS II or serratus anterior block. In this case PECS II was done as the primary anesthesia with no sedation.3
In literature, regional block was used in few cases as the primary anesthesia for different procedures on the chest wall and axilla; e.g., breast surgery, axillary dissection, transthoracic arteriovenous graft repair and cardiovascular implantable electronic device with or without sedation. In one case report, the author described a case of axillary clearance under regional blocks (supraclavicular BP and ICBN blocks).2 In another case, breast conserving surgery with axillary dissection was done using PECS II, with sedation in form of dexmedetomidine infusion.4 While in another case PECS II was used as the sole anesthetic for removal of a large axillary tumor.5 A combination of PECS I, serratus anterior plane (SAP), and parasternal intercostal plane blocks with sedation in the form of propofol infusion was used for modified radical mastectomy and axillary lymph node dissection.6 Viewing such literature reinforces the limit of evidence, lack of guidelines, and wide discrepancy in the practice among anesthesiologists toward regional block preferences and opinions for surgeries involving the anterolateral chest wall and specifically the axilla.
In addition to the complexity of regional anesthesia for surgeries in the axillary area; fascial plane blocks, in general, are still one of the new evolving debatable topics regarding their value, reliability and effectiveness; particularly in case of PECS block, where there is much data in favor of recent development of such techniques.7 On the other hand, few studies have shown no benefits and even some showed an increase in the reported pain scores with PECS group.7 Such discrepancies might be due to these blocks being relatively recently introduced with lack of a particular end point target. In addition to the numerous factors which could affect the fascial plane blocks, Elsharkawy et al. described the basics of facial plane and how many factors could influence the effectiveness, the quality and the spread of the block.8 Site of injection, multi injectional sites, volume of local anesthesia, biomechanical properties of the fascia, types of fasciae and fascial layers; all could influence the dermatomal spread and quality of the block.8
To better understand the value of these factors, for example the site of injection in PECS II, injecting lateral to thoracoacromial branch and close to anterior axillary line for the superficial injection and injecting between the level of third and fourth rib over the anterior axillary line for the deeper one will result in more reliable block.3,9
In this case report we do not only suggest the potential of PECS block to provide a decrease in the intraoperative and postoperative opioid consumption and lower pain scores, but we also see a potential for it to be used as the primary anesthesia for selected surgeries. In addition to the factors which influence the success of facial plane block, carefully choosing which block to perform for a specific procedure is crucial to ensure a total pain free experience. For example, PECS II block is a great block in certain chest wall surgeries; however, it is a pure somatic block and doesn’t provide visceral block. For cases where visceral coverage also needed one should think of other blocks like; erector spinae plane or midpoint transverse process to pleura blocks.3
3. CONCLUSION
An efficient perioperative care of a patient starts with carful preoperative assessment and discussion with all involved medical teams, and of course the patient, to formulate the best possible plan and care. Fascial plane blocks have potential to provide not only sensory block, but surgical block too, when we understand and implement them to the right procedures and patients. In the axilla with its complex innervation, fascial plane blocks could offer a proper surgical coverage and maybe with fewer side effects and complications in high risk patients.
4. Ethical considerations
Written consent was obtained from the patient to use his pictures for the academic purpose.
5. Conflict of interests
The author declares no conflict of interests.
6. Author’s contribution
Omar Al Misnid is the sole author of this case report.
7. REFERENCES
- Jacobs A, Lemoine A, Joshi GP, Van Zundert A, Van de Velde M, Bonnet MP, et al. PROSPECT guideline for oncological breast surgery: a systematic review and procedure-specific postoperative pain management recommendations. Anaesthesia. 2020;75:664–73. PubMed DOI: 1111/anae.14964
- Munasinghe BM, Subramaniam N, Nimalan S, Sivamayuran P. Ultrasound to the rescue: axillary clearance under complete regional blockade. Case Rep Anesthesiol. 2021;2021:6655930. PubMed DOI: 1155/2021/6655930
- Chin KJ, Versyck B, Elsharkawy H, Rojas Gomez MF, Sala-Blanch X, Reina MA. Anatomical basis of fascial plane blocks. Reg Anesth Pain Med. 2021;46(7):581–99. PubMed DOI: 1136/rapm-2021-102506
- Moon EJ, Kim SB, Chung JY, Song JY, Yi JW. Pectoral nerve block (Pecs block) with sedation for breast conserving surgery without general anesthesia. Ann Surg Treat Res. 2017;93(3):166–9. PubMed DOI: 4174/astr.2017.93.3.166
- Van de Putte P, Blockmans D, De Rop C, Versyck B. Pectoral nerve block type II as the sole anesthetic for removal of a large axillary tumor: a case report. A A Pract. 2020;14(6):e01201. PubMed DOI: 1213/XAA.0000000000001201
- Bhakta P, Mac Sweeney K, O’Donnell BD. Chest wall regional anesthesia for modified radical mastectomy and axillary lymph node dissection: a case report. A A Pract. 2021;15(6):e01482. PubMed DOI: 1213/XAA.0000000000001482
- Bin Ghali K, AlKharraz N, Almisnid O, Alqarni A, Alyamani OA. The pectoral (PECS) regional block: a scoping review. Cureus. 2023;15(10):e46594. PubMed DOI: 7759/cureus.46594
- Elsharkawy H, Pawa A, Mariano ER. Interfascial plane blocks: back to basics. Reg Anesth Pain Med. 2018;43(4):341–6. PubMed DOI: 1097/AAP.0000000000000750
- Versyck B, Groen G, van Geffen GJ, Van Houwe P, Bleys RL. The pecs anesthetic blockade: a correlation between magnetic resonance imaging, ultrasound imaging, reconstructed cross-sectional anatomy and cross-sectional histology. Clin Anat. 2019;32(3):421–9. PubMed DOI: 1002/ca.23333