Ali Najih Al-awwady*
Author’s affiliation:
*Ali Najih Al-awwady, Department of Surgery, College of Medicine, Jabir ibn Hayyan University for Medical and Pharmaceutical Sciences, An-Najaf, Iraq; Email: ali.alawwdy@jmu.edu.iq
Correspondence: Ali Najih Al-awwady; E-mail: ali.alawwdy@jmu.edu.iq
Background & objective: A widespread post-operative complication that can lead to serious discomfort and morbidity is sore throat, and it is usually linked to endotracheal intubation during general anesthesia (GA). We examined and compared the effects of nebulized magnesium with nebulized ketamine on the frequency and intensity of sore throat in the first 24 hr following thyroidectomy under GA.
Methods: In this randomized clinical trial, 60 adult patients aged 18-55 years, were enrolled to receive either nebulized 50 mg ketamine, magnesium sulfate 250 mg, or normal saline. Each group consists of 20 patients, all categorized as American Society of Anesthesia I or II. The treatment was administered 15 min before the induction of anesthesia and the incidence. The severity of postoperative sore throat was evaluated, and the systolic, and diastolic blood pressure, heart rate, and blood oxygen saturation were examined. The measurement at the following time intervals of 0h, 2 hr, 4 hr, 6 hr, 8 hr, 12 hr, and 24 hr post thyroidectomy.
Result: The incidence of postoperative sore throat at 4 hr, 6 hr, 8 hr, 12 hr, and 24 hr post-surgery was significantly higher in the normal saline group compared with the ketamine or magnesium sulfate group, the overall incidence of sore throat was 75%, 24.2%, and 32.1% respectively. Patients with both ketamine and magnesium groups showed less severity of sore throat at 2 hr, 4 hr, 6 hr, 8 hr, 12 hr, and 24 hr post-surgery. No significant differences regarding the hemodynamics parameter between groups as well as per and post-nebulization.
Conclusion: Both nebulizations of either ketamine or magnesium sulfate before surgery are effective for the attenuation of postoperative sore throat one day post-thyroidectomy, with no difference between the two agents.
Abbreviations: BMI: Basal metabolic index, ETT: endotracheal tubes, GA: general anesthesia, NMDR: N-methyl D-aspartate receptors, POST: Postoperative sore throat
Keywords: Ketamine; magnesium sulfate; nebulize; sore throat; thyroidectomy
Citation: Al-awwady AN. Comparison of nebulized ketamine and magnesium sulfate for post-thyroidectomy sore throat relief. Anaesth. pain intensive care 2025;29(3):496-501. DOI: 10.35975/apic.v29i3.2776
Received: May 09, 2024; Revised: October 26, 2024; Accepted: January 01, 2025
Advanced anesthesia has increased focus on quality assurance to improve postoperative results. Consequently, reducing the severity and occurrence of anesthesia complications is important.] Postoperative sore throat (POST) is quite common after endotracheal intubation and general anesthesia (GA). It is regarded as the second most common minor side effect, besides nausea and vomiting following surgery.2 Studies show that the incidence of POST varies between 21% and 65%.3 Airway procedures, airway devices, and female sex are high-risk factors for POST.4
In most cases, it goes away at its own. However, many factors, including endotracheal intubation-induced mucosal erosion, trauma, inflammation, suctioning of the airway, low airway humidity; and in certain situations, surgical alteration of the tissue surrounding the airway, might result in POST.5 Although it is still considered a minor complication, it can lead to significant patient morbidity, dissatisfaction, and a prolonged stay in the hospital.6
There have been several pharmacological and non-pharmacological studies conducted to reduce the severity and frequency of sore throats. Smaller endotracheal tubes (ETTs), lubricating the ETTs, a gentle and careful use of airway equipment, intubating after complete relaxation, providing full oropharyngeal suction, limiting laryngoscopy attempts, minimizing minimal intracuff pressure to < 20 mmHg, and extubation after the tracheal cuff has completely deflated, are all examples of non-pharmacological techniques.7
Pharmacological treatment to reduce postoperative sore throat includes use of magnesium sulfate, ketamine nebulization, and the inhalation of steroids.8 Topical/local anti-nociceptive and anti-inflammatory medications used before induction reduce POST by preventing inflammation or nociception caused by mucosal damage.9 N-methyl D-aspartate receptors (NMDAR) are found in the peripheral nerve cells that are responsive to nociception in the airways.10 Considered anti-nociceptive, NMDAR antagonists have been studied for POST via nebulization with varying results. [8] Nebulization has a special benefit of evenly dispersing over all regions affected by instrumentation and mucosal injury. NMDAR antagonists with anti-inflammatory properties that are readily available include magnesium and ketamine.11
This study assessed the effectiveness of perioperative nebulized magnesium sulfate vs. ketamine to reduce the incidence of POST after thyroidectomy.
A single-blind randomized controlled trial was conducted at Al-Sader Teaching Hospital, Najaf. The study included 60 patients, ASA physical status I and II, 18-55 years old, both genders, with BMI 22-30 kg/m2, from the first February to 30th August, scheduled for elective thyroidectomy under GA. Patients with a history of per-operative sore throat, predicted difficult intubation, suffering from common cold or chronic airway disease, on non-steroidal anti-inflammatory drugs, and patients allergic to study drugs were excluded. A written consent was obtained from each patient before starting anesthesia.
Patients were randomly divided into three groups, the N Group (control group) received 2.5 mL of normal saline; the K Group received 50 mg (2.5 mL) of ketamine, and the M Group received 250 mg (2.5 mL) of magnesium sulfate. All these medications were nebulized through a nebulizer mask over 15 min while the patients spontaneously breathed before starting anesthesia, baseline hemodynamic variables were recorded such as systolic, diastolic blood pressure, heart rate, and blood oxygen saturation, and then the patients were transferred to the operating room. Classical GA was given and at the end of the surgery, throat suctioning was done, ETT cuff was deflated and the patients extubated, and transferred to the recovery room for monitoring.
The incidence and severity of sore throat were assessed at 0 hr, 2 hr, 4 hr, 6 hr, 8 hr, 12 hr, and 24 hr after extubation according to the following score (0-3):
Statistical analysis
The frequency of POST within 24 hours after extubation was our primary outcome. Our secondary outcomes were hemodynamic status and the severity of POST at 0, 2, 4, 6, 8, 12, and 24 hours. IBM SPSS version 26 (Chicago, IL., USA) was used for statistical analysis. While the chi-square test was used to analyze categorical variables, the independent t-test and one-way analysis of variance (ANOVA) were used to look for associations for continuous variables. For counts less than five, Fisher exact was utilized. A significance level of P < 0.05 was established.
Ethical considerations
The research was done following the national and international ethical standards of conducting medical research and permission was sought from the regional ethical committee. Patients’ personal information was removed and disguised from the study among other precautions to maintain the patient's privacy.
Sixty patients were involved in the study, 21 males and 39 females, the mean age was between 40.75 and 47.65 years old and the mean body mass index was between 24.5-26.2 kg/m2, 39 patients were classified as ASA class I and 21 of them were II. The mean duration of surgery was 59.35 to 71.25 min, and the mean duration of anesthesia was 89.3 to 101.25 min. Mean age, sex, BMI, ASA, D1, and D2 were insignificant among the three study groups, with a P > 0.05 (Table 1).
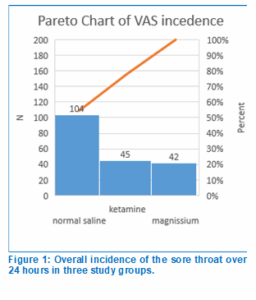
The majority of the time, both the K and the M groups showed a decrease in the incidence of POST as compared with the N group (P < 0.05). However, there were insignificant differences at zero time between the N and K groups, as well as at 2 hr between the N and K groups or the N and M groups (P > 0.05). None of the patients in the K group complained of sore throat 24 hr postoperatively. The incidence of POST between the K and M groups was insignificant (P > 0.05), as shown in Table 2. Figure 1 shows the overall incidence of POST in all three groups; 54.5% in Group N, 23.6% in Group K, and 22% in Group M.
At the initial measurement (0 hr), one patient in the N group developed a severe sore throat, but none in the K or M groups; 6 patients developed moderate sore throat in the N group, 3 in group K, and 1 in group M. While at the 2-hr mark, another one patient in the N group developed severe sore throat, and 4 patients had moderate pain but no significance was observed (P > 0.05). At 4, 6, 8, 12, and 24 hr, both K and M groups didn’t have a severe sore throat, while during 12 hr, and 24 hr both of them had a moderate sore throat. patients who suffer from mild sore throats were also lower in the Group K and M compared with the Group N with a P < 0.05 (Table 3).
The mean systolic blood pressure (SBP) during pre-nebulization (baseline) was 128.05 ± 12.96 in Group N, 136.1 ± 13.91 in Group K, and 132.75 ± 11.63 in Group M with insignificant differences between the study groups, post-nebulization at 0, 2, 4, 6, 8, 12, and 24 hr, the SBP showed no significant differences among the three study groups (P > 0.05).
The mean diastolic blood pressure (DBP) during pre-nebulization (baseline) was 79.7 ± 8.392 in Group N, 79.9 ± 9.447 in Group K, and 82.25 ± 8.347 in Group M with insignificant differences between the study groups; post-nebulization at 0, 2, 4, 6, 8, 12, and 24 hr, the DBP showed no significant differences among the three study groups (P > 0.05).
The mean heart rate (HR) during pre-nebulization (baseline) was 79.55 ± 8.562 in Group N, 83.45 ± 9.128 in Group K, and 83.95 ± 11.1 in Group M with insignificant differences between the study groups; post-nebulization at 0, 2, 4, 6, 8, 12, and 24 hr, HR showed no significant differences among the three study groups (P > 0.05).
The mean oxygen saturation (SpO2) during pre-nebulization (baseline) was 98.8 ± 0.523% in Group N, 98.95 ± 1.191% in Group K, and 98.8 ± 0.523% in Group M with insignificant differences between the study groups; post-nebulization at 0, 2, 4, 6, 8, 12, and 24 hr, the SpO2 showed no significant differences among the three study groups with a P > 0.05 (Table 4).
A usual complaint following GA is sore throat. It has been noted that there is a higher frequency of POST after thyroid surgery; this issue could be caused by vocal cord hematoma, laryngeal edema, local mucosal trauma, bilateral vocal cord palsy or vocal cord paralysis.12-13
The primary result of this study is that nebulized magnesium or ketamine administered preemptively can reduce the incidence and severity of POST within the first 24 hours after thyroidectomy under GA. The anti-nociceptive and anti-inflammatory characteristics of NMDAR antagonists are proposed as the mechanism for the diminution of sore throat.14
POST usually happens after a stressful event triggered by inflammation produced by mucosal injury.15 Upon mucosal damage or when pharyngeal muscles are stretched by equipment, excitatory amino acids like glutamate and inflammatory mediators flow out.16 Administration of either ketamine or magnesium prevents glutamate-mediated central sensitization and sensation of postoperative sore throat.17
In the current study, magnesium, and ketamine significantly reduced the incidence of POST at 4, 8, 12, and 24 hr post-surgery compared with normal saline, which aligns with the study reported by Orji et al.20 The highest possible POST incidence among the three groups was recorded at 2 hr, consistent with the incidence reported in a related research,19 which may be attributed to a high level of inflammatory mediator release or noxious stimuli. In our study, no patients in the study groups experienced significant postoperative symptoms during the trial. However, between 2- and 6 hr post-surgery, there was an increase in the Group M, possibly due to gradually developing inflammation that goes unnoticed initially and these results align with the results reported by Yadav et al.18
The resolution of inflammation and diminished nociception may be the cause of the decline in both severity and incidence in all groups from the 8 hr to the 24-hour timeframe. A reduction in severe POST in the control group by 12 hours and more supports this hypothesis. At 24 hours, the control group experienced an incidence of 50%, while 0% in the Group K and 10% in the Group M experienced POST, indicating the effect.
As the suggested method involves local anti-inflammatory and anti-nociceptive effects, their impact should gradually be minimized by ongoing
absorption from the mucosal surface. The varying effects of the two NMDAR antagonists at different times may potentially be explained by their degree of absorption. The incidence of NMDAR antagonism and POST is reported to decrease during 24 hours with several randomized controlled trials.1,15
On the contrary, significant rates of POST have been reported in clinical investigations carried out 24 hours after anesthesia.23
The study reported by Segaran et al.8 and Jain et al.22 reports that the nebulization of magnesium sulfate significantly reduces the severity and incidence of a POST when compared with the ketamine, which is in confidence with the results of our reported study.
The hemodynamic parameters such as SBP, DBP, HR, and SpO2 showed insignificant differences between groups as well as pre-and post-nebulization, this finding is same as reported by Rajan et al.,21 but not with the study reported by Segaran et al.,8 who presented that hemodynamics parameter increase in ketamine group after nebulization, which might be due to systemic absorption.
We conclude the overall incidence of sore throat in the current study within 24 hours was 54.5% for normal saline, 23.6% for ketamine, and 22% for magnesium sulfate. Additionally, we found that nebulization of both ketamine and magnesium sulfate before induction is effective in the prevention of early and late postoperative sore throat.
Testing different doses of either ketamine or magnesium sulfate for attenuation of postoperative sore throat is suggested with an increased sample size.
6. Data availability
The numerical data generated during this research is available with the authors.
7. Ethical considerations
The study followed the guidelines laid down by COPE. Ethical approval was obtained from the ethics committee of Jabir ibn Hayyan University for Medical and Pharmaceutical Sciences, An-Najaf.
8. Conflict of interest
All authors declare that there was no conflict of interest.
9. Funding
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Authors’ contribution
Ali Najih Al-awwady was the sole investigator and the author of this manuscript.
Author’s affiliation:
*Ali Najih Al-awwady, Department of Surgery, College of Medicine, Jabir ibn Hayyan University for Medical and Pharmaceutical Sciences, An-Najaf, Iraq; Email: ali.alawwdy@jmu.edu.iq
Correspondence: Ali Najih Al-awwady; E-mail: ali.alawwdy@jmu.edu.iq
ABSTRACT
Background & objective: A widespread post-operative complication that can lead to serious discomfort and morbidity is sore throat, and it is usually linked to endotracheal intubation during general anesthesia (GA). We examined and compared the effects of nebulized magnesium with nebulized ketamine on the frequency and intensity of sore throat in the first 24 hr following thyroidectomy under GA.
Methods: In this randomized clinical trial, 60 adult patients aged 18-55 years, were enrolled to receive either nebulized 50 mg ketamine, magnesium sulfate 250 mg, or normal saline. Each group consists of 20 patients, all categorized as American Society of Anesthesia I or II. The treatment was administered 15 min before the induction of anesthesia and the incidence. The severity of postoperative sore throat was evaluated, and the systolic, and diastolic blood pressure, heart rate, and blood oxygen saturation were examined. The measurement at the following time intervals of 0h, 2 hr, 4 hr, 6 hr, 8 hr, 12 hr, and 24 hr post thyroidectomy.
Result: The incidence of postoperative sore throat at 4 hr, 6 hr, 8 hr, 12 hr, and 24 hr post-surgery was significantly higher in the normal saline group compared with the ketamine or magnesium sulfate group, the overall incidence of sore throat was 75%, 24.2%, and 32.1% respectively. Patients with both ketamine and magnesium groups showed less severity of sore throat at 2 hr, 4 hr, 6 hr, 8 hr, 12 hr, and 24 hr post-surgery. No significant differences regarding the hemodynamics parameter between groups as well as per and post-nebulization.
Conclusion: Both nebulizations of either ketamine or magnesium sulfate before surgery are effective for the attenuation of postoperative sore throat one day post-thyroidectomy, with no difference between the two agents.
Abbreviations: BMI: Basal metabolic index, ETT: endotracheal tubes, GA: general anesthesia, NMDR: N-methyl D-aspartate receptors, POST: Postoperative sore throat
Keywords: Ketamine; magnesium sulfate; nebulize; sore throat; thyroidectomy
Citation: Al-awwady AN. Comparison of nebulized ketamine and magnesium sulfate for post-thyroidectomy sore throat relief. Anaesth. pain intensive care 2025;29(3):496-501. DOI: 10.35975/apic.v29i3.2776
Received: May 09, 2024; Revised: October 26, 2024; Accepted: January 01, 2025
1. INTRODUCTION
Advanced anesthesia has increased focus on quality assurance to improve postoperative results. Consequently, reducing the severity and occurrence of anesthesia complications is important.] Postoperative sore throat (POST) is quite common after endotracheal intubation and general anesthesia (GA). It is regarded as the second most common minor side effect, besides nausea and vomiting following surgery.2 Studies show that the incidence of POST varies between 21% and 65%.3 Airway procedures, airway devices, and female sex are high-risk factors for POST.4
In most cases, it goes away at its own. However, many factors, including endotracheal intubation-induced mucosal erosion, trauma, inflammation, suctioning of the airway, low airway humidity; and in certain situations, surgical alteration of the tissue surrounding the airway, might result in POST.5 Although it is still considered a minor complication, it can lead to significant patient morbidity, dissatisfaction, and a prolonged stay in the hospital.6
There have been several pharmacological and non-pharmacological studies conducted to reduce the severity and frequency of sore throats. Smaller endotracheal tubes (ETTs), lubricating the ETTs, a gentle and careful use of airway equipment, intubating after complete relaxation, providing full oropharyngeal suction, limiting laryngoscopy attempts, minimizing minimal intracuff pressure to < 20 mmHg, and extubation after the tracheal cuff has completely deflated, are all examples of non-pharmacological techniques.7
Pharmacological treatment to reduce postoperative sore throat includes use of magnesium sulfate, ketamine nebulization, and the inhalation of steroids.8 Topical/local anti-nociceptive and anti-inflammatory medications used before induction reduce POST by preventing inflammation or nociception caused by mucosal damage.9 N-methyl D-aspartate receptors (NMDAR) are found in the peripheral nerve cells that are responsive to nociception in the airways.10 Considered anti-nociceptive, NMDAR antagonists have been studied for POST via nebulization with varying results. [8] Nebulization has a special benefit of evenly dispersing over all regions affected by instrumentation and mucosal injury. NMDAR antagonists with anti-inflammatory properties that are readily available include magnesium and ketamine.11
This study assessed the effectiveness of perioperative nebulized magnesium sulfate vs. ketamine to reduce the incidence of POST after thyroidectomy.
2. METHODOLOGY
A single-blind randomized controlled trial was conducted at Al-Sader Teaching Hospital, Najaf. The study included 60 patients, ASA physical status I and II, 18-55 years old, both genders, with BMI 22-30 kg/m2, from the first February to 30th August, scheduled for elective thyroidectomy under GA. Patients with a history of per-operative sore throat, predicted difficult intubation, suffering from common cold or chronic airway disease, on non-steroidal anti-inflammatory drugs, and patients allergic to study drugs were excluded. A written consent was obtained from each patient before starting anesthesia.
Patients were randomly divided into three groups, the N Group (control group) received 2.5 mL of normal saline; the K Group received 50 mg (2.5 mL) of ketamine, and the M Group received 250 mg (2.5 mL) of magnesium sulfate. All these medications were nebulized through a nebulizer mask over 15 min while the patients spontaneously breathed before starting anesthesia, baseline hemodynamic variables were recorded such as systolic, diastolic blood pressure, heart rate, and blood oxygen saturation, and then the patients were transferred to the operating room. Classical GA was given and at the end of the surgery, throat suctioning was done, ETT cuff was deflated and the patients extubated, and transferred to the recovery room for monitoring.
The incidence and severity of sore throat were assessed at 0 hr, 2 hr, 4 hr, 6 hr, 8 hr, 12 hr, and 24 hr after extubation according to the following score (0-3):
- 0 = without a sore throat.
- 1 = minimal sore throat (only by asking).
- 2 = moderate sore throat (complains of sore throat without asking).
- 3 = severe sore throat (might be voice change or hoarseness of voice with pain).
Statistical analysis
The frequency of POST within 24 hours after extubation was our primary outcome. Our secondary outcomes were hemodynamic status and the severity of POST at 0, 2, 4, 6, 8, 12, and 24 hours. IBM SPSS version 26 (Chicago, IL., USA) was used for statistical analysis. While the chi-square test was used to analyze categorical variables, the independent t-test and one-way analysis of variance (ANOVA) were used to look for associations for continuous variables. For counts less than five, Fisher exact was utilized. A significance level of P < 0.05 was established.
Ethical considerations
The research was done following the national and international ethical standards of conducting medical research and permission was sought from the regional ethical committee. Patients’ personal information was removed and disguised from the study among other precautions to maintain the patient's privacy.
3. RESULTS
Sixty patients were involved in the study, 21 males and 39 females, the mean age was between 40.75 and 47.65 years old and the mean body mass index was between 24.5-26.2 kg/m2, 39 patients were classified as ASA class I and 21 of them were II. The mean duration of surgery was 59.35 to 71.25 min, and the mean duration of anesthesia was 89.3 to 101.25 min. Mean age, sex, BMI, ASA, D1, and D2 were insignificant among the three study groups, with a P > 0.05 (Table 1).
| Table 1: Demographics data. | ||||
| Characteristics | Group N | Group K | Group M | p-value |
| Gender M/F | 8/12 | 5/15 | 8/12 | 0.517 |
| Age (Yr) | 45.85 ± 9.7 | 40.75 ± 7.5 | 47.65 ± 7.52 | 0.032 |
| BMI (kg/m2) | 24.5 ± 2.27 | 24.7 ± 1.98 | 26.2 ± 2.29 | 0.032 |
| D1 | 59.35 ± 12.17 | 71.25 ± 19.25 | 63.05 ± 14.05 | 0.058 |
| D2 | 89.3 ± 12.37 | 101.25 ± 18.97 | 92.8 ± 14.51 | 0.054 |
| ASA I/II | 14/6 | 12/8 | 13/7 | 0.803 |
| Data presented as numbers; P < 0.05 considered significant
BMI: body mass index, D1: duration of surgery, D2: duration of anesthesia. |
||||
The majority of the time, both the K and the M groups showed a decrease in the incidence of POST as compared with the N group (P < 0.05). However, there were insignificant differences at zero time between the N and K groups, as well as at 2 hr between the N and K groups or the N and M groups (P > 0.05). None of the patients in the K group complained of sore throat 24 hr postoperatively. The incidence of POST between the K and M groups was insignificant (P > 0.05), as shown in Table 2. Figure 1 shows the overall incidence of POST in all three groups; 54.5% in Group N, 23.6% in Group K, and 22% in Group M.
| Table 2: Incidence of sore throat among the three study groups at different time intervals. | ||||||
| Times | Group N
n (%) |
Group K
n (%) |
Group M
n (%) |
P-value | ||
| N and K | Nand M | K and M | ||||
| Zero | 14 (70) | 10 (50) | 5 (25) | 0.414 | 0.029 | 0.064 |
| 2 hr | 18 (90) | 12 (60) | 12 (60) | 0.545 | 0.545 | - |
| 4 hr | 19 (95) | 9 (45) | 8 (40) | 0.040 | 0.045 | 0.865 |
| 6 hr | 18 (90) | 6 (30) | 8 (40) | 0.024 | 0.043 | 0.830 |
| 8 hr | 13 (65) | 4 (20) | 5 (25) | 0.020 | 0.038 | 0.883 |
| 12 hr | 13 (65) | 1 (5) | 5 (25) | 0.012 | 0.038 | 0.063 |
| 24 hr | 10 (50) | 0 (0) | 2 (10) | <0.001 | 0.009 | 0.136 |
| Data presented as n (%); P < 0.05 considered significant | ||||||
At the initial measurement (0 hr), one patient in the N group developed a severe sore throat, but none in the K or M groups; 6 patients developed moderate sore throat in the N group, 3 in group K, and 1 in group M. While at the 2-hr mark, another one patient in the N group developed severe sore throat, and 4 patients had moderate pain but no significance was observed (P > 0.05). At 4, 6, 8, 12, and 24 hr, both K and M groups didn’t have a severe sore throat, while during 12 hr, and 24 hr both of them had a moderate sore throat. patients who suffer from mild sore throats were also lower in the Group K and M compared with the Group N with a P < 0.05 (Table 3).
| Table 3: Severity of sore throat at different time intervals among three study groups | |||||||
| Time | Severity grade | Group N | Group K | Group M | P-value | ||
| N and K | N and M | K and M | |||||
| 0 hr | 0 1 2 3 |
6 7 6 1 |
10 7 3 0 |
15 4 1 0 |
0.577 | 0.041 | 0.420 |
| 2 hr | 0 1 2 3 |
2 13 4 1 |
8 10 2 0 |
8 11 1 0 |
0.200 | 0.135 | 0.944 |
| 4 hr | 0 1 2 3 |
2 10 7 1 |
11 8 1 0 |
12 3 4 1 |
0.012 | 0.008 | 0.251 |
| 6 hr | 0 1 2 3 |
2 8 6 4 |
14 4 2 0 |
12 4 4 0 |
0.002 | 0.013 | 0.844 |
| 8 hr | 0 1 2 3 |
7 4 3 6 |
16 4 0 0 |
15 4 1 0 |
0.045 | 0.058 | 0.999 |
| 12 hr | 0 1 2 3 |
7 5 5 3 |
19 1 0 0 |
15 5 0 0 |
0.008 | 0.089 | 0.370 |
| 24 hr | 0 1 2 3 |
10 8 2 0 |
20 0 0 0 |
18 2 0 0 |
0.010 | 0.045 | 0.812 |
| Data presented as numbers; P < 0.05 considered significant | |||||||
The mean systolic blood pressure (SBP) during pre-nebulization (baseline) was 128.05 ± 12.96 in Group N, 136.1 ± 13.91 in Group K, and 132.75 ± 11.63 in Group M with insignificant differences between the study groups, post-nebulization at 0, 2, 4, 6, 8, 12, and 24 hr, the SBP showed no significant differences among the three study groups (P > 0.05).
The mean diastolic blood pressure (DBP) during pre-nebulization (baseline) was 79.7 ± 8.392 in Group N, 79.9 ± 9.447 in Group K, and 82.25 ± 8.347 in Group M with insignificant differences between the study groups; post-nebulization at 0, 2, 4, 6, 8, 12, and 24 hr, the DBP showed no significant differences among the three study groups (P > 0.05).
The mean heart rate (HR) during pre-nebulization (baseline) was 79.55 ± 8.562 in Group N, 83.45 ± 9.128 in Group K, and 83.95 ± 11.1 in Group M with insignificant differences between the study groups; post-nebulization at 0, 2, 4, 6, 8, 12, and 24 hr, HR showed no significant differences among the three study groups (P > 0.05).
The mean oxygen saturation (SpO2) during pre-nebulization (baseline) was 98.8 ± 0.523% in Group N, 98.95 ± 1.191% in Group K, and 98.8 ± 0.523% in Group M with insignificant differences between the study groups; post-nebulization at 0, 2, 4, 6, 8, 12, and 24 hr, the SpO2 showed no significant differences among the three study groups with a P > 0.05 (Table 4).
| Table 4: Comparison of study groups according to SpO2 over 24 hr. | ||||
| Time | Group N | Group K | Group M | P.value |
| Baseline | 98.8 ± 0.523 | 98.95 ± 1.191 | 98.8 ± 0.523 | 0.796 |
| 0 time | 98.45 ± 0.605 | 98.45 ± 0.887 | 98.7 ± 0.571 | 0.435 |
| 2 hr | 98.25 ± 0.716 | 98.4 ± 0.754 | 98.35 ± 0.671 | 0.796 |
| 4 hr | 98.5 ± 0.761 | 98.5 ± 0.688 | 98.2 ± 0.768 | 0.341 |
| 6 hr | 98.6 ± 0.598 | 98.1 ± 1.071 | 98.15 ± 0.745 | 0.119 |
| 8 hr | 98.6 ± 0.598 | 98.1 ± 98.2 | 0.759 ± 0.759 | 0.088 |
| 12 hr | 98.8 ± 0.523 | 98.2 ± 0.834 | 98.6 ± 0.681 | 0.056 |
| 24 hr | 98.75 ± 0.444 | 98.6 ± 0.681 | 98.5 ± 0.761 | 0.469 |
| Data presented as mean ± SD; P < 0.05 considered significant | ||||
4. DISCUSSION
A usual complaint following GA is sore throat. It has been noted that there is a higher frequency of POST after thyroid surgery; this issue could be caused by vocal cord hematoma, laryngeal edema, local mucosal trauma, bilateral vocal cord palsy or vocal cord paralysis.12-13
The primary result of this study is that nebulized magnesium or ketamine administered preemptively can reduce the incidence and severity of POST within the first 24 hours after thyroidectomy under GA. The anti-nociceptive and anti-inflammatory characteristics of NMDAR antagonists are proposed as the mechanism for the diminution of sore throat.14
POST usually happens after a stressful event triggered by inflammation produced by mucosal injury.15 Upon mucosal damage or when pharyngeal muscles are stretched by equipment, excitatory amino acids like glutamate and inflammatory mediators flow out.16 Administration of either ketamine or magnesium prevents glutamate-mediated central sensitization and sensation of postoperative sore throat.17
In the current study, magnesium, and ketamine significantly reduced the incidence of POST at 4, 8, 12, and 24 hr post-surgery compared with normal saline, which aligns with the study reported by Orji et al.20 The highest possible POST incidence among the three groups was recorded at 2 hr, consistent with the incidence reported in a related research,19 which may be attributed to a high level of inflammatory mediator release or noxious stimuli. In our study, no patients in the study groups experienced significant postoperative symptoms during the trial. However, between 2- and 6 hr post-surgery, there was an increase in the Group M, possibly due to gradually developing inflammation that goes unnoticed initially and these results align with the results reported by Yadav et al.18
The resolution of inflammation and diminished nociception may be the cause of the decline in both severity and incidence in all groups from the 8 hr to the 24-hour timeframe. A reduction in severe POST in the control group by 12 hours and more supports this hypothesis. At 24 hours, the control group experienced an incidence of 50%, while 0% in the Group K and 10% in the Group M experienced POST, indicating the effect.
As the suggested method involves local anti-inflammatory and anti-nociceptive effects, their impact should gradually be minimized by ongoing
absorption from the mucosal surface. The varying effects of the two NMDAR antagonists at different times may potentially be explained by their degree of absorption. The incidence of NMDAR antagonism and POST is reported to decrease during 24 hours with several randomized controlled trials.1,15
On the contrary, significant rates of POST have been reported in clinical investigations carried out 24 hours after anesthesia.23
The study reported by Segaran et al.8 and Jain et al.22 reports that the nebulization of magnesium sulfate significantly reduces the severity and incidence of a POST when compared with the ketamine, which is in confidence with the results of our reported study.
The hemodynamic parameters such as SBP, DBP, HR, and SpO2 showed insignificant differences between groups as well as pre-and post-nebulization, this finding is same as reported by Rajan et al.,21 but not with the study reported by Segaran et al.,8 who presented that hemodynamics parameter increase in ketamine group after nebulization, which might be due to systemic absorption.
5. CONCLUSION
We conclude the overall incidence of sore throat in the current study within 24 hours was 54.5% for normal saline, 23.6% for ketamine, and 22% for magnesium sulfate. Additionally, we found that nebulization of both ketamine and magnesium sulfate before induction is effective in the prevention of early and late postoperative sore throat.
Testing different doses of either ketamine or magnesium sulfate for attenuation of postoperative sore throat is suggested with an increased sample size.
6. Data availability
The numerical data generated during this research is available with the authors.
7. Ethical considerations
The study followed the guidelines laid down by COPE. Ethical approval was obtained from the ethics committee of Jabir ibn Hayyan University for Medical and Pharmaceutical Sciences, An-Najaf.
8. Conflict of interest
All authors declare that there was no conflict of interest.
9. Funding
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Authors’ contribution
Ali Najih Al-awwady was the sole investigator and the author of this manuscript.
11. REFERENCES
- Mohamed Rizk MA, Moustafa ZA, Kamal KY, Salah AM. Comparative study between preoperative nebulization with magnesium sulfate and ketamine in the prevention of postoperative sore throat during general anesthesia with endotracheal intubation in adults: a randomized double-blinded clinical trial. QJM. 2024;117(Suppl_2):hcae175.072. DOI: 1093/qjmed/hcae175.072
- Chattopadhyay S, Das A, Nandy S, RoyBasunia S. Postoperative sore throat prevention in ambulatory surgery: a comparison between preoperative aspirin and magnesium sulfate gargle—a prospective, randomized, double-blind study. Anesth Essays Res. 2017;11(1):94-100. PubMed DOI: 4103/0259-1162.186602
- Lee SH, Lee YC, Lee JH, Choi SR, Lee SC. The prophylactic effect of dexamethasone on postoperative sore throat in prone position surgery. Korean J Anesthesiol. 2016;69(3):255-61. PubMed DOI: 4097/kjae.2016.69.3.255
- Patel N, Dhuliya S, Shah D. Comparative evaluation of the incidence of postoperative sore throat after nebulization with ketamine and magnesium sulfate in patients undergoing general anesthesia requiring endotracheal intubation. Indian J Clin Anaesth. 2022;9(2):227-32. DOI: 18231/j.ijca.2022.045
- Kuriyama A, Nakanishi M, Kamei J, Sun R, Ninomiya K, Hino M. Topical application of ketamine to prevent postoperative sore throat in adults: a systematic review and meta-analysis. Acta Anaesthesiol Scand. 2020;64(5):579-91. PubMed DOI: 1111/aas.13553
- Puthenveettil N, Kishore K, Paul J. Effect of cuff pressures on postoperative sore throat in gynecologic laparoscopic surgery: an observational study. Anesth Essays Res. 2018;12(2):484-8. PubMed DOI: 4103/aer.AER_72_18
- Canbay O, Celebi N, Sahin A, Celiker V, Ozgen S, Aypar U. Ketamine gargle for attenuating postoperative sore throat. Br J Anaesth. 2008;100(4):490-3. PubMed DOI: 1093/bja/aen023
- Segaran S, Bacthavasalame AT, Venkatesh RR, Zachariah M, George SK, Kandasamy R. Comparison of nebulized ketamine with nebulized magnesium sulfate on the incidence of postoperative sore throat. Anesth Essays Res. 2018;12(4):885-90. PubMed DOI: 4103/aer.AER_148_18
- Jiang Y, Chen R, Xu S, Li J, Yu F, Kong L, et al. The impact of prophylactic dexamethasone on postoperative sore throat: an updated systematic review and meta-analysis. J Pain Res. 2018;11:2463-75. PubMed DOI: 2147/JPR.S172419
- Balentine CJ, Sippel RS. Outpatient thyroidectomy: is it safe? Surg Oncol Clin N Am. 2016;25(1):61-75. PubMed DOI: 1016/j.soc.2015.08.003
- Roman BR, Randolph GW, Kamani D. Conventional thyroidectomy in the treatment of primary thyroid cancer. Endocrinol Metab Clin North Am. 2019;48(1):125-41. PubMed DOI: 1016/j.ecl.2018.11.003
- Shekhar S, Gupta A, Gunjan, Gupta S, Singh K. Comparison of nebulized ketamine and ketamine with clonidine in postoperative sore throat. Anesth Essays Res. 2019;13(2):313-6. PubMed DOI: 4103/aer.AER_19_19
- Gong Y, Xu X, Wang J, Che L, Wang W, Yi J. Laryngeal mask airway reduces the incidence of postoperative sore throat after thyroid surgery compared with endotracheal tube: a single-blinded randomized controlled trial. BMC Anesthesiol. 2020;20(1):16. PubMed DOI: 1186/s12871-020-0932-2
- Khan KS, Bhardwaj S, Chaturvedi A. Magnesium: its role in anesthesia. J Anaesthesiol Clin Pharmacol. 2017;33(4):486-92.
- Borazan H, Kececioglu A, Okesli S, Otelcioglu S. Oral magnesium lozenge reduces postoperative sore throat: a randomized, prospective, placebo-controlled study. Anesthesiology. 2012;117:512-8. PubMed DOI: 1097/ALN.0b013e3182639d5f
- Puyo CA, Dahms TE. Innate immunity mediating inflammation secondary to endotracheal intubation. Arch Otolaryngol Head Neck Surg. 2012;138:854-8. PubMed DOI: 1001/archoto.2012.1746
- Rudra A, Ray S, Chatterjee S, et al. Gargling with ketamine attenuates the postoperative sore throat. Indian J Anaesth. 2009;53:40-3. PubMed
- Yadav M, Chalumuru N, Gopinath R. Effect of magnesium sulfate nebulization on the incidence of postoperative sore throat. J Anaesthesiol Clin Pharmacol. 2016;32:168-71. PubMed DOI: 4103/0970-9185.173367
- Kajal K, Dharmu D, Bhukkal I, Yaddanapudi S, Soni SL, Kumar M, et al. Comparison of three different methods of attenuating postoperative sore throat, cough, and hoarseness of voice in patients undergoing tracheal intubation. Anesth Essays Res. 2019;13(3):572-6. PubMed DOI: 4103/aer.AER_61_19
- Orji MO, Osinaike BB, Amanor-Boadu SD. Nebulized magnesium versus ketamine for prevention of postoperative sore throat in patients for general anesthesia. Ann Ibadan Postgrad Med. 2020;18(1):3-8. PubMed
- Rajan S, Malayil GJ, Varghese R, Kumar L. Comparison of the usefulness of ketamine and magnesium sulfate nebulizations for attenuating postoperative sore throat, hoarseness of voice, and cough. Anesth Essays Res. 2017;11(2):287-93. PubMed DOI: 4103/0259-1162.181427
- Jain S, Barasker SK. A comparative study of preoperative ketamine and MgSO4 nebulization for incidence of postoperative sore throat after endotracheal intubation. Int J Contemp Med Res. 2017;4:1356-9. Full Text
- Fenta E, Teshome D, Melaku D, et al. Incidence and factors associated with a postoperative sore throat for patients undergoing surgery under general anesthesia with endotracheal intubation at Debre Tabor General Hospital, Northcentral Ethiopia: a cross-sectional study. Int J Surg Open. 2020;25:1-5. DOI: 1016/j.ijso.2020.06.003