Citra Tanoto1, Charles2, Tjokorda Gde Agung Senapathi3, I Gusti Agung Gede Utara Hartawan4
Author affiliations:
Parotid abscess originates from an ascending infection of the parotid gland through Stensen’s duct, which progresses into formation of pus. Infections involving the oral or neck structure may obscure the vocal cords and complicate the tracheal intubation with direct laryngoscopy. We present a case of 44-year-old male patient presented with painful swelling of the left cheek extending into the temporal region for four days. His physical examination revealed erythematous swelling of the left cheek that limited the patient’s mouth opening. He was diagnosed with left-sided parotid abscess and surgical drainage was planned. The hyoid-mental and thyrohyoid distances were decreased, which indicated that the patient’s airway might be difficult to visualize with direct laryngoscopy. We decided to choose awake intubation with flexible intubation scope for tracheal tube placement. The procedure went smoothly without any complication and the patient’s condition was stable throughout 18 days of care in the intermediate ward. The current gold standard management of anticipated difficult airway is awake tracheal intubation (ATI) and the American Society of Anesthesiologists recommended the use of non-invasive airway management devices, including flexible intubation scope. This procedure is preferred due to its low risk of complications and high success rates.
Keywords: Awake tracheal intubation; Awake fibreoptic intubation; Difficult airway; Flexible intubation scope; Parotid abscess
Citation: Tanoto C, Charles, Senapathi TGA, Utara Hartawan IGAG. Awake intubation with intubation fiberscope in a patient with difficult intubation and difficult ventilation: a case report. Anaesth. pain intensive care 2025;29(3):699-702. DOI: 10.35975/apic.v29i3.2768
Received: May 09, 2024; Revised: October 26, 2024; Accepted: January 01, 2025
Parotid abscess is usually preceded by ascending infection into the parotid gland through Stensen’s duct. The incidence of this condition is quite low, and it mostly affects immunocompromised population, such as infants and elderly. The most common pathogens that cause parotid abscess are aerobic bacteria, including Staphylococcus aureus, Hemophilus influenzae, and Streptococcus pneumoniae. Poor oral cavity hygiene or dental infection are some of the predisposing factors of parotid infection. The infected intra-parotid and periparotid lymph nodes may cause pus formation and lead to abscess formation. If abscess formation persists, pus will enter the capsule and infiltrate the surrounding tissue and spread into the skin, external auditory canal or deep cervical fascial. Parotid abscess that extends to the head and neck
structures can cause airway obstruction which is potentially life-threatening.1,2
Tracheal intubation assisted by direct laryngoscopy following induction is the standard anesthetic procedure in most of these cases. However, patients with difficult airway, where visualizing the vocal cords might be difficult, is in higher risk of unsuccessful tracheal intubation with conventional laryngoscopy. Therefore, awake intubation is preferred as an alternative tracheal tube placement.3 Here we present a patient with difficult airway due to left-sided parotid abscess and awake intubation with Flexible Intubation Scope (FIS) was indicated.
A 44-year-old male patient with left-sided parotid abscess and orbital cellulitis presented with painful swelling of the left cheek extending into the temporal for four days. The patient also experienced difficulty in eating and drinking due to the painful swelling of the left cheek. Other complaints, such as fever, cough or shortness of breath, were denied. The patient had medical history of type 2 diabetes mellitus for 10 years and was currently on insulin treatment. The patient also had history of hypertension for 2 years and taking amlodipine regularly. Vital signs were within normal limits.
Anthropometric assessment found body weight 60 kg, height 175 cm and BMI 19.5 kg/m2. Physical examination of the head showed erythematous swelling of the left cheek (±7x8 cm) extending into the temporal and orbital region, warmth and fluctuant on palpation (Figure 1).

Figure 1: Physical examination showed erythematous swelling of the left cheek (±7x8 cm) extending into the temporal and orbital region.
Mouth opening was limited, the hyomental distance was more than three finger-breadths, and the thyrohyoid distance was more than two finger-breadths. The patient’s Mallampati class was too difficult to assess. Neck CT-scan with contrast revealed well-defined hypodense lesion with fluid density suggesting abscess in the left masticator space extending to the left ofacial, left pre-septal space, left parotid space, left submandibular and sublingual spaces, and left parapharyngeal space (Figure 2).
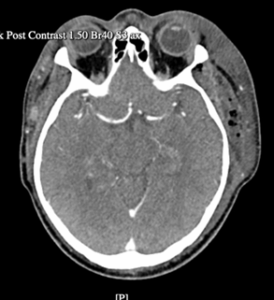
Figure 2: Neck CT-scan with contrast revealed well-defined hypodense lesion with fluid density suggesting abscess in the left masticator space extending to the left fronto-temporo-parietal region of the scalp.
Laboratory findings were unremarkable. We concluded the patient with ASA physical status III. The patient was scheduled for abscess drainage under general anesthesia with awake intubation using flexible intubation scope (FIS).fronto-temporo-parietal region of the scalp, left maxilla Once the patient arrived at the preparation room, 1 mL of xylocaine 10% and 2 drops of oxymetazoline nasal solution were instilled into the left nostril followed by nebulization of 3 mL of lidocaine 4%. The patient was given intravenous fentanyl 25 µg, dexamethasone 10 mg, diphenhydramine 10 mg, ketamine 10 mg, and midazolam 2 mg as premedication. In the operating room, oxygen was administered at 6 L/min with face mask for pre-oxygenation. The endotracheal tube size 7.0 was inserted into the FIS tube. Then, the FIS was inserted slowly into the left nostril. Once it reached the vocal cords, 2 mL of lidocaine 2% was sprayed through the working port and waited for 3-5 min. The FIS was again slowly advanced passing through the vocal cord until it reached the trachea, where 4 mL of lidocaine 2% was again sprayed. After 3-5 min, the patient coughed which helped the distribution of local anesthetic. The insertion of endotracheal tube was guided by the FIS and once the endotracheal tube was placed, the cuff was inflated followed by removal of the FIS and fixation of the endotracheal tube. After the intubation procedure was done, the patient was still awake and breathing spontaneously. For induction of anesthesia, intravenous propofol 100 mg, fentanyl 100 µg, and rocuronium 40 mg was administered. Anesthesia was maintained by sevoflurane in N2O + O2 inhalation and fentanyl 25 µg IV every 45 min.
The surgery was successfully completed, and the patient was conscious and cooperative during extubation. During observation in the recovery room, the patient’s vital signs were within normal limits. The patient was then transferred to the intermediate ward. After 18 days of care for the infection, the patient was discharged without any complications.
According to the American Society of Anesthesiologists (ASA), difficult airway is defined as a clinical situation in which an anesthesia care-trained physician experiences an anticipated or unanticipated difficulty or failure on one or more of the following: facemask ventilation, laryngoscopy, supraglottic airway ventilation, tracheal intubation, extubation, or invasive airway.4 Several conditions can predict difficult away including infection, such as dental abscess, Ludwig’s angina, epiglottitis or croup, which in our case was a parotid abscess.5 Physical examination may also help identify difficult airway. Mouth opening is measured by the inter-incisor distance and a gap of < 3 cm is considered a limitation for direct laryngoscope visualization. The thyromental distance, which is the distance between the chin and upper margin of the thyroid cartilage, is also commonly measured. The thyromental distance of < 6,5 cm is considered as difficult laryngoscopy. The Mallampati score is used to assess the size of the tongue and oropharyngeal cavity with score range from 1-4. Mallampati class of 3 and 4 is associated with difficulty in facemask ventilation and laryngoscopy.6 In our case, the patient presented with left-sided parotid abscess and physical examination revealed erythematous swelling of the left cheek that limited the patient’s mouth opening. The hyomental and thyrohyoid distances were decreased which indicated that the patient’s airway was too difficult to visualize with direct laryngoscopy. Therefore, we decided to choose awake intubation with flexible intubation scope for tracheal tube placement.
The current gold standard management of anticipated difficult airway is awake tracheal intubation (ATI) due to its low risk of complications and high success rate.4,7,8 The only absolute contraindication of ATI is patient’s rejection of the procedure. Several relative contraindications are; a history of allergic reaction to local anesthetic, airway hemorrhage, uncooperative patient, and certain tumors in the airway.5 There are several techniques in use for ATI including flexible bronchoscopy, video-laryngoscopy or both (video-assisted flexible/fiberoptic intubation).8 In 1967, surgical choledochoscope was first used for fiberoptic intubation by Dr Peter Murphy and later it became a potential airway management.5 Nowadays, awake fiberoptic intubation (AFI) is still preferred in cases of difficult airway.9 It can be inserted into the oral or nasal route depending on the patient’s condition, surgical access, and the availability of tool.8 AFI may also be performed in patients with limited neck movement because this procedure does not need head positioning and vocal cord visualization.3 Some advantages of AFI are reduced need of tracheostomy, lower risk of hypoxia and pulmonary aspiration caused by epistaxis.9 The success rate of awake flexible intubation scopes was quite high, reported ranging from 78-100%.4 In a cohort study, failed awake flexible intubation was found in 3.5% patients and the most common cause of failure was dislocation, followed by difficulty in passing the tube, patient distress and airway bleeding.10
Previous case reports have observed successful AFI in patients with difficult airway. Sung et al. (2014) presented a patient with upper airway obstruction post cervical fusion surgery. Intubation with laryngoscope was failed because the patient had short sternomental distance, limited neck movement, and flexed cervical angle. The author inserted a laryngeal mask to pass the endotracheal tube with the assistance of fiberoptic bronchoscope. The patient was extubated the following day and no airway complications were reported.9
Shaik et al. (2014) reported successful use of AFI through nasal route in a patient with difficult airway due to Ludwig's angina and concluded that this procedure is a less invasive airway management compared to tracheostomy.11 Raval et al. (2013) also presented a patient with submandibular abscess who underwent AFI and reported similar outcome.12 In other case report by Kang et al. (2013), AFI through nasal route was successful in a patient with temporomandibular joint ankylosis, who was unable to open his mouth, and underwent corrective spinal surgery due to ankylosing spondylitis. The author reported no airway swelling or any airway complication post-extubation.13
In this case, we successfully performed awake tracheal intubation assisted with flexible intubation scope in a patient with difficult airway due to large parotid abscess. We did not delay extubation as previous case reports mentioned, to prevent airway swelling. However, no complications or adverse condition was found in this patient. We conclude that awake fiberoptic intubation is a promising airway management technique for patients with anticipated difficult airway and should be performed by skilled anesthesiologist.
5. Ethical considerations
Written consent of the patient was obtained to publish his story for educational purposes.
6. Conflict of interests
The authors declare no conflict of interests.
7. Author contribution
CT, C: Conduct the case, literature review, manuscript writing
TGAS, IGAGUH: Supervise the case, review of the manuscript, final approval of manuscript
Author affiliations:
- Citra Tanoto, Resident, Department of Anesthesiology, Pain Management & Intensive Care, Udayana University/Sanglah Hospital, Bali, Indonesia; Email: citratanoto@yahoo.co.id
- Charles, Resident, Department of Anesthesiology, Pain Management, and Intensive Care Udayana University/Sanglah Hospital, Bali, Indonesia; Email: clebius2021@gmail.com
- Tjokorda Gde Agung Senapathi, Professor, Department of Anesthesiology, Pain Management, and Intensive Care Udayana University/Sanglah Hospital, Bali, Indonesia; Email: tjoksenapathi@unud.ac.id
- I Gusti Agung Gede Utara Hartawan, Lecturer, Department of Anesthesiology, Pain Management, and Intensive Care Udayana University/Sanglah Hospital, Bali, Indonesia; Email: utarahartawan@gmail.com
ABSTRACT
Parotid abscess originates from an ascending infection of the parotid gland through Stensen’s duct, which progresses into formation of pus. Infections involving the oral or neck structure may obscure the vocal cords and complicate the tracheal intubation with direct laryngoscopy. We present a case of 44-year-old male patient presented with painful swelling of the left cheek extending into the temporal region for four days. His physical examination revealed erythematous swelling of the left cheek that limited the patient’s mouth opening. He was diagnosed with left-sided parotid abscess and surgical drainage was planned. The hyoid-mental and thyrohyoid distances were decreased, which indicated that the patient’s airway might be difficult to visualize with direct laryngoscopy. We decided to choose awake intubation with flexible intubation scope for tracheal tube placement. The procedure went smoothly without any complication and the patient’s condition was stable throughout 18 days of care in the intermediate ward. The current gold standard management of anticipated difficult airway is awake tracheal intubation (ATI) and the American Society of Anesthesiologists recommended the use of non-invasive airway management devices, including flexible intubation scope. This procedure is preferred due to its low risk of complications and high success rates.
Keywords: Awake tracheal intubation; Awake fibreoptic intubation; Difficult airway; Flexible intubation scope; Parotid abscess
Citation: Tanoto C, Charles, Senapathi TGA, Utara Hartawan IGAG. Awake intubation with intubation fiberscope in a patient with difficult intubation and difficult ventilation: a case report. Anaesth. pain intensive care 2025;29(3):699-702. DOI: 10.35975/apic.v29i3.2768
Received: May 09, 2024; Revised: October 26, 2024; Accepted: January 01, 2025
1. INTRODUCTION
Parotid abscess is usually preceded by ascending infection into the parotid gland through Stensen’s duct. The incidence of this condition is quite low, and it mostly affects immunocompromised population, such as infants and elderly. The most common pathogens that cause parotid abscess are aerobic bacteria, including Staphylococcus aureus, Hemophilus influenzae, and Streptococcus pneumoniae. Poor oral cavity hygiene or dental infection are some of the predisposing factors of parotid infection. The infected intra-parotid and periparotid lymph nodes may cause pus formation and lead to abscess formation. If abscess formation persists, pus will enter the capsule and infiltrate the surrounding tissue and spread into the skin, external auditory canal or deep cervical fascial. Parotid abscess that extends to the head and neck
structures can cause airway obstruction which is potentially life-threatening.1,2
Tracheal intubation assisted by direct laryngoscopy following induction is the standard anesthetic procedure in most of these cases. However, patients with difficult airway, where visualizing the vocal cords might be difficult, is in higher risk of unsuccessful tracheal intubation with conventional laryngoscopy. Therefore, awake intubation is preferred as an alternative tracheal tube placement.3 Here we present a patient with difficult airway due to left-sided parotid abscess and awake intubation with Flexible Intubation Scope (FIS) was indicated.
2. CASE REPORT
A 44-year-old male patient with left-sided parotid abscess and orbital cellulitis presented with painful swelling of the left cheek extending into the temporal for four days. The patient also experienced difficulty in eating and drinking due to the painful swelling of the left cheek. Other complaints, such as fever, cough or shortness of breath, were denied. The patient had medical history of type 2 diabetes mellitus for 10 years and was currently on insulin treatment. The patient also had history of hypertension for 2 years and taking amlodipine regularly. Vital signs were within normal limits.
Anthropometric assessment found body weight 60 kg, height 175 cm and BMI 19.5 kg/m2. Physical examination of the head showed erythematous swelling of the left cheek (±7x8 cm) extending into the temporal and orbital region, warmth and fluctuant on palpation (Figure 1).
Figure 1: Physical examination showed erythematous swelling of the left cheek (±7x8 cm) extending into the temporal and orbital region.
Mouth opening was limited, the hyomental distance was more than three finger-breadths, and the thyrohyoid distance was more than two finger-breadths. The patient’s Mallampati class was too difficult to assess. Neck CT-scan with contrast revealed well-defined hypodense lesion with fluid density suggesting abscess in the left masticator space extending to the left ofacial, left pre-septal space, left parotid space, left submandibular and sublingual spaces, and left parapharyngeal space (Figure 2).
Figure 2: Neck CT-scan with contrast revealed well-defined hypodense lesion with fluid density suggesting abscess in the left masticator space extending to the left fronto-temporo-parietal region of the scalp.
Laboratory findings were unremarkable. We concluded the patient with ASA physical status III. The patient was scheduled for abscess drainage under general anesthesia with awake intubation using flexible intubation scope (FIS).fronto-temporo-parietal region of the scalp, left maxilla Once the patient arrived at the preparation room, 1 mL of xylocaine 10% and 2 drops of oxymetazoline nasal solution were instilled into the left nostril followed by nebulization of 3 mL of lidocaine 4%. The patient was given intravenous fentanyl 25 µg, dexamethasone 10 mg, diphenhydramine 10 mg, ketamine 10 mg, and midazolam 2 mg as premedication. In the operating room, oxygen was administered at 6 L/min with face mask for pre-oxygenation. The endotracheal tube size 7.0 was inserted into the FIS tube. Then, the FIS was inserted slowly into the left nostril. Once it reached the vocal cords, 2 mL of lidocaine 2% was sprayed through the working port and waited for 3-5 min. The FIS was again slowly advanced passing through the vocal cord until it reached the trachea, where 4 mL of lidocaine 2% was again sprayed. After 3-5 min, the patient coughed which helped the distribution of local anesthetic. The insertion of endotracheal tube was guided by the FIS and once the endotracheal tube was placed, the cuff was inflated followed by removal of the FIS and fixation of the endotracheal tube. After the intubation procedure was done, the patient was still awake and breathing spontaneously. For induction of anesthesia, intravenous propofol 100 mg, fentanyl 100 µg, and rocuronium 40 mg was administered. Anesthesia was maintained by sevoflurane in N2O + O2 inhalation and fentanyl 25 µg IV every 45 min.
The surgery was successfully completed, and the patient was conscious and cooperative during extubation. During observation in the recovery room, the patient’s vital signs were within normal limits. The patient was then transferred to the intermediate ward. After 18 days of care for the infection, the patient was discharged without any complications.
3. DISCUSSION
According to the American Society of Anesthesiologists (ASA), difficult airway is defined as a clinical situation in which an anesthesia care-trained physician experiences an anticipated or unanticipated difficulty or failure on one or more of the following: facemask ventilation, laryngoscopy, supraglottic airway ventilation, tracheal intubation, extubation, or invasive airway.4 Several conditions can predict difficult away including infection, such as dental abscess, Ludwig’s angina, epiglottitis or croup, which in our case was a parotid abscess.5 Physical examination may also help identify difficult airway. Mouth opening is measured by the inter-incisor distance and a gap of < 3 cm is considered a limitation for direct laryngoscope visualization. The thyromental distance, which is the distance between the chin and upper margin of the thyroid cartilage, is also commonly measured. The thyromental distance of < 6,5 cm is considered as difficult laryngoscopy. The Mallampati score is used to assess the size of the tongue and oropharyngeal cavity with score range from 1-4. Mallampati class of 3 and 4 is associated with difficulty in facemask ventilation and laryngoscopy.6 In our case, the patient presented with left-sided parotid abscess and physical examination revealed erythematous swelling of the left cheek that limited the patient’s mouth opening. The hyomental and thyrohyoid distances were decreased which indicated that the patient’s airway was too difficult to visualize with direct laryngoscopy. Therefore, we decided to choose awake intubation with flexible intubation scope for tracheal tube placement.
The current gold standard management of anticipated difficult airway is awake tracheal intubation (ATI) due to its low risk of complications and high success rate.4,7,8 The only absolute contraindication of ATI is patient’s rejection of the procedure. Several relative contraindications are; a history of allergic reaction to local anesthetic, airway hemorrhage, uncooperative patient, and certain tumors in the airway.5 There are several techniques in use for ATI including flexible bronchoscopy, video-laryngoscopy or both (video-assisted flexible/fiberoptic intubation).8 In 1967, surgical choledochoscope was first used for fiberoptic intubation by Dr Peter Murphy and later it became a potential airway management.5 Nowadays, awake fiberoptic intubation (AFI) is still preferred in cases of difficult airway.9 It can be inserted into the oral or nasal route depending on the patient’s condition, surgical access, and the availability of tool.8 AFI may also be performed in patients with limited neck movement because this procedure does not need head positioning and vocal cord visualization.3 Some advantages of AFI are reduced need of tracheostomy, lower risk of hypoxia and pulmonary aspiration caused by epistaxis.9 The success rate of awake flexible intubation scopes was quite high, reported ranging from 78-100%.4 In a cohort study, failed awake flexible intubation was found in 3.5% patients and the most common cause of failure was dislocation, followed by difficulty in passing the tube, patient distress and airway bleeding.10
Previous case reports have observed successful AFI in patients with difficult airway. Sung et al. (2014) presented a patient with upper airway obstruction post cervical fusion surgery. Intubation with laryngoscope was failed because the patient had short sternomental distance, limited neck movement, and flexed cervical angle. The author inserted a laryngeal mask to pass the endotracheal tube with the assistance of fiberoptic bronchoscope. The patient was extubated the following day and no airway complications were reported.9
Shaik et al. (2014) reported successful use of AFI through nasal route in a patient with difficult airway due to Ludwig's angina and concluded that this procedure is a less invasive airway management compared to tracheostomy.11 Raval et al. (2013) also presented a patient with submandibular abscess who underwent AFI and reported similar outcome.12 In other case report by Kang et al. (2013), AFI through nasal route was successful in a patient with temporomandibular joint ankylosis, who was unable to open his mouth, and underwent corrective spinal surgery due to ankylosing spondylitis. The author reported no airway swelling or any airway complication post-extubation.13
4. CONCLUSION
In this case, we successfully performed awake tracheal intubation assisted with flexible intubation scope in a patient with difficult airway due to large parotid abscess. We did not delay extubation as previous case reports mentioned, to prevent airway swelling. However, no complications or adverse condition was found in this patient. We conclude that awake fiberoptic intubation is a promising airway management technique for patients with anticipated difficult airway and should be performed by skilled anesthesiologist.
5. Ethical considerations
Written consent of the patient was obtained to publish his story for educational purposes.
6. Conflict of interests
The authors declare no conflict of interests.
7. Author contribution
CT, C: Conduct the case, literature review, manuscript writing
TGAS, IGAGUH: Supervise the case, review of the manuscript, final approval of manuscript
8. REFERENCES
- Brook I. Acute bacterial suppurative parotitis: microbiology and management. J Craniofac Surg. 2003;14(1):37–40. PubMed DOI: 1097/00001665-200301000-00006
- Viselner G, van der Byl G, Maira A, Merico V, Draghi F. Parotid abscess: mini-pictorial essay. J Ultrasound. 2013;16(1):11–5. PubMed DOI: 1007/s40477-013-0006-0
- Nicholson A, Smith AF, Lewis SR, Cook TM. Tracheal intubation with a flexible intubation scope versus other intubation techniques for obese patients requiring general anaesthesia. Cochrane Database Syst Rev. 2014;2014(4):CD010320. PubMed DOI: 1002/14651858.CD010320.pub2
- Apfelbaum JL, Hagberg CA, Connis RT, Abdelmalak BB, Agarkar M, Dutton RP, et al. 2022 American Society of Anesthesiologists practice guidelines for management of the difficult airway. Anesthesiology. 2022;136(1):31–81. PubMed DOI: 1097/ALN.0000000000004002
- Leslie D, Stacey M. Awake intubation. Contin Educ Anaesth Crit Care Pain. 2015;15(2):64–7. DOI: 1093/bjaceaccp/mku015
- Crawley S, Dalton A. Predicting the difficult airway. BJA Educ. 2015;15(5):253–8. DOI: 1093/bjaceaccp/mku047
- Cook TM, MacDougall-Davis SR. Complications and failure of airway management. Br J Anaesth. 2012;109:i68–85. PubMed
- Vora J, Leslie D, Stacey M. Awake tracheal intubation. BJA Educ. 2022;22(8):298–305. DOI: 1016/j.bjae.2022.03.006
- Sung JK, Kim HG, Kim JE, Jang MS, Kang JM. Endotracheal tube intubation with the aid of a laryngeal mask airway, a fiberoptic bronchoscope, and a tube exchanger in a difficult airway patient: a case report. Korean J Anesthesiol. 2014;66(3):237. PubMed DOI: 4097/kjae.2014.66.3.237
- Karlsen KAH, Gisvold SE, Nordseth T, Fasting S. Incidence, causes, and management of failed awake fibreoptic intubation—a retrospective study of 833 procedures. Acta Anaesthesiol Scand. 2023;67(10):1341–7. PubMed DOI: 1111/aas.14313
- Shaikh SI, Sarala B, Bhosale R. Anaesthetic management of case of Ludwig’s angina: forewarned is forearmed. Int J Biomed Adv Res. 2014;5(2):123–5. FullText
- Raval CB, Khan S. Airway management in submandibular abscess patient with awake fibreoptic intubation—a case report. Middle East J Anaesthesiol. 2012;21(4):647–51. PubMed
- Kang JM, Lee KW, Kim DO, Yi JW. Airway management of an ankylosing spondylitis patient with severe temporomandibular joint ankylosis and impossible mouth opening. Korean J Anesthesiol. 2013;64(1):84. PubMed DOI: 4097/kjae.2013.64.1.84