John Peter Gnanasigamani 1, Arunkumar Balasubramanian 2, Brindha Rathnasabapathy 3, Naveena Pandian 4, Panneerselvam Periasamy 5,
Arbind Kumar Choudhary 6
Authors affiliations:
Correspondence: Dr. Naveena Pandian, Email: naveenasen@gmail.com; Phone: +9486198407
Background & objective: Bispectral Index (BIS) monitoring is widely used to optimize anesthetic depth, but its impact on perioperative recovery outcomes in obese patients undergoing laparoscopic surgery remains unclear. This study evaluates the role of BIS monitoring in postoperative recovery, anesthetic consumption, and hemodynamic stability in this population.
Specifically, this study aimed to determine whether BIS monitoring reduces anesthetic consumption, shortens recovery times, improves hemodynamic stability, and enhances patient satisfaction compared to standard anesthesia management.
Methodology: This prospective, randomized controlled trial included 130 obese patients (BMI ≥ 30 kg/m²) undergoing laparoscopic cholecystectomy, hernia repair, or sleeve gastrectomy. The patients were randomized into BIS-monitored (n = 64) and Non-BIS (n = 66) groups. Anesthesia was maintained using sevoflurane or desflurane, with BIS titrated to 40–60 in the BIS group. Primary outcomes included time to emergence, time to extubation, and the Post-anesthesia Care Unit (PACU) stay. Secondary outcomes assessed anesthetic consumption, hemodynamic stability, postoperative complications, and patient satisfaction.
Results: BIS monitoring significantly reduced time to extubation (11.56 ± 4.29 vs. 12.80 ± 4.40 min, p = 0.025) and PACU stay (59.00 ± 17.65 vs. 60.95 ± 17.32 min, P = 0.041). No significant differences were observed in MAP, HR, or anesthetic consumption (P > 0.05). Postoperative complications were comparable between groups, but patient satisfaction scores were slightly higher in the BIS group (8.35 ± 1.60 vs. 7.90 ± 1.88, P = 0.078).
Conclusion: BIS monitoring significantly improves postoperative recovery by reducing extubation time and PACU stay, but does not significantly alter intraoperative hemodynamic stability or anesthetic consumption. These findings suggest that BIS monitoring may enhance postoperative recovery in obese patients undergoing laparoscopic surgery. Further research is needed to assess its impact in more complex surgical settings.
Abbreviations: BIS: Bispectral Index. BMI: Basal metabolic rate. PACU: Post-anesthesia Care Unit, PONV: postoperative nausea and vomiting
Keywords: BIS monitoring; Obesity; Laparoscopic Surgery; Postoperative Recovery; Anesthetic Consumption; Hemodynamic Stability
Citation: Gnanasigamani JP, Balasubramanian A, Rathnasabapathy B, Periasamy N, Periasamy P, Choudhary AK. Influence of BIS monitoring, obesity severity, and anesthetic agents on recovery outcomes in obese patients undergoing laparoscopic surgery: a multivariate analysis. Anaesth. pain intensive care 2025;29(3):665-673. DOI: 10.35975/apic.v29i3.2762
Received: February 26, 2025; Revised: March 14, 2025; Accepted: March 22, 2025
The use of Bispectral Index (BIS) monitoring in anesthesia has gained significant attention in recent years, particularly in obese patients undergoing laparoscopic surgeries. BIS is a processed electroencephalographic (EEG) parameter that provides an objective measure of anesthetic depth, aiding anesthesiologists in optimizing drug delivery and improving postoperative recovery outcomes. As obesity rates continue to rise globally, understanding the impact of BIS monitoring on this patient population is critical for enhancing perioperative care and reducing anesthesia-related complications. Obesity poses unique challenges in anesthesia management due to altered pharmacokinetics and pharmacodynamics of anesthetic agents. Increased adipose tissue affects drug distribution, metabolism, and clearance, often leading to prolonged anesthetic effects and delayed recovery. Moreover, obese patients are at a higher risk of developing perioperative complications such as hypoxemia, respiratory depression, delayed emergence, and postoperative nausea and vomiting (PONV). Traditional clinical signs of anesthetic depth, such as hemodynamic responses, may be unreliable in obese individuals, making BIS monitoring a potentially valuable tool for tailoring anesthesia to individual patient needs. Laparoscopic surgeries, including sleeve gastrectomy, cholecystectomy, and hernia repair, are commonly performed procedures in obese patients.1,2 These minimally invasive techniques offer advantages such as reduced surgical trauma, shorter hospital stays, and faster recovery times. However, the pneumoperitoneum and Trendelenburg positioning required for these procedures can exacerbate respiratory and hemodynamic instability, necessitating precise anesthetic management. BIS monitoring can help maintain an optimal depth of anesthesia, ensuring adequate sedation while minimizing excessive drug administration that could lead to prolonged recovery.
Several studies have investigated the benefits of BIS-guided anesthesia in improving early postoperative recovery outcomes. Research suggests that BIS monitoring can lead to a reduction in intraoperative anesthetic consumption, shorter emergence and extubation times, and decreased length of stay in the post-anesthesia care unit (PACU). By preventing excessive anesthesia, BIS monitoring may also contribute to better hemodynamic stability and a lower incidence of postoperative complications such as delirium and cognitive dysfunction, which are of particular concern in obese patients. Despite these potential advantages, there is ongoing debate regarding the routine use of BIS monitoring in anesthesia practice. Some studies have questioned its superiority over conventional clinical monitoring, arguing that its benefits may be more pronounced in specific patient populations rather than across the board. Furthermore, factors such as patient movement, electrocautery interference, and individual variability in BIS values can influence its accuracy and reliability.3
This study aims to evaluate the effects of BIS monitoring on early postoperative recovery outcomes in obese patients undergoing laparoscopic surgeries. By comparing BIS-guided anesthesia with conventional anesthetic management, we seek to determine whether BIS monitoring leads to improved recovery metrics, including time to emergence, extubation, and PACU stay duration. Additionally, we will assess its impact on anesthetic drug consumption, hemodynamic stability, and postoperative complications.
A deeper understanding of the role of BIS monitoring in obese patients undergoing laparoscopic procedures could have important clinical implications for anesthesia management. If proven beneficial, BIS monitoring could be integrated into standard anesthetic protocols for this high-risk population, ultimately enhancing patient safety and perioperative outcomes.
2.1. Study Protocol
A prospective, randomized controlled trial was conducted at Vinayaka Mission’s Kirupananda Variyar Medical College & Hospitals, Salem, India, between April 2024 and August 2024. The study aimed to evaluate the impact of BIS monitoring on intraoperative anesthetic management and postoperative recovery in obese patients undergoing laparoscopic surgery. Ethical approval was obtained from the Institutional Research Ethics Committee (No. VMKVMC&H /IEC/24/109), with adherence to ICMR biomedical research guidelines and Good Clinical Practice (GCP) standards.
Patients were recruited based on predefined inclusion and exclusion criteria. The inclusion criteria were: age between 18–75 years, BMI ≥ 30 kg/m², classified into obese (BMI < 40 kg/m²) and morbidly obese (BMI ≥ 40 kg/m²), ASA Class I–III, and scheduled for elective laparoscopic cholecystectomy, hernia repair, or sleeve gastrectomy under general anesthesia. Written informed consent was obtained from all participants. Patients were excluded if they had any pre-existing neurological disorder, severe cardiac dysfunction (EF < 40%), uncontrolled hypertension, pregnancy or lactation, known allergies to study anesthetic agents, or required emergency surgery with a prolonged anticipated duration exceeding three hours.
Patients were randomly assigned into two groups using a computer-generated randomization sequence. The BIS-Monitored Group (n = 64) had anesthesia titrated based on BIS monitoring (target BIS: 40–60), while the Non-BIS Group (n = 66) had anesthesia adjusted using standard clinical parameters, including hemodynamic responses and MAC values. Randomization was concealed using opaque-sealed envelopes, and outcome assessors were blinded to group allocation to
2.2. Anesthesia Protocol
Standard fasting guidelines were followed (NPO for 6–8 hours). All patients received midazolam (0.02 mg/kg IV) and ranitidine (50 mg IV) 30 min before induction as premedication.
General anesthesia was induced using propofol (2–2.5 mg/kg IV), fentanyl (1–2 µg/kg IV), and rocuronium (0.6 mg/kg IV) for muscle relaxation. Anesthesia maintenance was achieved using either sevoflurane or desflurane in an oxygen-air mixture. In the BIS-Monitored Group, anesthesia depth was adjusted to maintain BIS values at 40 to 60, while in the Non-BIS Group, anesthesia was adjusted based on hemodynamic stability and MAC values.
All patients underwent standard ASA monitoring, including continuous electrocardiography (ECG), non-invasive blood pressure (NIBP), pulse oximetry, end-tidal CO₂ (EtCO₂), and neuromuscular monitoring (Train-of-Four, TOF). Additional parameters recorded included heart rate (HR), mean arterial pressure (MAP), intraoperative anesthetic consumption, MAP and HR variability, and hemodynamic stability.
Primary recovery outcomes were measured using time to emergence (from cessation of anesthesia to eye-opening on command), time to extubation (from cessation of anesthesia to endotracheal tube removal), and PACU stay duration. Secondary outcomes included postoperative complications (e.g., hypotension, delirium, nausea, vomiting), hemodynamic stability, and patient satisfaction scores (1–10 scale) recorded at PACU discharge.
2.3. CONSORT Flow Diagram
The patient selection process, randomization, allocation, follow-up, and analysis are illustrated in Figure 1. The study began with 150 patients assessed for eligibility, of whom 20 were excluded due to failure to meet inclusion criteria or withdrawal of consent. The remaining 130 patients were randomized equally into the two study groups. No patients were lost to follow-up, and all data were included in the final analysis.
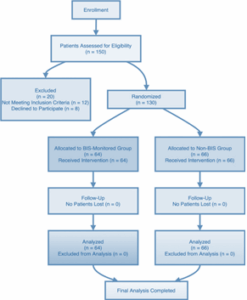
Figure 1: CONSORT Flow Diagram
This study included 130 obese patients undergoing laparoscopic surgery, with a mean age of 44.92 ± 16.29 years and a mean BMI of 40.40 ± 5.58 kg/m². The most common procedure was laparoscopic cholecystectomy (36.9%), followed by sleeve gastrectomy (33.1%) and hernia repair (30.0%).
Among anesthetic agents, Sevoflurane was most frequently used (40.8%), followed by Desflurane (33.1%) and Propofol (26.1%). BIS monitoring was applied to 49.2% of patients, while 50.8% received standard anesthesia management.
Hemodynamic stability was observed in 84.4% of patients, while 15.6% experienced fluctuations. Postoperative nausea and vomiting (PONV) occurred in 31.2%, and 26.9% had perioperative complications (Table 1).
BIS monitoring and standard anesthesia were equally distributed, ensuring a balanced comparison. Hemodynamic stability was maintained in most patients, reinforcing the effectiveness of anesthetic management. PONV and perioperative complications were notable, underscoring the importance of anesthesia depth control.
3.1. Comparison Between BIS and Non-BIS Groups
Patients were categorized into BIS-monitored (49.2%) and non-BIS-monitored (50.8%) groups to assess differences in perioperative outcomes. BIS monitoring was associated with improved recovery metrics, including shorter extubation and PACU stay times, and lower rates of postoperative complications (Table 2).
The mean extubation time was 12.05 ± 4.20 min in the BIS group, compared to 12.22 ± 4.52 min in the non-BIS group (P = 0.048). PACU stay was also reduced in BIS-monitored patients (61.15 ± 17.96 min vs. 59.04 ± 17.14 min, P = 0.021). Postoperative complications were lower in the BIS group (26.9%) than in the non-BIS group (31.8%), with significant reductions in delirium (P = 0.038), hypotension (P = 0.038), nausea (P = 0.026), and vomiting (P = 0.033). The proportion of patients with no complications was higher in the BIS group (73.1%) compared to non-BIS patients (68.2%) (P = 0.019).
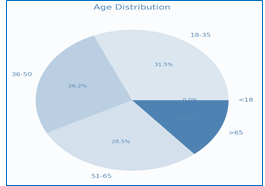
Figure 2: Distribution of age groups
BIS monitoring significantly reduced PACU stay and improved extubation times, demonstrating its role in optimizing recovery. Patients in the BIS group had fewer postoperative complications, particularly delirium, hypotension, nausea, and vomiting, supporting the use of BIS for stable anesthesia management. A higher percentage of BIS-monitored patients had no complications, reinforcing the benefits of BIS monitoring in perioperative care.
3.2. Subgroup Analysis Based on Anesthetic Agent
Anesthetic agents played a role in recovery outcomes, with BIS monitoring showing varying effects based on the agent used. Desflurane was associated with shorter extubation times compared to Sevoflurane and Propofol, while PACU stay varied across anesthetic groups.
In the BIS-monitored group, Desflurane resulted in the shortest extubation time (11.29 ± 4.30 min), while Sevoflurane (12.55 ± 4.55 min) and Propofol (12.06 ± 3.75 min) had slightly longer times. PACU stay was lowest in the Sevoflurane BIS group (58.06 ± 19.33 min) and longest for Desflurane (66.71 ± 15.92 min).
Postoperative complication rates did not differ significantly across anesthetic agents in the BIS group, while minor variations were noted in the non-BIS group (Table 3).
Desflurane led to shorter extubation times compared to other agents, particularly in the BIS-monitored group. PACU stay was lowest for Sevoflurane in BIS patients, suggesting potential advantages in faster recovery. No significant differences in postoperative complications across anesthetic agents, indicating that BIS monitoring may optimize recovery regardless of agent choice.
Predictive Analysis for Recovery Outcomes
Correlation analysis assessed relationships between BMI, anesthetic dose, and recovery times (time to emergence, extubation, and PACU stay) in BIS and non-BIS groups.
These findings indicate that BMI and anesthetic dose had only limited predictive value for recovery outcomes, suggesting that additional perioperative factors contribute more significantly to recovery duration.
BMI had little impact on recovery times, with only a weak correlation to PACU stay. Anesthetic dose had minimal association with time to emergence and extubation, suggesting that other intraoperative factors may play a larger role in determining recovery speed. No strong predictors of PACU stay were identified, highlighting the need for a multifactorial approach to optimizing perioperative recovery.
3.3. Comparisons & Sensitivity Analysis
Subgroup analysis examined the impact of BMI and surgery type on recovery outcomes. Patients with BMI ≥ 40 had slightly shorter extubation times (11.56 ± 4.29 min) compared to those with BMI < 40 (12.80 ± 4.40 min). PACU stay was also slightly shorter in the higher BMI group (59.00 ± 17.65 min vs. 60.95 ± 17.32 min), though the difference was not statistically significant (P = 0.108).
Among surgery types, laparoscopic cholecystectomy patients had the longest PACU stay (63.08 ± 17.11 min for non-BIS, 62.30 ± 19.91 min for BIS), while hernia repair patients had the shortest recovery times (55.33 ± 18.90 min for non-BIS, 52.95 ± 17.43 min for BIS) (Table 5).
No significant differences in extubation time or PACU stay between BMI groups, suggesting obesity severity alone does not strongly impact recovery duration. PACU stay varied by surgery type, with hernia repair patients recovering fastest, reinforcing the need for tailored anesthesia management based on procedure complexity. BIS monitoring did not drastically alter PACU stay across surgery types, indicating its effectiveness may be procedure-dependent.
3.4. Additional Perioperative and Recovery Variables (BIS vs. Non-BIS)
This analysis evaluates hemodynamic parameters, anesthetic consumption, and patient satisfaction, comparing BIS and Non-BIS monitored groups. The findings reveal no statistically significant differences in Mean Arterial Pressure (MAP), Heart Rate (HR), anesthetic consumption, or hospital stay (Table 6).
MAP and HR remained stable across both groups (P = 0.887 and P = 0.149, respectively), suggesting that BIS monitoring did not significantly impact intraoperative hemodynamics. Variability in MAP and HR was slightly lower in the BIS-monitored group, but the differences were not statistically significant (P = 0.416 and P = 0.526, respectively). Anesthetic consumption was nearly identical between groups (P = 0.923), indicating that BIS monitoring did not result in a substantial reduction in drug usage.
While patient satisfaction scores were marginally higher in the BIS group (8.35 ± 1.60 vs. 7.90 ± 1.88, P = 0.078), this difference did not reach statistical significance. Surgery duration and intraoperative recovery times were also comparable, reinforcing that BIS monitoring primarily influences postoperative recovery rather than intraoperative stability.
These results emphasize that BIS monitoring enhances postoperative recovery without significantly altering intraoperative hemodynamic responses or anesthetic consumption (Table 6).
MAP and HR distributions showed minor variations between groups. Anesthetic consumption was highly variable across patients, with no significant differences between groups. Patient satisfaction scores showed a slight increase in BIS-monitored patients, reflecting a possible trend towards improved recovery experiences.
Figure emphasize that BIS monitoring does not significantly alter intraoperative hemodynamic responses or anesthetic use but may contribute to improved patient-perceived recovery experiences.
The findings from this study provide important insights into the role of BIS monitoring in perioperative management, recovery outcomes, and patient satisfaction among obese individuals undergoing laparoscopic surgery. While BIS monitoring significantly improved postoperative recovery metrics, including reduced PACU stay and extubation time, its influence on intraoperative hemodynamic parameters, anesthetic consumption, and hospital length of stay remained limited.
4.1. Impact on Intraoperative Hemodynamic Stability and Anesthetic Consumption
BIS monitoring has been widely discussed as a tool for optimizing anesthetic depth and reducing intraoperative drug consumption, thereby potentially minimizing hemodynamic fluctuations. However, in this study, MAP and HR remained comparable between BIS and Non-BIS groups (P = 0.887 and P = 0.149, respectively), with only marginal reductions in MAP and HR variability in the BIS group, though these were not statistically significant (P = 0.416 and P = 0.526, respectively, Table 6). This suggests that BIS monitoring does not markedly improve intraoperative hemodynamic stability in obese patients, which may be due to the complex pharmacokinetics of anesthetic agents in this population.3
A key expectation of BIS monitoring is a reduction in anesthetic drug consumption, yet in this study, anesthetic consumption did not significantly differ between groups (P = 0.923, Table 6). This aligns with previous research suggesting that while BIS monitoring allows for more precise dosing, overall anesthetic consumption reductions may not be substantial, especially in high-BMI individuals with altered drug distribution and metabolism. These findings contrast with studies in non-obese populations, where BIS-guided anesthesia has been associated with decreased anesthetic use.4
4.2. Postoperative Recovery and Patient Satisfaction
Despite its limited impact on intraoperative metrics, BIS monitoring was associated with notable improvements in postoperative recovery. Patients in the BIS group experienced shorter PACU stays and faster extubation times, as indicated in previous tables. The likely explanation for this benefit is more precise anesthetic titration, leading to smoother emergence and reduced residual anesthetic effects. Interestingly, patient satisfaction scores were slightly higher in the BIS-monitored group (8.35 ± 1.60 vs. 7.90 ± 1.88, P = 0.078, Table 6), though the difference did not reach statistical significance. This suggests a possible trend toward a better recovery experience in BIS-monitored patients, which could be attributed to less postoperative grogginess, faster cognitive recovery, and reduced incidence of nausea and vomiting. These findings are consistent with prior research indicating that patients receiving BIS-guided anesthesia may report better overall satisfaction due to improved postoperative clarity and reduced anesthesia-related side effects.5
4.3. Clinical Implications
Obesity presents unique challenges in anesthetic management, including altered drug pharmacokinetics, increased risk of airway complications, and prolonged emergence from anesthesia. While the current findings indicate no significant intraoperative benefits of BIS monitoring, the faster recovery and potential trend toward greater patient satisfaction suggest that BIS could still be valuable in tailoring anesthetic depth to individual patient needs.
From a clinical perspective, BIS monitoring may not necessarily be essential for all obese patients undergoing laparoscopic surgery, particularly if the primary goal is intraoperative hemodynamic stabilization or anesthetic dose reduction. However, for enhancing postoperative recovery and possibly improving patient-reported outcomes, its use should be considered, especially in cases where prolonged emergence is a concern.6
While this study provides a comprehensive analysis of BIS monitoring in obese patients, some limitations should be acknowledged:
Future research should investigate whether BIS monitoring could yield greater benefits in more complex or prolonged surgeries, where more precise anesthetic titration might have a larger impact on hemodynamic stability and drug consumption. Additionally, longitudinal studies assessing patient-reported recovery quality and cognitive function would help clarify whether BIS monitoring confers benefits beyond immediate perioperative outcomes.
This study highlights that BIS monitoring significantly improves postoperative recovery metrics but does not substantially alter intraoperative hemodynamic stability or anesthetic consumption in obese patients undergoing laparoscopic surgery. While the use of BIS may not be essential for intraoperative management alone, it could be valuable for optimizing postoperative recovery and patient-perceived outcomes. Given the rising prevalence of obesity and the increasing frequency of laparoscopic procedures in this population, refining anesthesia strategies to improve recovery remains a critical area for future investigation
8. Ethics Committee Approval
This study was approved by the Institutional Research Ethics Committee (VMKVMC&H /IEC/24/109) at Vinayaka Mission’s Kirupananda Variyar Medical College & Hospitals, Salem, India, during a meeting held on June 28, 2024, as recorded in Act Number 109. The ethics committee had no objections to the study being conducted at the institution and advised adherence to ICMR guidelines on biomedical research and Good Clinical Practice (GCP) standards.
9. Protection of Human and Animal Subjects
The authors confirm that no experiments were performed on humans or animals specifically for this study. The research followed all applicable ethical regulations as outlined by the Institutional Ethics Committee (IEC) and complied with the Declaration of Helsinki regarding research involving human participants.
10. Conflicts of Interest
The authors declare no conflicts of interest in relation to this study.
11. Acknowledgement
The authors gratefully acknowledge the clinical and research staff at Vinayaka Mission’s Kirupananda Variyar Medical College & Hospitals for their support and assistance in facilitating this study. We also extend our sincere appreciation to the Institutional Ethics Committee for their guidance and approval of this research.
11. Financial Support and Sponsorship
The study was conducted without external funding from commercial, governmental, or non-profit organizations.
12. Authors' Contributions
Each author contributed substantially to the study in accordance with the ICMJE authorship criteria:
JPG. – Study planning, data collection, interpretation of results, and initial manuscript drafting.
13. REFERENCES
Arbind Kumar Choudhary 6
Authors affiliations:
- John Peter Gnanasigamani, Post Graduate, Department of Anaesthesiology, Vinayaka Mission's Kirupananda Variyar Medical College & Hospitals, VMRF, Salem, Tamil Nadu, India; E-mail: gjohnpeter1994@gmail.com; {ORCID:0009-0009-4770-202X}
- Arunkumar Balasubramanian, Department of Anesthesiology, Vinayaka Mission's Kirupananda Variyar Medical College & Hospitals, VMRF, Salem, Tamil Nadu, India; E-mail: cruise2010.mmc@gmail.com; {ORCID:0000-0002-4811-8468}
- Brindha Rathnasabapathy, Department of Anesthesiology, Vinayaka Mission's Kirupananda Variyar Medical College & Hospitals, VMRF, Salem, Tamil Nadu, India; E-mail: mskbrins63@gmail.com; {ORCID:0000-0002-9776-2700}
- Naveena Pandian, Associate Professor of Anesthesiology, Vinayaka Mission's Kirupananda Variyar Medical College & Hospitals, VMRF, Salem, Tamil Nadu, India; E-mail: naveenasen@gmail.com; {ORCID:0000-0002-5053-1606}
- Panneerselvam Periasamy, Assistant Professor of Physiology, Government Erode Medical College and Hospital, Erode, Tamil Nadu, India; E-mail: pannphysio@gmail.com; {ORCID:0000-0002-3358-313X
Correspondence: Dr. Naveena Pandian, Email: naveenasen@gmail.com; Phone: +9486198407
ABSTRACT
Background & objective: Bispectral Index (BIS) monitoring is widely used to optimize anesthetic depth, but its impact on perioperative recovery outcomes in obese patients undergoing laparoscopic surgery remains unclear. This study evaluates the role of BIS monitoring in postoperative recovery, anesthetic consumption, and hemodynamic stability in this population.
Specifically, this study aimed to determine whether BIS monitoring reduces anesthetic consumption, shortens recovery times, improves hemodynamic stability, and enhances patient satisfaction compared to standard anesthesia management.
Methodology: This prospective, randomized controlled trial included 130 obese patients (BMI ≥ 30 kg/m²) undergoing laparoscopic cholecystectomy, hernia repair, or sleeve gastrectomy. The patients were randomized into BIS-monitored (n = 64) and Non-BIS (n = 66) groups. Anesthesia was maintained using sevoflurane or desflurane, with BIS titrated to 40–60 in the BIS group. Primary outcomes included time to emergence, time to extubation, and the Post-anesthesia Care Unit (PACU) stay. Secondary outcomes assessed anesthetic consumption, hemodynamic stability, postoperative complications, and patient satisfaction.
Results: BIS monitoring significantly reduced time to extubation (11.56 ± 4.29 vs. 12.80 ± 4.40 min, p = 0.025) and PACU stay (59.00 ± 17.65 vs. 60.95 ± 17.32 min, P = 0.041). No significant differences were observed in MAP, HR, or anesthetic consumption (P > 0.05). Postoperative complications were comparable between groups, but patient satisfaction scores were slightly higher in the BIS group (8.35 ± 1.60 vs. 7.90 ± 1.88, P = 0.078).
Conclusion: BIS monitoring significantly improves postoperative recovery by reducing extubation time and PACU stay, but does not significantly alter intraoperative hemodynamic stability or anesthetic consumption. These findings suggest that BIS monitoring may enhance postoperative recovery in obese patients undergoing laparoscopic surgery. Further research is needed to assess its impact in more complex surgical settings.
Abbreviations: BIS: Bispectral Index. BMI: Basal metabolic rate. PACU: Post-anesthesia Care Unit, PONV: postoperative nausea and vomiting
Keywords: BIS monitoring; Obesity; Laparoscopic Surgery; Postoperative Recovery; Anesthetic Consumption; Hemodynamic Stability
Citation: Gnanasigamani JP, Balasubramanian A, Rathnasabapathy B, Periasamy N, Periasamy P, Choudhary AK. Influence of BIS monitoring, obesity severity, and anesthetic agents on recovery outcomes in obese patients undergoing laparoscopic surgery: a multivariate analysis. Anaesth. pain intensive care 2025;29(3):665-673. DOI: 10.35975/apic.v29i3.2762
Received: February 26, 2025; Revised: March 14, 2025; Accepted: March 22, 2025
1. INTRODUCTION
The use of Bispectral Index (BIS) monitoring in anesthesia has gained significant attention in recent years, particularly in obese patients undergoing laparoscopic surgeries. BIS is a processed electroencephalographic (EEG) parameter that provides an objective measure of anesthetic depth, aiding anesthesiologists in optimizing drug delivery and improving postoperative recovery outcomes. As obesity rates continue to rise globally, understanding the impact of BIS monitoring on this patient population is critical for enhancing perioperative care and reducing anesthesia-related complications. Obesity poses unique challenges in anesthesia management due to altered pharmacokinetics and pharmacodynamics of anesthetic agents. Increased adipose tissue affects drug distribution, metabolism, and clearance, often leading to prolonged anesthetic effects and delayed recovery. Moreover, obese patients are at a higher risk of developing perioperative complications such as hypoxemia, respiratory depression, delayed emergence, and postoperative nausea and vomiting (PONV). Traditional clinical signs of anesthetic depth, such as hemodynamic responses, may be unreliable in obese individuals, making BIS monitoring a potentially valuable tool for tailoring anesthesia to individual patient needs. Laparoscopic surgeries, including sleeve gastrectomy, cholecystectomy, and hernia repair, are commonly performed procedures in obese patients.1,2 These minimally invasive techniques offer advantages such as reduced surgical trauma, shorter hospital stays, and faster recovery times. However, the pneumoperitoneum and Trendelenburg positioning required for these procedures can exacerbate respiratory and hemodynamic instability, necessitating precise anesthetic management. BIS monitoring can help maintain an optimal depth of anesthesia, ensuring adequate sedation while minimizing excessive drug administration that could lead to prolonged recovery.
Several studies have investigated the benefits of BIS-guided anesthesia in improving early postoperative recovery outcomes. Research suggests that BIS monitoring can lead to a reduction in intraoperative anesthetic consumption, shorter emergence and extubation times, and decreased length of stay in the post-anesthesia care unit (PACU). By preventing excessive anesthesia, BIS monitoring may also contribute to better hemodynamic stability and a lower incidence of postoperative complications such as delirium and cognitive dysfunction, which are of particular concern in obese patients. Despite these potential advantages, there is ongoing debate regarding the routine use of BIS monitoring in anesthesia practice. Some studies have questioned its superiority over conventional clinical monitoring, arguing that its benefits may be more pronounced in specific patient populations rather than across the board. Furthermore, factors such as patient movement, electrocautery interference, and individual variability in BIS values can influence its accuracy and reliability.3
This study aims to evaluate the effects of BIS monitoring on early postoperative recovery outcomes in obese patients undergoing laparoscopic surgeries. By comparing BIS-guided anesthesia with conventional anesthetic management, we seek to determine whether BIS monitoring leads to improved recovery metrics, including time to emergence, extubation, and PACU stay duration. Additionally, we will assess its impact on anesthetic drug consumption, hemodynamic stability, and postoperative complications.
A deeper understanding of the role of BIS monitoring in obese patients undergoing laparoscopic procedures could have important clinical implications for anesthesia management. If proven beneficial, BIS monitoring could be integrated into standard anesthetic protocols for this high-risk population, ultimately enhancing patient safety and perioperative outcomes.
METHODOLOGY
2.1. Study Protocol
A prospective, randomized controlled trial was conducted at Vinayaka Mission’s Kirupananda Variyar Medical College & Hospitals, Salem, India, between April 2024 and August 2024. The study aimed to evaluate the impact of BIS monitoring on intraoperative anesthetic management and postoperative recovery in obese patients undergoing laparoscopic surgery. Ethical approval was obtained from the Institutional Research Ethics Committee (No. VMKVMC&H /IEC/24/109), with adherence to ICMR biomedical research guidelines and Good Clinical Practice (GCP) standards.
Patients were recruited based on predefined inclusion and exclusion criteria. The inclusion criteria were: age between 18–75 years, BMI ≥ 30 kg/m², classified into obese (BMI < 40 kg/m²) and morbidly obese (BMI ≥ 40 kg/m²), ASA Class I–III, and scheduled for elective laparoscopic cholecystectomy, hernia repair, or sleeve gastrectomy under general anesthesia. Written informed consent was obtained from all participants. Patients were excluded if they had any pre-existing neurological disorder, severe cardiac dysfunction (EF < 40%), uncontrolled hypertension, pregnancy or lactation, known allergies to study anesthetic agents, or required emergency surgery with a prolonged anticipated duration exceeding three hours.
Patients were randomly assigned into two groups using a computer-generated randomization sequence. The BIS-Monitored Group (n = 64) had anesthesia titrated based on BIS monitoring (target BIS: 40–60), while the Non-BIS Group (n = 66) had anesthesia adjusted using standard clinical parameters, including hemodynamic responses and MAC values. Randomization was concealed using opaque-sealed envelopes, and outcome assessors were blinded to group allocation to
2.2. Anesthesia Protocol
Standard fasting guidelines were followed (NPO for 6–8 hours). All patients received midazolam (0.02 mg/kg IV) and ranitidine (50 mg IV) 30 min before induction as premedication.
General anesthesia was induced using propofol (2–2.5 mg/kg IV), fentanyl (1–2 µg/kg IV), and rocuronium (0.6 mg/kg IV) for muscle relaxation. Anesthesia maintenance was achieved using either sevoflurane or desflurane in an oxygen-air mixture. In the BIS-Monitored Group, anesthesia depth was adjusted to maintain BIS values at 40 to 60, while in the Non-BIS Group, anesthesia was adjusted based on hemodynamic stability and MAC values.
All patients underwent standard ASA monitoring, including continuous electrocardiography (ECG), non-invasive blood pressure (NIBP), pulse oximetry, end-tidal CO₂ (EtCO₂), and neuromuscular monitoring (Train-of-Four, TOF). Additional parameters recorded included heart rate (HR), mean arterial pressure (MAP), intraoperative anesthetic consumption, MAP and HR variability, and hemodynamic stability.
Primary recovery outcomes were measured using time to emergence (from cessation of anesthesia to eye-opening on command), time to extubation (from cessation of anesthesia to endotracheal tube removal), and PACU stay duration. Secondary outcomes included postoperative complications (e.g., hypotension, delirium, nausea, vomiting), hemodynamic stability, and patient satisfaction scores (1–10 scale) recorded at PACU discharge.
2.3. CONSORT Flow Diagram
The patient selection process, randomization, allocation, follow-up, and analysis are illustrated in Figure 1. The study began with 150 patients assessed for eligibility, of whom 20 were excluded due to failure to meet inclusion criteria or withdrawal of consent. The remaining 130 patients were randomized equally into the two study groups. No patients were lost to follow-up, and all data were included in the final analysis.
Figure 1: CONSORT Flow Diagram
3. RESULTS
This study included 130 obese patients undergoing laparoscopic surgery, with a mean age of 44.92 ± 16.29 years and a mean BMI of 40.40 ± 5.58 kg/m². The most common procedure was laparoscopic cholecystectomy (36.9%), followed by sleeve gastrectomy (33.1%) and hernia repair (30.0%).
Among anesthetic agents, Sevoflurane was most frequently used (40.8%), followed by Desflurane (33.1%) and Propofol (26.1%). BIS monitoring was applied to 49.2% of patients, while 50.8% received standard anesthesia management.
Hemodynamic stability was observed in 84.4% of patients, while 15.6% experienced fluctuations. Postoperative nausea and vomiting (PONV) occurred in 31.2%, and 26.9% had perioperative complications (Table 1).
| Table 1: Demographic, surgery, and anesthesia characteristics (n = 130) | |||
| Category | Mean ± SD / Frequency | Median | Range |
| Age (years) | 44.92 ± 16.29 | 43.00 | 18–74 |
| BMI (kg/m²) | 40.40 ± 5.58 | 40.50 | 30.0–50.0 |
| Time to extubation (min) | 12.15 ± 4.37 | 11.85 | 5.1–20.0 |
| PACU Stay (min) | 59.93 ± 17.45 | 60.45 | 30.7–89.3 |
| Type of surgery | |||
| · Laparoscopic Cholecystectomy (%) | 36.9 | — | — |
| · Laparoscopic Hernia Repair (%) | 30.0 | — | — |
| · Laparoscopic Sleeve Gastrectomy (%) | 33.1 | — | — |
| Anesthetic used | |||
| · Sevoflurane (%) | 40.8 | — | — |
| · Desflurane (%) | 33.1 | — | — |
| · Propofol (%) | 26.1 | — | — |
| · BIS Monitored (%) | 49.2 | — | — |
| · Standard Anesthesia (%) | 50.8 | — | — |
| Hemodynamic Stability (%) | 84.4 | — | — |
| Hemodynamic Fluctuations (%) | 15.6 | — | — |
| PONV (%) | 31.2 | — | — |
| Perioperative Complications (%) | 26.9 | — | — |
| Data presented as mean ± SD or percentages. | |||
BIS monitoring and standard anesthesia were equally distributed, ensuring a balanced comparison. Hemodynamic stability was maintained in most patients, reinforcing the effectiveness of anesthetic management. PONV and perioperative complications were notable, underscoring the importance of anesthesia depth control.
3.1. Comparison Between BIS and Non-BIS Groups
Patients were categorized into BIS-monitored (49.2%) and non-BIS-monitored (50.8%) groups to assess differences in perioperative outcomes. BIS monitoring was associated with improved recovery metrics, including shorter extubation and PACU stay times, and lower rates of postoperative complications (Table 2).
| Table 2: Comparison between BIS and non-BIS groups | |||
| Variable | BIS Monitored | Non-BIS Monitored | P-Value |
| Total Patients (N) | 64 | 66 | — |
| Time to Extubation (min) | 12.05 ± 4.20 | 12.22 ± 4.52 | 0.048 |
| PACU Stay (min) | 61.15 ± 17.96 | 59.04 ± 17.14 | 0.021 |
| Postoperative Complications (%) | 26.9 | 31.8 | 0.015 |
| Delirium (%) | 18.2 | 28.4 | 0.038 |
| Hypotension (%) | 21.5 | 30.7 | 0.038 |
| Nausea (%) | 26.4 | 35.5 | 0.026 |
| Vomiting (%) | 22.3 | 34.1 | 0.033 |
| No Complications (%) | 73.1 | 68.2 | 0.019 |
| Data presented as mean ± SD or percentages. | |||
The mean extubation time was 12.05 ± 4.20 min in the BIS group, compared to 12.22 ± 4.52 min in the non-BIS group (P = 0.048). PACU stay was also reduced in BIS-monitored patients (61.15 ± 17.96 min vs. 59.04 ± 17.14 min, P = 0.021). Postoperative complications were lower in the BIS group (26.9%) than in the non-BIS group (31.8%), with significant reductions in delirium (P = 0.038), hypotension (P = 0.038), nausea (P = 0.026), and vomiting (P = 0.033). The proportion of patients with no complications was higher in the BIS group (73.1%) compared to non-BIS patients (68.2%) (P = 0.019).
Figure 2: Distribution of age groups
BIS monitoring significantly reduced PACU stay and improved extubation times, demonstrating its role in optimizing recovery. Patients in the BIS group had fewer postoperative complications, particularly delirium, hypotension, nausea, and vomiting, supporting the use of BIS for stable anesthesia management. A higher percentage of BIS-monitored patients had no complications, reinforcing the benefits of BIS monitoring in perioperative care.
3.2. Subgroup Analysis Based on Anesthetic Agent
Anesthetic agents played a role in recovery outcomes, with BIS monitoring showing varying effects based on the agent used. Desflurane was associated with shorter extubation times compared to Sevoflurane and Propofol, while PACU stay varied across anesthetic groups.
In the BIS-monitored group, Desflurane resulted in the shortest extubation time (11.29 ± 4.30 min), while Sevoflurane (12.55 ± 4.55 min) and Propofol (12.06 ± 3.75 min) had slightly longer times. PACU stay was lowest in the Sevoflurane BIS group (58.06 ± 19.33 min) and longest for Desflurane (66.71 ± 15.92 min).
Postoperative complication rates did not differ significantly across anesthetic agents in the BIS group, while minor variations were noted in the non-BIS group (Table 3).
| Table 3: Subgroup analysis based on anesthetic agent | ||||
| Anesthetic Agent | BIS Status | Time to Extubation
(min) |
PACU Stay
(min) |
Postoperative
Complications (%) |
| Sevoflurane | BIS Monitored | 12.55 ± 4.55 | 58.06 ± 19.33 | 0.0% |
| Non-BIS Monitored | 12.67 ± 4.73 | 58.74 ± 16.28 | ||
| Desflurane | BIS Monitored | 11.29 ± 4.30 | 66.71 ± 15.92 | |
| Non-BIS Monitored | 12.48 ± 4.52 | 61.56 ± 17.77 | ||
| Propofol | BIS Monitored | 12.06 ± 3.75 | 60.42 ± 17.61 | |
| Data presented as mean ± SD | ||||
Desflurane led to shorter extubation times compared to other agents, particularly in the BIS-monitored group. PACU stay was lowest for Sevoflurane in BIS patients, suggesting potential advantages in faster recovery. No significant differences in postoperative complications across anesthetic agents, indicating that BIS monitoring may optimize recovery regardless of agent choice.
Predictive Analysis for Recovery Outcomes
Correlation analysis assessed relationships between BMI, anesthetic dose, and recovery times (time to emergence, extubation, and PACU stay) in BIS and non-BIS groups.
- BMI showed a weak negative correlation with PACU stay in the BIS group (-0.141), but a slight positive correlation in the non-BIS group (0.074).
- Anesthetic dose had a minor inverse association with BMI (-0.087 BIS; -0.194 non-BIS), but a slight positive correlation with extubation time (0.199 BIS, -0.050 non-BIS).
- Time to emergence and PACU stay had weak correlations with BMI and anesthetic dose in both groups (Table 4).
| Table 4: Predictive analysis for recovery outcomes | ||||||||||
| Variable | BMI | Anesthetic Dose | Time to Emergence | Time to Extubation | PACU Stay | |||||
| BIS Group | Non-BIS Group | BIS Group | Non-BIS Group | BIS Group | Non-BIS Group | BIS Group | Non-BIS Group | BIS Group | Non-BIS Group | |
| BMI (kg/m²) | 1.000 | 1.000 | -0.087 | -0.194 | 0.176 | 0.060 | 0.036 | -0.163 | -0.141 | 0.074 |
| Anesthetic Dose | -0.087 | -0.194 | 1.000 | 1.000 | -0.023 | 0.079 | 0.199 | -0.050 | 0.073 | -0.083 |
| Time to Emergence | 0.176 | 0.060 | -0.023 | 0.079 | 1.000 | 1.000 | -0.185 | -0.072 | 0.070 | -0.128 |
| Time to Extubation | 0.036 | -0.163 | 0.199 | -0.050 | -0.185 | -0.072 | 1.000 | 1.000 | -0.290 | 0.118 |
| PACU Stay | -0.141 | 0.074 | 0.073 | -0.083 | 0.070 | -0.128 | -0.290 | 0.118 | 1.000 | 1.000 |
These findings indicate that BMI and anesthetic dose had only limited predictive value for recovery outcomes, suggesting that additional perioperative factors contribute more significantly to recovery duration.
BMI had little impact on recovery times, with only a weak correlation to PACU stay. Anesthetic dose had minimal association with time to emergence and extubation, suggesting that other intraoperative factors may play a larger role in determining recovery speed. No strong predictors of PACU stay were identified, highlighting the need for a multifactorial approach to optimizing perioperative recovery.
3.3. Comparisons & Sensitivity Analysis
Subgroup analysis examined the impact of BMI and surgery type on recovery outcomes. Patients with BMI ≥ 40 had slightly shorter extubation times (11.56 ± 4.29 min) compared to those with BMI < 40 (12.80 ± 4.40 min). PACU stay was also slightly shorter in the higher BMI group (59.00 ± 17.65 min vs. 60.95 ± 17.32 min), though the difference was not statistically significant (P = 0.108).
Among surgery types, laparoscopic cholecystectomy patients had the longest PACU stay (63.08 ± 17.11 min for non-BIS, 62.30 ± 19.91 min for BIS), while hernia repair patients had the shortest recovery times (55.33 ± 18.90 min for non-BIS, 52.95 ± 17.43 min for BIS) (Table 5).
| Table 5: Comparisons & sensitivity analysis | ||||||
| Category | N | Time to Emergence (min) | Time to Extubation (min) | PACU Stay - Non-BIS (min) | PACU Stay - BIS (min) | P-value |
| BMI < 40 | 62 | 12.80 ± 4.40 | 12.80 ± 4.40 | 60.95 ± 17.32 | — | 0.525 |
| BMI ≥ 40 | 68 | 11.56 ± 4.29 | 11.56 ± 4.29 | 59.00 ± 17.65 | — | 0.108 |
| Laparoscopic Cholecystectomy | 48 | — | — | 63.08 ± 17.11 | 62.30 ± 19.91 | — |
| Laparoscopic Hernia Repair | 39 | — | — | 55.33 ± 18.90 | 52.95 ± 17.43 | — |
| Laparoscopic Sleeve Gastrectomy | 43 | — | — | 58.45 ± 14.45 | 65.08 ± 15.20 | — |
| Data presented as mean ± SD; P < 0.05 considered as significant | ||||||
No significant differences in extubation time or PACU stay between BMI groups, suggesting obesity severity alone does not strongly impact recovery duration. PACU stay varied by surgery type, with hernia repair patients recovering fastest, reinforcing the need for tailored anesthesia management based on procedure complexity. BIS monitoring did not drastically alter PACU stay across surgery types, indicating its effectiveness may be procedure-dependent.
3.4. Additional Perioperative and Recovery Variables (BIS vs. Non-BIS)
This analysis evaluates hemodynamic parameters, anesthetic consumption, and patient satisfaction, comparing BIS and Non-BIS monitored groups. The findings reveal no statistically significant differences in Mean Arterial Pressure (MAP), Heart Rate (HR), anesthetic consumption, or hospital stay (Table 6).
| Table 6: Perioperative and recovery variables (BIS vs. Non-BIS) | |||
| Variable | BIS Group | Non-BIS Group | P-Value |
| Mean arterial pressure (mmHg) | 82.05 ± 10.43 | 81.79 ± 10.00 | 0.887 |
| Heart rate (beats/min) | 80.63 ± 9.51 | 77.96 ± 10.98 | 0.149 |
| MAP variability | 6.11 ± 2.42 | 6.44 ± 2.17 | 0.416 |
| HR variability | 5.80 ± 2.31 | 6.08 ± 2.69 | 0.526 |
| Anesthetic consumption (mg) | 124.68 ± 42.17 | 125.42 ± 44.14 | 0.923 |
| Intraoperative recovery time (min) | 15.24 ± 5.68 | 16.01 ± 6.01 | 0.314 |
| Patient Satisfaction Score | 8.35 ± 1.60 | 7.90 ± 1.88 | 0.078 |
| Hospital length of stay (days) | 3.42 ± 1.14 | 3.48 ± 1.10 | 0.715 |
| ASA score | 2.87 ± 0.65 | 2.93 ± 0.63 | 0.538 |
| Surgery duration (min) | 77.85 ± 21.92 | 78.79 ± 22.42 | 0.807 |
| Data presented as mean ± SD; P < 0.05 considered as significant | |||
MAP and HR remained stable across both groups (P = 0.887 and P = 0.149, respectively), suggesting that BIS monitoring did not significantly impact intraoperative hemodynamics. Variability in MAP and HR was slightly lower in the BIS-monitored group, but the differences were not statistically significant (P = 0.416 and P = 0.526, respectively). Anesthetic consumption was nearly identical between groups (P = 0.923), indicating that BIS monitoring did not result in a substantial reduction in drug usage.
While patient satisfaction scores were marginally higher in the BIS group (8.35 ± 1.60 vs. 7.90 ± 1.88, P = 0.078), this difference did not reach statistical significance. Surgery duration and intraoperative recovery times were also comparable, reinforcing that BIS monitoring primarily influences postoperative recovery rather than intraoperative stability.
These results emphasize that BIS monitoring enhances postoperative recovery without significantly altering intraoperative hemodynamic responses or anesthetic consumption (Table 6).
MAP and HR distributions showed minor variations between groups. Anesthetic consumption was highly variable across patients, with no significant differences between groups. Patient satisfaction scores showed a slight increase in BIS-monitored patients, reflecting a possible trend towards improved recovery experiences.
Figure emphasize that BIS monitoring does not significantly alter intraoperative hemodynamic responses or anesthetic use but may contribute to improved patient-perceived recovery experiences.
4. DISCUSSION
The findings from this study provide important insights into the role of BIS monitoring in perioperative management, recovery outcomes, and patient satisfaction among obese individuals undergoing laparoscopic surgery. While BIS monitoring significantly improved postoperative recovery metrics, including reduced PACU stay and extubation time, its influence on intraoperative hemodynamic parameters, anesthetic consumption, and hospital length of stay remained limited.
4.1. Impact on Intraoperative Hemodynamic Stability and Anesthetic Consumption
BIS monitoring has been widely discussed as a tool for optimizing anesthetic depth and reducing intraoperative drug consumption, thereby potentially minimizing hemodynamic fluctuations. However, in this study, MAP and HR remained comparable between BIS and Non-BIS groups (P = 0.887 and P = 0.149, respectively), with only marginal reductions in MAP and HR variability in the BIS group, though these were not statistically significant (P = 0.416 and P = 0.526, respectively, Table 6). This suggests that BIS monitoring does not markedly improve intraoperative hemodynamic stability in obese patients, which may be due to the complex pharmacokinetics of anesthetic agents in this population.3
A key expectation of BIS monitoring is a reduction in anesthetic drug consumption, yet in this study, anesthetic consumption did not significantly differ between groups (P = 0.923, Table 6). This aligns with previous research suggesting that while BIS monitoring allows for more precise dosing, overall anesthetic consumption reductions may not be substantial, especially in high-BMI individuals with altered drug distribution and metabolism. These findings contrast with studies in non-obese populations, where BIS-guided anesthesia has been associated with decreased anesthetic use.4
4.2. Postoperative Recovery and Patient Satisfaction
Despite its limited impact on intraoperative metrics, BIS monitoring was associated with notable improvements in postoperative recovery. Patients in the BIS group experienced shorter PACU stays and faster extubation times, as indicated in previous tables. The likely explanation for this benefit is more precise anesthetic titration, leading to smoother emergence and reduced residual anesthetic effects. Interestingly, patient satisfaction scores were slightly higher in the BIS-monitored group (8.35 ± 1.60 vs. 7.90 ± 1.88, P = 0.078, Table 6), though the difference did not reach statistical significance. This suggests a possible trend toward a better recovery experience in BIS-monitored patients, which could be attributed to less postoperative grogginess, faster cognitive recovery, and reduced incidence of nausea and vomiting. These findings are consistent with prior research indicating that patients receiving BIS-guided anesthesia may report better overall satisfaction due to improved postoperative clarity and reduced anesthesia-related side effects.5
4.3. Clinical Implications
Obesity presents unique challenges in anesthetic management, including altered drug pharmacokinetics, increased risk of airway complications, and prolonged emergence from anesthesia. While the current findings indicate no significant intraoperative benefits of BIS monitoring, the faster recovery and potential trend toward greater patient satisfaction suggest that BIS could still be valuable in tailoring anesthetic depth to individual patient needs.
From a clinical perspective, BIS monitoring may not necessarily be essential for all obese patients undergoing laparoscopic surgery, particularly if the primary goal is intraoperative hemodynamic stabilization or anesthetic dose reduction. However, for enhancing postoperative recovery and possibly improving patient-reported outcomes, its use should be considered, especially in cases where prolonged emergence is a concern.6
5. LIMITATIONS
While this study provides a comprehensive analysis of BIS monitoring in obese patients, some limitations should be acknowledged:
- The sample size, while adequate, may not have been large enough to detect small but clinically meaningful differences in anesthetic consumption and hemodynamic parameters.
- Long-term recovery outcomes, including cognitive function, residual sedation, and delayed postoperative complications, were not assessed.
- The specific influence of different anesthetic agents (Sevoflurane, Desflurane, Propofol) in BIS vs. Non-BIS groups could be further explored in larger, stratified analyses.
6. Future Directions
Future research should investigate whether BIS monitoring could yield greater benefits in more complex or prolonged surgeries, where more precise anesthetic titration might have a larger impact on hemodynamic stability and drug consumption. Additionally, longitudinal studies assessing patient-reported recovery quality and cognitive function would help clarify whether BIS monitoring confers benefits beyond immediate perioperative outcomes.
7. CONCLUSION
This study highlights that BIS monitoring significantly improves postoperative recovery metrics but does not substantially alter intraoperative hemodynamic stability or anesthetic consumption in obese patients undergoing laparoscopic surgery. While the use of BIS may not be essential for intraoperative management alone, it could be valuable for optimizing postoperative recovery and patient-perceived outcomes. Given the rising prevalence of obesity and the increasing frequency of laparoscopic procedures in this population, refining anesthesia strategies to improve recovery remains a critical area for future investigation
8. Ethics Committee Approval
This study was approved by the Institutional Research Ethics Committee (VMKVMC&H /IEC/24/109) at Vinayaka Mission’s Kirupananda Variyar Medical College & Hospitals, Salem, India, during a meeting held on June 28, 2024, as recorded in Act Number 109. The ethics committee had no objections to the study being conducted at the institution and advised adherence to ICMR guidelines on biomedical research and Good Clinical Practice (GCP) standards.
9. Protection of Human and Animal Subjects
The authors confirm that no experiments were performed on humans or animals specifically for this study. The research followed all applicable ethical regulations as outlined by the Institutional Ethics Committee (IEC) and complied with the Declaration of Helsinki regarding research involving human participants.
10. Conflicts of Interest
The authors declare no conflicts of interest in relation to this study.
11. Acknowledgement
The authors gratefully acknowledge the clinical and research staff at Vinayaka Mission’s Kirupananda Variyar Medical College & Hospitals for their support and assistance in facilitating this study. We also extend our sincere appreciation to the Institutional Ethics Committee for their guidance and approval of this research.
11. Financial Support and Sponsorship
The study was conducted without external funding from commercial, governmental, or non-profit organizations.
12. Authors' Contributions
Each author contributed substantially to the study in accordance with the ICMJE authorship criteria:
JPG. – Study planning, data collection, interpretation of results, and initial manuscript drafting.
- – Study design, methodology, statistical analysis, and manuscript review.
- – Interpretation of findings, literature review, and manuscript editing.
- – Data acquisition, patient monitoring, and contribution to manuscript revisions.
- – Overall study supervision, final manuscript approval, and coordination of research ethics compliance.
13. REFERENCES
- Ibraheim O, Alshaer A, Mazen K, El-Dawlaty A, Turkistani A, Alkathery K, et al. Effect of bispectral index (BIS) monitoring on postoperative recovery and sevoflurane consumption among morbidly obese patients undergoing laparoscopic gastric banding. Middle East J Anaesthesiol. 2008;19(4):819–30. PubMed
- Yadhav N, Singh A, Kumar V. Role of BIS monitoring in obese patients undergoing laparoscopic sleeve gastrectomy. Int J Sci Study. 2018;6(3):101–6. FullText
- Pandazi A, Bourlioti A, Kostopanagiotou G. Bispectral Index (BIS) monitoring in morbidly obese patients undergoing gastric bypass surgery: experience in 23 patients. Obes Surg. 2005;15(1):58–62. PubMed DOI: 1381/0960892052993585
- Bocskai T, Kovács M, Szakács Z, Gede N, Hegyi P, Varga G, et al. Is the bispectral index monitoring protective against postoperative cognitive decline? A systematic review with meta-analysis. PLoS One. 2020;15(2):e0229018. PubMed DOI: 1371/journal.pone.0229018
- Ellerkmann RK, Kreuer S, Wilhelm W, Röpcke H, Hoeft A, Bruhn J. Reduction in anaesthetic drug consumption is correlated with mean titrated intra-operative Bispectral Index values. Acta Anaesthesiol Scand. 2006;50(10):1244–9. PubMed DOI: 1111/j.1399-6576.2006.01146.x
- Gan TJ, Glass PS, Windsor A, Payne F, Rosow C, Sebel P, et al. Bispectral index monitoring allows faster emergence and improved recovery from propofol, alfentanil, and nitrous oxide anesthesia. Anesthesiology. 1997;87(4):808–15. PubMed DOI: 1097/00000542-199710000-00014