Hanaa Elfeky 1 , Rabab Habeeb 2*, Ahmed Omran 3
Authors affiliations:
Background & objective: Effective pain relief during labor enhances maternal comfort, in addition to improving maternal and fetal outcomes. Various techniques of administering epidural analgesia include single bolus epidural analgesia, continuous epidural infusion, Patient-Controlled Epidural Analgesia (PCEA), Programmed Intermittent Epidural Bolus (PIEB), and PCEA with background infusion. Nulliparous and multiparous women exhibit distinct responses to labor pains. We compared the efficacy of PIEB in both multiparous and nulliparous participants.
Methodology: 30 patients undergoing normal vaginal delivery under epidural analgesia were included, and divided into two groups (15 per group), depending on whether they were nulliparous (Group N) or multiparous (Group M). All patients received PIEB in combination with PCEA. The primary outcome was to measure adequate labor analgesia using the Visual Analog Scale (VAS), the number of PCEA attempts, the volume administered via PCEA, and the timing of the first PCEA bolus. Time in the second stage of labor, and type of labor, were noted.
Results: The patients in Group N experienced greater pain from 4 to 7 hours than those in Group M, and this difference was statistically significant (P < 0.05). The mean time required to administer the first dose of PCEA bolus was significantly longer in Group M than in Group N (P = 0.0003). Similarly, Group N received significantly higher mean PCEA doses and volume of drug administered via PCEA than Group M, and the difference was significant (P < 0.0001).
Conclusion: The combination of PIEB and PCEA is an excellent method of providing labor analgesia in nulliparous as well as in multiparous women. However, nulliparous women are more likely to use top-up doses of PCEA as compared to multiparous women.
Abbreviations: PCEA: Patient-Controlled Epidural Analgesia, PIEB: Programmed Intermittent Epidural Bolus, VAS: Visual Analog Scale
Keywords: Labor Analgesia; Programmed Intermittent Epidural Bolus; Patient-Controlled Epidural Analgesia; Parity
Citation: Elfeky H, Habeeb R, Omran A. Comparative study of programmed intermittent epidural boluses (PIEB) of 10 mL bupivacaine 0.0625% plus 2 μg/mL fentanyl at 90 min intervals in nulliparous versus multiparous parturients. Anaesth. pain intensive care 2025;29(5):338-344. DOI: 10.35975/apic.v29i5.2636
Received: December 26, 2024; Revised: July 09, 2025; Accepted: July 10, 2025
Labor analgesia is vital in contemporary obstetrics due to its advantages for pregnant women and newborns. Effective pain relief during labor ensures maternal comfort and plays a pivotal role in optimizing maternal-fetal outcomes. Analgesia during labor alleviates the intense pain, allowing mothers to maintain their energy, resulting in reduced maternal exhaustion and facilitating a more efficient progression of labor.1 Consequently, this can potentially minimize the risk of prolonged labor and its associated outcomes, such as birth asphyxia in infants. Effective pain management during labor analgesia has a beneficial effect on the newborn by promoting successful breastfeeding. The occurrence of maternal pain and stress during labor can result in difficulties in breastfeeding and its subsequent consequences. Analgesia improves both maternal and fetal outcomes by alleviating maternal pain and stress.2
Labor analgesia encompasses a diverse range of options, including pharmacological methods such as epidural or spinal anesthesia, as well as non-pharmacological techniques, including relaxation, breathing exercises, or hydrotherapy.3 The availability of diverse analgesic modalities allows tailored pain management, personalized according to each woman’s specific needs and preferences, thereby enhancing the overall childbirth experience. Epidural and intrathecal blockade are two frequently employed techniques for achieving comprehensive analgesia during the initial and subsequent phases of labor. Out of these two pain management methods, epidural analgesia has been shown to offer a superior safety profile for pregnant women and newborns.4
Various epidural analgesia regimens include single bolus epidural analgesia, continuous epidural infusion, PCEA, PIEB, and PCEA with PCEA in background.5 Patient-controlled epidural analgesia is associated with improved pain management and a sense of autonomy. Multiple studies have shown numerous advantages of using the PIEB technique, which involves the automatic administration of a predetermined dose of local anesthetic drug at specific time intervals, as opposed to the continuous epidural infusion technique. The benefits include improved maternal satisfaction, decreased local anesthetic requirement, and reduced time for the second stage of labor. Furthermore, it is linked to a reduced likelihood of instrumental deliveries.6
Childbirth entails inevitable pain, which often instills a profound sense of fear in many women, particularly nulliparous women.7 The severity as well as perception of labor pain experienced by nulliparous and multiparous women vary significantly. Nulliparous women have a higher likelihood of experiencing fear related to the pain of childbirth, whereas multiparous women are less apprehensive.8 Moreover, in nulliparous women, more significant pain is experienced during the early phase of labor, whereas in multiparous women, more intense pain is experienced during the pelvic phase due to the rapid descent of the fetus. Nevertheless, it is crucial to recognize that parity is not a decisive factor in determining the need for labor analgesia, which should be offered to all women during childbirth.9
This comparative study aimed to analyze the effectiveness of PIEB interval 90 (EI90) of 10 ml 0.0625% bupivacaine and 2 μg/mL fentanyl in nulliparous versus multiparous parturient.
This prospective comparative study was conducted in the Anesthesiology Department at Menoufia University over a 1-year period, from November 2022 to November 2023, after approval of the local ethical committee Menoufia University Faculty of Medicine Research Ethical Committee date and number 10/2022ANET1-1 chairperson Professor Walaa Farid and ClinicalTrials.gov ID: NCT05441085. The study included a cohort of 30 patients who were undergoing routine vaginal delivery and receiving epidural analgesia. The selection of these patients was based on pre-established criteria for inclusion and exclusion. The patients received a detailed explanation of the nature of the study, and written consent was obtained from all participants.
The sample size was determined by analyzing previous literature (Laura et al., 2018), which revealed that nulliparous women experienced labor pain for a significantly longer duration compared to multiparous women. The nulliparous women gave birth 9.3 hours after the debut of pain (95%CI:8.11–13.25). In contrast, the multiparous women delivered 8.1 hours after the debut of pain (95%CI:2.25–9.22).10 The minimum sample size was calculated using statistics, and sample size provision 6 was 30 subjects divided into two equal groups. The power of the study is 80%, and the confidence level is 95%. Consequently, 30 patients were included, with 15 patients in each of the two groups. For the purpose of comparison, the patients were categorized into the following groups: Group N compromised 15 nulliparous women receiving epidural analgesia for labor pain, whereas Group M included 15 multiparous women receiving epidural analgesia for labor pain.
Inclusion criteria: Participants who provided informed written consent, pregnant women in the initial stage of labor, with a gestational age of more than 37 weeks, experiencing regular contractions every 5 min, and cervical dilation between 2 and 5 cm, as well as patients classified as American Society of Anaesthesiologists (ASA) II and III. Exclusion criteria: Individuals who refused to provide consent for participation, contraindications to epidural analgesia, and known allergy to bupivacaine or fentanyl. Patients who received opioid analgesic or sedatives within 4 hours prior to epidural insertion, inadvertent dural puncture, patients who delivered within 1 hour or failed to achieve a VAS score less than two after the initiation of an epidural clinician bolus.
Baseline measurements, including pulse rate, blood pressure, and oxygen saturation, were recorded for all participants. A 500 mL infusion of Ringer’s lactate as pre-load was initiated. The patient was positioned in a seated posture, and an epidural catheter was inserted using an 18-G Tuohy needle, following skin sterilization with a 2% chlorhexidine in 70% alcohol solution. The loss-of-resistance technique was employed with either air or saline. A 19-G multi-orifice wire-reinforced catheter (Arrow Flextip plus; Arrow International Inc., Reading, PA, USA) was then inserted 5 cm into the epidural space. Aspiration was conducted to ensure the absence of blood or cerebrospinal fluid.
Initially, a preliminary dose of 0.125% bupivacaine 3 mL with fentanyl 3.3 μg/mL was administered. After three minutes, a loading dose consisting of 2 boluses of bupivacaine 0.125% 6 mL with fentanyl 3.3 μg/mL was injected, with a three-minute interval between them. This loading dose was followed by a maintenance dose comprising bupivacaine 0.0625% with fentanyl 2 μg/mL, where the initial Patient-Initiated Epidural Bolus (PIEB) interval time was set at 60 min. The system was additionally programmed with PCEA settings to give 10 mL of the same local anesthetic solution with a lockout period of 10 min. Maximum total volume was set to 30 mL/hr, including the PIEB and the PCEA. Patients were instructed to push the PCEA switch if they found contractions to be uncomfortable.
The primary outcomes in the present study were the labor pain severity assessed by the VAS score, the number of PCEA attempts, the volume administered via PCEA, and the timing of the first PCEA bolus. The hemodynamic parameters were monitored. The time spent in the second stage of labor, type of labor, and incidence of adverse effects were also compared.
Statistical analysis
Statistical analysis was done with the help of IBM SPSS 23.0. Descriptive statistics were employed, continuous variables are presented as mean and standard deviation, whereas categorical data are presented as frequencies and percentages. The study groups are compared using independent t-tests for continuous data and chi-square tests for categorical data analysis. P < 0.05 is taken to be statistically significant.
This study involved 39 patients who were undergoing normal vaginal delivery and receiving epidural analgesia. After exclusion of patients who didn’t meet inclusion criteria or refused to participate in the study, 36 patients were selected. After taking full obstetric history they were subdivided into two groups; Group M (multipara) (n = 19) and Group N (nullipara) (n = 17). Six patients experienced failed vaginal delivery and underwent C-section leaving 15 patients in each group. The groups were compared for mean age, weight, and ASA Grades. The mean age of the patients in Group N was less than that of those in Group M, and this difference was significant (P = 0.011). The mean weight and ASA grades were comparable in both groups (Table I).
The groups were compared for pregnancy characteristics and comorbidities. Both groups were comparable in prevalence of gestational diabetes and pre-eclampsia (P > 0.05). The mean Gestational age of patients in Group N and Group M was 38.94 ± 1.24 and 38.12 ± 1.34 weeks. The gestational age in both the groups was comparable (P = 0.09) (Table 1).
The comparison of patients for induction and augmentation of labor showed both groups to be comparable (P > 0.05). Assisted vaginal delivery was done in 4 (26.67%) patients in Group N and 2 (13.33%) patients in Group M. Need for assisted delivery was more in Group N as compared to Group M. However, the difference was not statistically significant (P > 0.05). Duration of the first and second stages of labor was more in Group N patients than in Group M (P < 0.0001) (Table 1).
The pain intensity of the patients in both groups was assessed by calculating the mean VAS scores at various time intervals following the onset of labor. While the pain experienced by patients in Group N was more severe compared to patients in Group M, it was equivalent to a duration of 3 hours. Between 4th and 7th hours, Group N patients experienced a higher level of pain intensity than Group M patients, and this difference was found to be statistically significant (P < 0.05). The pain intensity between the two groups was comparable from 8 to 12th hours (P > 0.05), as shown in Table 2.
The average duration for the first PCEA bolus in Group N and Group M was 94 ± 18 and 124 ± 22 minutes, respectively. The mean duration was more significant in Group M compared to Group N, and this difference was statistically significant (P = 0.0003). Group N had significantly higher mean PCEA doses and volume of drug administered compared to Group M (P < 0.0001), as illustrated in Table 3.
The average heart rate in Group N and Group M was determined to be 79.73 ± 3.12 and 78.24 ± 2.60, respectively. Both groups’ mean heart rates and mean arterial pressures were comparable (P > 0.05; Figure 1).
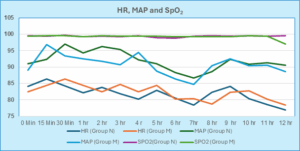
Figure 1: Comparison of Mean Heart Rate, MAP and SpO2 in groups
Both groups were compared on the basis of adverse events. In Group N and M 5 (33.33%) and 4 (26.66%) patients developed adverse events. In Group N, three patients (20%) developed tachycardia whereas 1 (6.66%) patient in Group M developed bradycardia. Pruritis was detected in two patients (13.33%) of Group N and 3 (20%) patients of Group M. The analysis of adverse events in both groups showed that the incidence of adverse events was comparable in both groups (Figure 2).
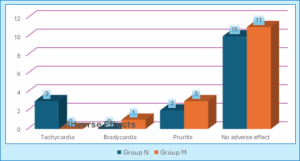
Figure 2: Comparison of adverse effects in both the cases
Effective and safe analgesia is crucial for the successful management of patients in labor. It ensures that the expulsive efforts required for labor progress are preserved. In recent times, epidural analgesia become increasingly popular for labor analgesia, and several studies have established its effectiveness.11 In this study, we aimed to compare the efficacy of epidural analgesia in both nulliparous and multiparous women. Our comparative analysis revealed that patients in both groups were comparable in terms of demographic characteristics, ASA Grades, and the prevalence of pre-eclampsia and gestational diabetes. However, when considering the type of delivery, it was observed that the need for assisted delivery was slightly lower in Group M compared to Group N. However, this difference was not statistically significant (P > 0.05). Moreover, the duration of the first and second stages of labor was considerably longer in Group N than in Group M (P < 0.0001).
A study by Jardine et al. (2020) aimed to determine the rate of complicated births in nulliparous as well as multiparous women, analyzing maternity records of 276,766 women having singleton pregnancies.12 In this study, authors defined complicated delivery as birth associated with the use of instruments, cesarean section, perineal tears, postpartum hemorrhage, or an Apgar score of 7 or less than 7 at five minutes. This study revealed a notably higher risk of instrumental delivery in nulliparous cases compared to multiparous women, which is similar to our findings. Likewise, a similar increased risk of instrumental deliveries in nulliparous women was also reported by Mazouni C et al. (2006) and Wassen MM et al. (2011).13,14
Although pain is an unavoidable aspect of labor, it is important to acknowledge that the experience of labor pain varies in nulliparous women. Multiparous women typically exhibit more severe pain and a greater fear of pain compared to multiparous women. In our study, the comparison of pain severity assessed by VAS scores showed that pain levels were comparable in both groups for the first three hours from the start of labor. During the period from the fourth to the seventh hour, patients in Group N experienced more intense pain compared to those in Group M, and this difference was found to be statistically significant (P < 0.05). Between the eighth and the twelfth hour postpartum, the severity of pain was comparable in both groups (P > 0.05).
In a study by Fridh et al., the authors explored background factors, emotional feelings, and mothers’ expectations concerning pain intensity during labor. They found that parity, young age, lower educational qualification, history of menstrual irregularity, previous abortion, emotional instability, and unrealistic expectations of labor pain were associated with increased pain intensity during labor.15 Similar factors affecting the intensity of labor pain were also reported in studies done by Sheiner E et al. (1998) and Labor S et al. (2008).16,17
In our study, epidural analgesia was administered using PIEB and PCEA. A comparison of patients based on the meantime for the 1st PCEA bolus showed that the mean time was 94 ± 18 minutes in Group N and 124 ± 22 min in Group M. The mean time was shorter in Group N compared to Group M, and this difference was highly statistically significant (P = 0.0003). Similarly, mean PCEA doses and the volume of drugs administered via PCEA were greater in Group N compared to Group M, and this difference was statistically significant (P < 0.0001). Notably, there is limited research on the differences in drug requirement during epidural analgesia between nulliparous and multiparous women. However, Malevic et al. (2019) discovered notable variations in the preferences for pain relief methods between primiparous and multiparous women.18 Epidural analgesia was preferred by primiparous women, while delivery without any analgesia was more common among multiparous women. These findings are consistent with our study in terms of the effectiveness of epidural analgesia during labor. Studies by Halpern et al. (2010) and Agrawal D et al. (2014) have reported similar conclusions in their studies.19,20
The patient groups experienced minor adverse effects, such as transient tachycardia, bradycardia, and pruritus. The incidence of adverse effects in both groups was similar statistically (P > 0.05).
Besides a small sample size, one limitation of the study was that the patients were instructed to administer a dose of PCEA based on their own perception of discomfort, which is a subjective criterion.
PIEB combined with PCEA is an excellent method of providing labor analgesia in nulliparous as well as multiparous women. Nulliparous women are more likely to use top-up doses of PCEA as compared to multiparous women. However, more studies are required to determine The EI 90 for multiparous patients.
7. Data availability
The numerical data generated during this research is available with the authors.
8. Conflict of interest
All authors declare that there was no conflict of interest.
9. Funding
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Authors’ contribution
Both authors took equal part in the concept, study design, conduct of study, literature search and manuscript preparation.
Authors affiliations:
- Hanaa Elfeky, Department of Anesthesia & Intensive Care, Faculty of Medicine, Menoufia University, Menoufia, Egypt; Email: hanaafotoh@yahoo.com
- Rabab Habeeb, Department of Anesthesia & Intensive Care, Faculty of Medicine, Menoufia University, Menoufia, Egypt; Email: Rabab_habeeb@med.menofia.edu.eg
- Ahmed Omran, Department of Anesthesia & Intensive Care, Faculty of Medicine, Ain Shams University, Cairo, Egypt; Email; ahmed.omran@med.asu.edu.eg
ABSTRACT
Background & objective: Effective pain relief during labor enhances maternal comfort, in addition to improving maternal and fetal outcomes. Various techniques of administering epidural analgesia include single bolus epidural analgesia, continuous epidural infusion, Patient-Controlled Epidural Analgesia (PCEA), Programmed Intermittent Epidural Bolus (PIEB), and PCEA with background infusion. Nulliparous and multiparous women exhibit distinct responses to labor pains. We compared the efficacy of PIEB in both multiparous and nulliparous participants.
Methodology: 30 patients undergoing normal vaginal delivery under epidural analgesia were included, and divided into two groups (15 per group), depending on whether they were nulliparous (Group N) or multiparous (Group M). All patients received PIEB in combination with PCEA. The primary outcome was to measure adequate labor analgesia using the Visual Analog Scale (VAS), the number of PCEA attempts, the volume administered via PCEA, and the timing of the first PCEA bolus. Time in the second stage of labor, and type of labor, were noted.
Results: The patients in Group N experienced greater pain from 4 to 7 hours than those in Group M, and this difference was statistically significant (P < 0.05). The mean time required to administer the first dose of PCEA bolus was significantly longer in Group M than in Group N (P = 0.0003). Similarly, Group N received significantly higher mean PCEA doses and volume of drug administered via PCEA than Group M, and the difference was significant (P < 0.0001).
Conclusion: The combination of PIEB and PCEA is an excellent method of providing labor analgesia in nulliparous as well as in multiparous women. However, nulliparous women are more likely to use top-up doses of PCEA as compared to multiparous women.
Abbreviations: PCEA: Patient-Controlled Epidural Analgesia, PIEB: Programmed Intermittent Epidural Bolus, VAS: Visual Analog Scale
Keywords: Labor Analgesia; Programmed Intermittent Epidural Bolus; Patient-Controlled Epidural Analgesia; Parity
Citation: Elfeky H, Habeeb R, Omran A. Comparative study of programmed intermittent epidural boluses (PIEB) of 10 mL bupivacaine 0.0625% plus 2 μg/mL fentanyl at 90 min intervals in nulliparous versus multiparous parturients. Anaesth. pain intensive care 2025;29(5):338-344. DOI: 10.35975/apic.v29i5.2636
Received: December 26, 2024; Revised: July 09, 2025; Accepted: July 10, 2025
1. INTRODUCTION
Labor analgesia is vital in contemporary obstetrics due to its advantages for pregnant women and newborns. Effective pain relief during labor ensures maternal comfort and plays a pivotal role in optimizing maternal-fetal outcomes. Analgesia during labor alleviates the intense pain, allowing mothers to maintain their energy, resulting in reduced maternal exhaustion and facilitating a more efficient progression of labor.1 Consequently, this can potentially minimize the risk of prolonged labor and its associated outcomes, such as birth asphyxia in infants. Effective pain management during labor analgesia has a beneficial effect on the newborn by promoting successful breastfeeding. The occurrence of maternal pain and stress during labor can result in difficulties in breastfeeding and its subsequent consequences. Analgesia improves both maternal and fetal outcomes by alleviating maternal pain and stress.2
Labor analgesia encompasses a diverse range of options, including pharmacological methods such as epidural or spinal anesthesia, as well as non-pharmacological techniques, including relaxation, breathing exercises, or hydrotherapy.3 The availability of diverse analgesic modalities allows tailored pain management, personalized according to each woman’s specific needs and preferences, thereby enhancing the overall childbirth experience. Epidural and intrathecal blockade are two frequently employed techniques for achieving comprehensive analgesia during the initial and subsequent phases of labor. Out of these two pain management methods, epidural analgesia has been shown to offer a superior safety profile for pregnant women and newborns.4
Various epidural analgesia regimens include single bolus epidural analgesia, continuous epidural infusion, PCEA, PIEB, and PCEA with PCEA in background.5 Patient-controlled epidural analgesia is associated with improved pain management and a sense of autonomy. Multiple studies have shown numerous advantages of using the PIEB technique, which involves the automatic administration of a predetermined dose of local anesthetic drug at specific time intervals, as opposed to the continuous epidural infusion technique. The benefits include improved maternal satisfaction, decreased local anesthetic requirement, and reduced time for the second stage of labor. Furthermore, it is linked to a reduced likelihood of instrumental deliveries.6
Childbirth entails inevitable pain, which often instills a profound sense of fear in many women, particularly nulliparous women.7 The severity as well as perception of labor pain experienced by nulliparous and multiparous women vary significantly. Nulliparous women have a higher likelihood of experiencing fear related to the pain of childbirth, whereas multiparous women are less apprehensive.8 Moreover, in nulliparous women, more significant pain is experienced during the early phase of labor, whereas in multiparous women, more intense pain is experienced during the pelvic phase due to the rapid descent of the fetus. Nevertheless, it is crucial to recognize that parity is not a decisive factor in determining the need for labor analgesia, which should be offered to all women during childbirth.9
This comparative study aimed to analyze the effectiveness of PIEB interval 90 (EI90) of 10 ml 0.0625% bupivacaine and 2 μg/mL fentanyl in nulliparous versus multiparous parturient.
2. METHODOLOGY
This prospective comparative study was conducted in the Anesthesiology Department at Menoufia University over a 1-year period, from November 2022 to November 2023, after approval of the local ethical committee Menoufia University Faculty of Medicine Research Ethical Committee date and number 10/2022ANET1-1 chairperson Professor Walaa Farid and ClinicalTrials.gov ID: NCT05441085. The study included a cohort of 30 patients who were undergoing routine vaginal delivery and receiving epidural analgesia. The selection of these patients was based on pre-established criteria for inclusion and exclusion. The patients received a detailed explanation of the nature of the study, and written consent was obtained from all participants.
The sample size was determined by analyzing previous literature (Laura et al., 2018), which revealed that nulliparous women experienced labor pain for a significantly longer duration compared to multiparous women. The nulliparous women gave birth 9.3 hours after the debut of pain (95%CI:8.11–13.25). In contrast, the multiparous women delivered 8.1 hours after the debut of pain (95%CI:2.25–9.22).10 The minimum sample size was calculated using statistics, and sample size provision 6 was 30 subjects divided into two equal groups. The power of the study is 80%, and the confidence level is 95%. Consequently, 30 patients were included, with 15 patients in each of the two groups. For the purpose of comparison, the patients were categorized into the following groups: Group N compromised 15 nulliparous women receiving epidural analgesia for labor pain, whereas Group M included 15 multiparous women receiving epidural analgesia for labor pain.
Inclusion criteria: Participants who provided informed written consent, pregnant women in the initial stage of labor, with a gestational age of more than 37 weeks, experiencing regular contractions every 5 min, and cervical dilation between 2 and 5 cm, as well as patients classified as American Society of Anaesthesiologists (ASA) II and III. Exclusion criteria: Individuals who refused to provide consent for participation, contraindications to epidural analgesia, and known allergy to bupivacaine or fentanyl. Patients who received opioid analgesic or sedatives within 4 hours prior to epidural insertion, inadvertent dural puncture, patients who delivered within 1 hour or failed to achieve a VAS score less than two after the initiation of an epidural clinician bolus.
Baseline measurements, including pulse rate, blood pressure, and oxygen saturation, were recorded for all participants. A 500 mL infusion of Ringer’s lactate as pre-load was initiated. The patient was positioned in a seated posture, and an epidural catheter was inserted using an 18-G Tuohy needle, following skin sterilization with a 2% chlorhexidine in 70% alcohol solution. The loss-of-resistance technique was employed with either air or saline. A 19-G multi-orifice wire-reinforced catheter (Arrow Flextip plus; Arrow International Inc., Reading, PA, USA) was then inserted 5 cm into the epidural space. Aspiration was conducted to ensure the absence of blood or cerebrospinal fluid.
Initially, a preliminary dose of 0.125% bupivacaine 3 mL with fentanyl 3.3 μg/mL was administered. After three minutes, a loading dose consisting of 2 boluses of bupivacaine 0.125% 6 mL with fentanyl 3.3 μg/mL was injected, with a three-minute interval between them. This loading dose was followed by a maintenance dose comprising bupivacaine 0.0625% with fentanyl 2 μg/mL, where the initial Patient-Initiated Epidural Bolus (PIEB) interval time was set at 60 min. The system was additionally programmed with PCEA settings to give 10 mL of the same local anesthetic solution with a lockout period of 10 min. Maximum total volume was set to 30 mL/hr, including the PIEB and the PCEA. Patients were instructed to push the PCEA switch if they found contractions to be uncomfortable.
The primary outcomes in the present study were the labor pain severity assessed by the VAS score, the number of PCEA attempts, the volume administered via PCEA, and the timing of the first PCEA bolus. The hemodynamic parameters were monitored. The time spent in the second stage of labor, type of labor, and incidence of adverse effects were also compared.
Statistical analysis
Statistical analysis was done with the help of IBM SPSS 23.0. Descriptive statistics were employed, continuous variables are presented as mean and standard deviation, whereas categorical data are presented as frequencies and percentages. The study groups are compared using independent t-tests for continuous data and chi-square tests for categorical data analysis. P < 0.05 is taken to be statistically significant.
3. RESULTS
This study involved 39 patients who were undergoing normal vaginal delivery and receiving epidural analgesia. After exclusion of patients who didn’t meet inclusion criteria or refused to participate in the study, 36 patients were selected. After taking full obstetric history they were subdivided into two groups; Group M (multipara) (n = 19) and Group N (nullipara) (n = 17). Six patients experienced failed vaginal delivery and underwent C-section leaving 15 patients in each group. The groups were compared for mean age, weight, and ASA Grades. The mean age of the patients in Group N was less than that of those in Group M, and this difference was significant (P = 0.011). The mean weight and ASA grades were comparable in both groups (Table I).
The groups were compared for pregnancy characteristics and comorbidities. Both groups were comparable in prevalence of gestational diabetes and pre-eclampsia (P > 0.05). The mean Gestational age of patients in Group N and Group M was 38.94 ± 1.24 and 38.12 ± 1.34 weeks. The gestational age in both the groups was comparable (P = 0.09) (Table 1).
The comparison of patients for induction and augmentation of labor showed both groups to be comparable (P > 0.05). Assisted vaginal delivery was done in 4 (26.67%) patients in Group N and 2 (13.33%) patients in Group M. Need for assisted delivery was more in Group N as compared to Group M. However, the difference was not statistically significant (P > 0.05). Duration of the first and second stages of labor was more in Group N patients than in Group M (P < 0.0001) (Table 1).
| Table 1: Comparative demographic data of the patients, co-morbidities and labor profile in the groups | ||||
| Variable | Group N | Group M | P-value | |
| Mean age (years) | 23.12 ± 4.98 | 29.12 ± 6.98 | 0.011* | |
| Mean weight (kg) | 58.76 ± 8.12 | 63.24 ± 5.64 | 0.0902 | |
| ASA Grade | Grade II | 13 (73.33) | 22 (80 ) | 1.0 |
| Grade III | 2 (26.66) | 3 (20) | ||
| Gestational diabetes | 2 (13.33) | 2 (26.66) | 1.0 | |
| Pre-eclampsia | 1 (6.67) | 1 (6.67) | 1.0 | |
| Gestational age (in weeks) | 38.94 ± 1.24 | 38.12 ± 1.34 | 0.09 | |
| Induction of labour | 5 (33.33) | 5 (33.33) | 1.0 | |
| Augmentation of labour | 8 (53.33) | 5 (33.33) | 0.46 | |
| Spontaneous vaginal delivery | 11 (73.33) | 13 (86.67) | 0.65 | |
| Assisted vaginal delivery | 4 (26.67) | 2 (13.33) | 0.65 | |
| Duration of 1st stage of labor (min) | 269.4 ± 23.06 | 151.3 ± 54.92 | P < 0.0001** | |
| Duration of 2nd stage of labor (min) | 84.64 ± 38.86 | 38.70 ± 28.12 | 0.0009 ** | |
| Data are expressed as mean ± SD or n (%); *Statistically significant; **Highly Statistically significant | ||||
The pain intensity of the patients in both groups was assessed by calculating the mean VAS scores at various time intervals following the onset of labor. While the pain experienced by patients in Group N was more severe compared to patients in Group M, it was equivalent to a duration of 3 hours. Between 4th and 7th hours, Group N patients experienced a higher level of pain intensity than Group M patients, and this difference was found to be statistically significant (P < 0.05). The pain intensity between the two groups was comparable from 8 to 12th hours (P > 0.05), as shown in Table 2.
| Table 2: Mean VAS scores in studied groups at different intervals. | |||
| Duration | Group N | Group M | P value |
| At Admission | 1.92 ± 0.56 | 1.78 ± 0.48 | 0.468 |
| 30 minutes | 2.62 ± 0.98 | 2.12 ± 1.82 | 0.356 |
| 1 hours | 4.12 ± 2.12 | 4.98 ± 2.40 | 0.307 |
| 3 hours | 5.98 ± 2.62 | 5.34 ± 2.40 | 0.491 |
| 4 hours | 6.34 ± 3.14 | 3.64 ± 1.46 | 0.005* |
| 5 hours | 5.84 ± 2.98 | 2.90 ± 1.12 | 0.001* |
| 6 hours | 3.54 ± 0.94 | 2.12 ± 0.98 | 0.0004* |
| 7 hours | 3.12 ± 0.88 | 2.20 ± 0.86 | 0.0073* |
| 8 hours | 2.44 ± 0.96 | 2.02 ± 0.70 | 0.181 |
| 10 hours | 2.10 ± 0.86 | 1.94 +/ 0.64 | 0.56 |
| 12 hours | 1.68 ± 0.70 | 1.34 ± 0.58 | 0.15 |
| Data are expressed as mean ± SD; *Statistically significant | |||
The average duration for the first PCEA bolus in Group N and Group M was 94 ± 18 and 124 ± 22 minutes, respectively. The mean duration was more significant in Group M compared to Group N, and this difference was statistically significant (P = 0.0003). Group N had significantly higher mean PCEA doses and volume of drug administered compared to Group M (P < 0.0001), as illustrated in Table 3.
| Table 3: Comparison of mean time to PCEA bolus, mean PCA doses and volume | |||
| Duration | Group N | Group M | P value |
| Mean time for 1st
PCEA bolus (min) |
94 ± 18 | 124 ± 22 | 0.0003 ** |
| Mean PCEA doses (mg) | 5.94 ± 0.48 | 3.45 ± 0.54 | < 0.0001** |
| Volume administrated
by PECA (mL) |
64. 34 ± 13.98 | 42.34 ± 11.68 | 0.0001** |
| Data are expressed as mean ± SD; *Statistically significant; **Highly Statistically significant | |||
The average heart rate in Group N and Group M was determined to be 79.73 ± 3.12 and 78.24 ± 2.60, respectively. Both groups’ mean heart rates and mean arterial pressures were comparable (P > 0.05; Figure 1).
Figure 1: Comparison of Mean Heart Rate, MAP and SpO2 in groups
Both groups were compared on the basis of adverse events. In Group N and M 5 (33.33%) and 4 (26.66%) patients developed adverse events. In Group N, three patients (20%) developed tachycardia whereas 1 (6.66%) patient in Group M developed bradycardia. Pruritis was detected in two patients (13.33%) of Group N and 3 (20%) patients of Group M. The analysis of adverse events in both groups showed that the incidence of adverse events was comparable in both groups (Figure 2).
Figure 2: Comparison of adverse effects in both the cases
4. DISCUSSION
Effective and safe analgesia is crucial for the successful management of patients in labor. It ensures that the expulsive efforts required for labor progress are preserved. In recent times, epidural analgesia become increasingly popular for labor analgesia, and several studies have established its effectiveness.11 In this study, we aimed to compare the efficacy of epidural analgesia in both nulliparous and multiparous women. Our comparative analysis revealed that patients in both groups were comparable in terms of demographic characteristics, ASA Grades, and the prevalence of pre-eclampsia and gestational diabetes. However, when considering the type of delivery, it was observed that the need for assisted delivery was slightly lower in Group M compared to Group N. However, this difference was not statistically significant (P > 0.05). Moreover, the duration of the first and second stages of labor was considerably longer in Group N than in Group M (P < 0.0001).
A study by Jardine et al. (2020) aimed to determine the rate of complicated births in nulliparous as well as multiparous women, analyzing maternity records of 276,766 women having singleton pregnancies.12 In this study, authors defined complicated delivery as birth associated with the use of instruments, cesarean section, perineal tears, postpartum hemorrhage, or an Apgar score of 7 or less than 7 at five minutes. This study revealed a notably higher risk of instrumental delivery in nulliparous cases compared to multiparous women, which is similar to our findings. Likewise, a similar increased risk of instrumental deliveries in nulliparous women was also reported by Mazouni C et al. (2006) and Wassen MM et al. (2011).13,14
Although pain is an unavoidable aspect of labor, it is important to acknowledge that the experience of labor pain varies in nulliparous women. Multiparous women typically exhibit more severe pain and a greater fear of pain compared to multiparous women. In our study, the comparison of pain severity assessed by VAS scores showed that pain levels were comparable in both groups for the first three hours from the start of labor. During the period from the fourth to the seventh hour, patients in Group N experienced more intense pain compared to those in Group M, and this difference was found to be statistically significant (P < 0.05). Between the eighth and the twelfth hour postpartum, the severity of pain was comparable in both groups (P > 0.05).
In a study by Fridh et al., the authors explored background factors, emotional feelings, and mothers’ expectations concerning pain intensity during labor. They found that parity, young age, lower educational qualification, history of menstrual irregularity, previous abortion, emotional instability, and unrealistic expectations of labor pain were associated with increased pain intensity during labor.15 Similar factors affecting the intensity of labor pain were also reported in studies done by Sheiner E et al. (1998) and Labor S et al. (2008).16,17
In our study, epidural analgesia was administered using PIEB and PCEA. A comparison of patients based on the meantime for the 1st PCEA bolus showed that the mean time was 94 ± 18 minutes in Group N and 124 ± 22 min in Group M. The mean time was shorter in Group N compared to Group M, and this difference was highly statistically significant (P = 0.0003). Similarly, mean PCEA doses and the volume of drugs administered via PCEA were greater in Group N compared to Group M, and this difference was statistically significant (P < 0.0001). Notably, there is limited research on the differences in drug requirement during epidural analgesia between nulliparous and multiparous women. However, Malevic et al. (2019) discovered notable variations in the preferences for pain relief methods between primiparous and multiparous women.18 Epidural analgesia was preferred by primiparous women, while delivery without any analgesia was more common among multiparous women. These findings are consistent with our study in terms of the effectiveness of epidural analgesia during labor. Studies by Halpern et al. (2010) and Agrawal D et al. (2014) have reported similar conclusions in their studies.19,20
The patient groups experienced minor adverse effects, such as transient tachycardia, bradycardia, and pruritus. The incidence of adverse effects in both groups was similar statistically (P > 0.05).
5. LIMITATIONS
Besides a small sample size, one limitation of the study was that the patients were instructed to administer a dose of PCEA based on their own perception of discomfort, which is a subjective criterion.
6. CONCLUSION
PIEB combined with PCEA is an excellent method of providing labor analgesia in nulliparous as well as multiparous women. Nulliparous women are more likely to use top-up doses of PCEA as compared to multiparous women. However, more studies are required to determine The EI 90 for multiparous patients.
7. Data availability
The numerical data generated during this research is available with the authors.
8. Conflict of interest
All authors declare that there was no conflict of interest.
9. Funding
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Authors’ contribution
Both authors took equal part in the concept, study design, conduct of study, literature search and manuscript preparation.
11. REFERENCES
- Piper JM, Bolling DR, Newton ER. The second stage of labor: factors influencing duration. Am J Obstet Gynecol. 1991;165(4 Pt 1):976–9. ]PubMed] DOI: 1016/0002-9378(91)90452-w
- Cambic CR, Wong CA. Labour analgesia and obstetric outcomes. Br J Anaesth. 2010;105 Suppl 1:i50–60. ]PubMed] DOI: 1093/bja/aeq311
- Eyeberu A, Debela A, Getachew T, Dheresa M, Alemu A, Dessie Y. Obstetrics care providers attitude and utilization of non-pharmacological labor pain management in Harari regional state health facilities, Ethiopia. BMC Pregnancy Childbirth. 2022;22(1):389. ]PubMed] DOI: 1186/s12884-022-04717-9
- Pandya ST. Labour analgesia: recent advances. Indian J Anaesth. 2010;54(5):400–8. ]PubMed] DOI: 4103/0019-5049.71033
- Xu J, Zhou J, Xiao H, Pan S, Liu J, Shang Y, et al. A systematic review and meta-analysis comparing programmed intermittent bolus and continuous infusion as the background infusion for parturient-controlled epidural analgesia. Sci Rep. 2019;9(1):2583. ]PubMed] DOI: 1038/s41598-019-39248-5
- Carvalho B, George RB, Cobb B, McKenzie C, Riley ET. Implementation of programmed intermittent epidural bolus for the maintenance of labor analgesia. Anesth Analg. 2016;123(4):965–71. ]PubMed] DOI: 1213/ANE.0000000000001407
- Hendrix YMGA, Baas MAM, Vanhommerig JW, de Jongh A, Van Pampus MG. Fear of childbirth in nulliparous women. Front Psychol. 2022;13:923819. ]PubMed] DOI: 3389/fpsyg.2022.923819
- Kananikandeh S, Amin Shokravi F, Mirghafourvand M, Jahanfar S. Factors of the childbirth fear among nulliparous women in Iran. BMC Pregnancy Childbirth. 2022;22(1):547. ]PubMed] DOI: 1186/s12884-022-04870-1
- American Society of Anesthesiologists Task Force on Obstetric Anesthesia. Practice guidelines for obstetric anesthesia: an updated report. Anesthesiology. 2007;106:843–63. ]PubMed] DOI: 1097/01.anes.0000264744.63275.10
- Jacobsen LK, Helle H, Christina B, Laursen BS. Medically induced labor: Epidural analgesia and women’s perceptions of pain in early labor. European J Midwifery. 2018;2:15. DOI: 18332/ejm/99545
- Craig D, Carli F. Bromage motor blockade score - a score that has lasted more than a lifetime. Can J Anaesth. 2018;65(7):837–8. ]PubMed] DOI: 1007/s12630-018-1101-7
- Jardine J, Blotkamp A, Gurol-Urganci I, Knight H, Harris T, Hawdon J, et al. Risk of complicated birth at term in nulliparous and multiparous women using routinely collected maternity data in England: cohort study. BMJ. 2020;371:m3377. ]PubMed] DOI: 1136/bmj.m3377
- Mazouni C, Porcu G, Bretelle F, Loundou A, Heckenroth H, Gamerre M. Risk factors for forceps delivery in nulliparous patients. Acta Obstet Gynecol Scand. 2006;85(3):298–301. ]PubMed] DOI: 1080/00016340500500782
- Wassen MM, Zuijlen J, Roumen FJ, Smits LJ, Marcus MA, Nijhuis JG. Early versus late epidural analgesia and risk of instrumental delivery in nulliparous women: a systematic review. BJOG. 2011;118(6):655–61. ]PubMed] DOI: 1111/j.1471-0528.2011.02906.x
- Fridh G, Kopare T, Gaston-Johansson F, Norvell KT. Factors associated with more intense labor pain. Res Nurs Health. 1988;11(2):117–24. ]PubMed] DOI: 1002/nur.4770110207
- Sheiner E, Sheiner EK, Shoham-Vardi I. The relationship between parity and labor pain. Int J Gynaecol Obstet. 1998;63(3):287–8. ]PubMed] DOI: 1016/s0020-7292(98)00164-7
- Labor S, Maguire S. The pain of labour. Rev Pain. 2008;2(2):15–9. ]PubMed] DOI: 1177/204946370800200205
- Malevic A, Jatuzis D, Paliulyte V. Epidural analgesia and back pain after labor. Medicina (Kaunas). 2019;55(7):354. ]PubMed] DOI: 3390/medicina55070354
- Halpern SH, Abdallah FW. Effect of labor analgesia on labor outcome. Curr Opin Anaesthesiol. 2010;23:317–22. ]PubMed] DOI: 1097/ACO.0b013e3283385492
- Agrawal D, Makhija B, Arora M, Haritwal A, Gurha P. The effect of epidural analgesia on labour, mode of delivery and neonatal outcome in nullipara of India, 2011–2014. J Clin Diagn Res. 2014;8:OC03–6. ]PubMed] DOI: 7860/JCDR/2014/9974.4930