Amin M. Alansary, MD1, Mohamed Mourad Ali, MD2, Minatallah Ali Elshafie, MD3
Author affiliation:
Background & Objective: Cleft lip surgery is routinely performed in children under general anesthesia (GA). Infraorbital nerve block (IONB) has been used by some anesthetists to enhance the perioperative pain management in addition to the routine intravenous analgesics. We compared the addition of dexmedetomidine (Dex) plus bupivacaine with magnesium sulphate (MgSO4) plus bupivacaine for IONB in combination with GA, regarding their efficacy, effect on the duration of postoperative analgesia, and any adverse events.
Methodology: A total of 75 patients, aged 3 months to 7 y, of either sex, were randomly allocated into three equal groups. After induction of GA with a standardized method, Group D received IONB with Dex + bupivacaine; Group M received the nerve block with MgSO4 + bupivacaine, and a control group (Group C) received block with bupivacaine only. Acetaminophen infusion was used when additional analgesic was required in the postop period. The primary outcome was the duration of time until the first analgesic was administered, while the secondary outcomes were the amount of acetaminophen taken within the first 24 h following surgery, pain scores, and the frequency of side effects.
Results: The mean time to first requested analgesia was significantly longer in the Group D, followed by the Group M, and it was the shortest in the Group C (13.9 ± 1.7 h, 11.5 ± 2 h, 5.9 ± 1.3 h respectively, P < 0.001). Total acetaminophen consumption and pain scores were significantly lower among the Group D than the Group M and highest in the Group C (P < 0.001). Emergence agitation and vomiting were non-significantly less frequent in the Group D than the Group M and more frequent in the Group C. No significant difference regarding hypotension, bradycardia, and shivering, was observed among all the groups. Respiratory depression was not recorded in any of the groups.
Conclusion: Dexmedetomidine and magnesium sulphate, both offered prolonged analgesia when added to bupivacaine for infraorbital nerve block for perioperative analgesia in pediatric patients undergoing cleft lip surgery under general anesthesia. However, dexmedetomidine was superior to magnesium sulphate regarding the duration of postoperative analgesia.
Abbreviations: ASA-PS - American Society of Anesthesiologists Physical Status classification; Dex – Dexmedetomidine; FiO2 - Fraction of inspired oxygen; IONB - Infraorbital nerve block; MBP - Mean blood pressure; NIBP - Non-invasive blood pressure; PACU - Post Anesthesia Care Unit
Key words Bupivacaine; Cleft Lip; Dexmedetomidine; Infraorbital Nerve Block; Magnesium Sulfate
Citation: Alansary AM, Ali MM, Elshafie MA. A randomized controlled trial of dexmedetomidine vs magnesium sulfate as adjuvants to bupivacaine in infraorbital nerve block for perioperative analgesia in pediatric patients undergoing cleft lip surgery. Anaesth. pain intensive care 2023;27(4):514−522; DOI: 10.35975/apic.v27i4.2261
Received: May 22, 2023; Reviewed: June 02, 2023; Accepted: June 11, 2023
Cleft lip is a congenital craniofacial birth anomaly with a high prevalence. It is described as an upper lip fissure that was present at birth. It may be unilateral, bilateral, complete (extending to the nasal cavity), or incomplete. It may also be accompanied by a palatal cleft.1
The most widely used anesthetic method for cleft lip repair is general anesthesia (GA) combined with infraorbital nerve block (IONB). Combined use of GA and IONB reduces intraoperative anesthetic requirements, postoperative pain, and total opioid use.2 IONBs have been claimed to be effective for cleft lip repair;3 however, the duration and effectiveness of the regional block following a single local anesthetic dose are limited. Hence, adjuvants have to be added to local anesthetics to potentiate and prolong the local analgesic effect.4
Compared to clonidine, Dex is a more selective α2- adrenoreceptor agonist. It also has more analgesic and opioid-sparing effects.5 As an adjuvant to local anesthetics in peripheral nerve blocks, Dex has been recently introduced.6 Perineural Dex has been demonstrated to decrease opioid consumption while also extending the duration of the postoperative sensory block.7
The analgesic effect of MgSO4 has recently been recognized.8 When combined with local anesthetics, MgSO4 acts as an N-methyl-D-aspartate (NMDA) receptor antagonist and has been shown to decrease acute postoperative pain, analgesic consumption, or both.9,10 In pediatric patients, MgSO4 may be effective as an analgesic adjuvant in locoregional anesthesia.11
Moreover, adding MgSO4 as an adjuvant to regional blocks improves and extends the analgesic effect of local anesthetics, speeds up recovery from surgery, and reduces the likelihood of emergence agitation.12,13
We aimed to compare the effectiveness of IONB using a combination of bupivacaine with Dex or MgSO4 for perioperative analgesia as well as anesthesia-related adverse effects in pediatric patients scheduled for cleft lip repair.
Formal approval of this study was obtained from the research ethics committee of the Faculty of Medicine, Ain-Shams University (No. FMASU R 176/2022), and it was registered at clinical trials.gov with ID NCT05624151 on November 21, 2022.
This prospective, randomized, controlled trial was carried out at the orthodontics and dentofacial surgery unit of Ain-Shams University hospitals. Patient enrollment was started on November 25, 2022, and ended on May 2, 2023. All patients’ guardians provided their written, informed consent. The Declaration of Helsinki's guiding principles were followed in conducting the study.
A total of 75 pediatric patients of both sexes, 3 months to 7 y old, with an ASA-PS I or II, scheduled for elective cleft lip repair (cheiloplasty) under GA, were enrolled.
Patients with local infection at the injection site, generalized sepsis, coagulopathy, thrombocytopenia, hemophilia, complex congenital heart disease, renal failure, major illnesses, allergy, or contraindications to the study medication, and parental or guardian’s dissent were excluded from the study.
During the preoperative visit, all patients underwent medical evaluation, focusing on the heart, lungs, and airways to identify any associated conditions or abnormalities. Routine laboratory investigations, e.g., a chest X-ray, complete blood count, and coagulation profile, were performed.
Instructions were passed to abstain from clear fluids like water and non-particulate juices for two hours, breast milk for four hours, formula or solid food for six hours, and fat-containing meals for eight hours.
Before induction of anesthesia, standard monitors were attached in the operating room, and basal readings for the patient's heart rate (HR), mean blood pressure (MBP), and oxygen saturation (SpO2) were recorded.
Conventional GA was administered to every child. Patients were randomly assigned into one of the three groups (25 in each group) using computer-generated randomization numbers with a closed-seal envelope.
The first group (Group D) received bilateral IONB before surgical incision with one ml of a mixture of bupivacaine 0.25% plus 0.5 μg/kg Dex, while patients in the 2nd group (Group M) received bilateral IONB with one ml of a mixture of bupivacaine 0.25% with 2 mg/kg MgSO4 to a maximum of 50 mg. Patients in the 3rd group (Group C) served as control, and received bilateral IONB with one ml of bupivacaine 0.25%.
Sevoflurane in an O2/air mixture (FiO2 = 0.8) with a sealed face mask was used to induce anesthesia in spontaneously breathing patients. A peripheral venous cannula was inserted after the patients' consciousness was lost. Fentanyl 1–2 μg/kg and propofol 1–2 mg/kg were administered to achieve a deep plane of anesthesia. Rocuronium 0.9 mg/kg was administered intravenously to facilitate endotracheal intubation with a preformed Ring–Adair–Elwyn (RAE) endotracheal tube, which was fixed centrally over the lower lip. Capnography confirmed the correct placement of the tube.
After fixing the endotracheal tube, pressure-controlled ventilation was adjusted to maintain normocapnia by continuously monitoring end-tidal CO2 for adequate ventilation. According to age and body weight, Ringer's solution was infused in all patients. Sevoflurane in O2/air mixture (FiO2 = 0.3) at 1% minimum alveolar concentration and rocuronium supplementation at 0.15 mg/kg were used to maintain anesthesia.
The technique of IONB
Bilateral IONB was performed on all participants using the intraoral approach before surgical repair. The upper lip was pulled back after the infraorbital foramen was palpated, and a 28 G needle was then advanced to the foramen parallel to the maxillary premolar.
The needle was advanced cephalad by positioning a finger at the level of the infraorbital foramen. After negative aspiration on each side, the target volume was injected (Figure 1).

A pediatric anesthesiologist with five years of experience in pediatric regional nerve blockade performed IONBs.
Cardiovascular monitoring (HR, MBP) was maintained throughout the procedure; readings were taken every 5 minutes and recorded at specific intervals (baseline, after intubation, 10 minutes after block, mid-operative, and after extubation). Any adverse events, such as bradycardia or hypotension, were immediately dealt with.
When the procedure was finished, inhalational anesthesia was stopped, the minimal to moderate amount of blood and oral secretions in the oropharynx were carefully suctioned, and reversal agents (atropine 10-15μg/kg and neostigmine 0.05 mg/kg) were administered once the neuromuscular blockade had sufficiently recovered and adequate spontaneous breathing had been regained. An infant who was awake, presented with regular breathing and had good muscle tone underwent extubation after his or her airway reflexes had returned.
Patients were then transported to the Post-Anesthesia Care Unit (PACU) when they were stable from both cardiovascular and respiratory standpoints. A pediatric anesthesiologist and nurse, who were blinded to the study methodology, observed them. Hemodynamic measurements were recorded in the PACU at Minute 30, as well as at intervals of 1, 2, 4, 6, 12, and 24 h starting from the time of patient arrival. The child was discharged to the ward after meeting the standard discharge criteria.
FLACC scale 15 was used by a blinded observer anesthesiologist to assess pain in patients during the first 24 h (ranging from 0–10, where 0 = no pain, 10 = worst pain), at the time of arrival to the PACU, at postoperative minute 30, and then at 1, 2, 4, 6, 12 and 24 h.
Acetaminophen was administered intravenously at a dosage of 10 mg/kg whenever the FLACC Score was greater than 4. If the FLACC score was ≥ 4, the dose was repeated every six hours until they could tolerate oral intake. The time to the first analgesic requirement and the total acetaminophen consumption over the first 24 h postoperatively were recorded.
The Pediatric Anesthesia Emergence Delirium (PAED) scale 16 was used to measure the incidence of emergence agitation at 0, 5, 10, 20, 30, and 60 min. Additionally, postoperative vomiting (POV) within the first 24 h following surgery was noted. If POV developed, ondansetron 0.1 mg/kg was prescribed intravenously.
Hypotension, bradycardia, shivering, and respiratory depression were among the other adverse side effects that were noted. The primary outcome was the time to the first analgesic request, while the secondary outcomes were the total amount of acetaminophen consumed in the first 24 h following surgery, pain assessments, and adverse drug reactions.
Sample size calculation
Using the STATA program, the sample size was calculated with the type 1 error (α) set to 0.05 and the power (1-β) set to 0.9. The result from a previous study by Sayed et al.,17 showed that there was a significant difference between the study groups concerning the frequency of acetaminophen administrations; as 63% of cases in the Group D had paracetamol more than one time, compared to only 13% of patients of Group M. Calculation according to these values produced a sample size of 22 cases per group. To compensate for drop-outs, we included 25 cases in each group (a total sample of 75 cases).
Statistical methodology
The gathered data were coded, tabulated, and statistically analyzed using IBM SPSS statistics (Statistical Package for Social Sciences) software, version 28.0, IBM Corp., Chicago, USA, 2021. Shapiro-Wilk test was used to determine the normality of quantitative data, which was followed by mean and SD (standard deviation) descriptions and an ANOVA test to compare them. For variables with low expected values, Fisher's Exact and Chi-Square tests were used to compare qualitative data that are expressed as numbers and percentages. Pairwise comparisons were made by using the post hoc Bonferroni test. P < 0.050 was considered significant.
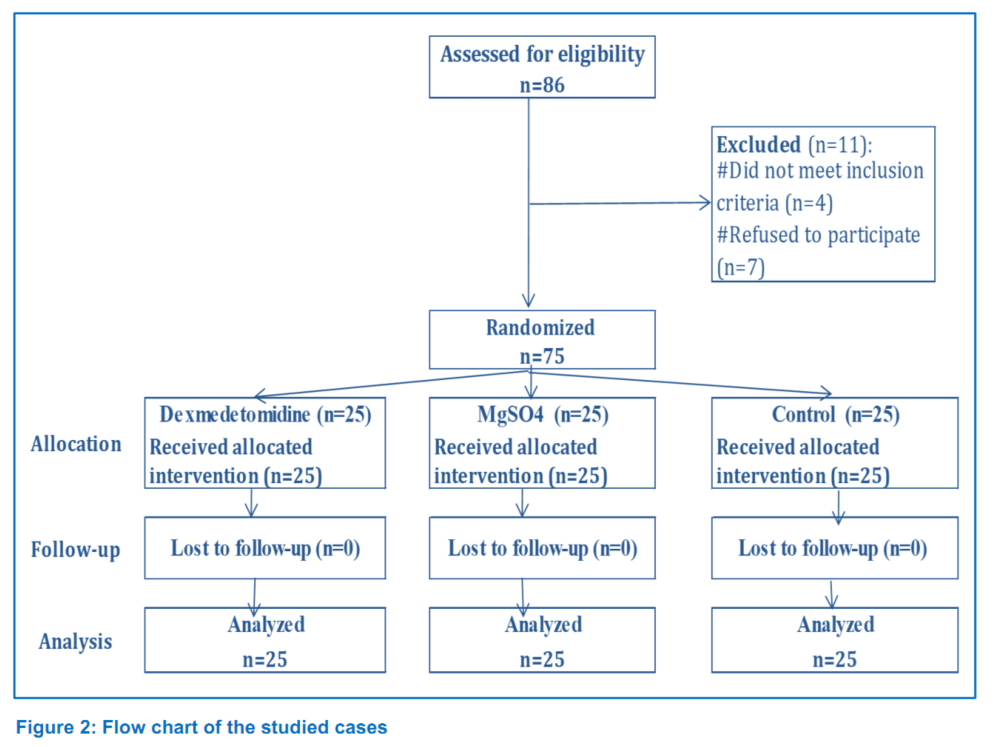
The study's eligibility requirements were checked on 86 patients. Four patients did not meet the inclusion criteria, and seven patient guardians declined to participate, resulting in the exclusion of eleven patients. In the end, 75 patients—25 for each group—completed the study and their data were analyzed (Figure 2).
Patients in the three groups didn’t differ regarding their demographic data (age, weight, sex, ASA-PS), repair type, and duration of surgery or anesthesia (Table 1).
There was no significant difference in all groups regarding HR and MBP in the intraoperative time (baseline, after intubation, 10 min after block, and mid-operative) as well as from postoperative min-0 to 4 h. HR and MBP at 6, 12, and 24 h were the lowest in the Group D, followed by the Group M, and the highest in the Group C, the differences were significant only in the Group D at 6 h, while the differences were between all the study groups at 12 and 24 h.

Postoperative pain scores at different time points were non-significantly lowest in the Group D, followed by the Group M, and were the highest in the Group C, the differences were significant only in the Group C at 6 h, while the differences were between all the study groups at 12 and 24 h (Figure 3).
Time to first requested analgesia was significantly longest in the Group D, followed by the Group M, and shortest in the Group C (13.9 ± 1.7 h, 11.5 ± 2.0 h, 5.9 ± 1.3 h) respectively (Figure 4).
In addition, the rate of analgesic doses was significantly less frequent in the Group D followed by Mgso4, and more frequent in the Group C. Furthermore, total postoperative acetaminophen consumption was significantly lower in the Group D, followed by the Group M, and highest in the Group C (Figure 4).
Regarding postoperative side effects, emergence agitation, and POV were non-significantly less frequent in the Group D, followed by the Group M, and most frequent in the Group C. PAED scale at different time points was non-significantly lowest in the Group D, followed by the Group M, and highest in the Group C. Sedation was non-significantly most frequent in the Group D, followed by the Group M, and least frequent in the Group C. Bradycardia non-significantly occurred only in the Group D. Hypotension was non-significantly least frequent in the Group M, with equal incidences in Group D and Group C. Shivering was non-significantly most frequent in the Group C, with equal incidences in Group M and Group C. Respiratory depression did not occur in all studied groups (Table 2).

Perioperative pain management after cleft lip repair is very challenging, as the procedure is very painful and it's difficult to assess and manage pain at this age. We aimed for effective prolonged analgesia to avoid a vigorous child in pain which is considered as one of the risk factors for postoperative bleeding.
Our results reported that the time to first request rescue analgesia was significantly increased in the dexmedetomidine group, followed by the MgSO4 group, and shortest in the control group. The total acetaminophen dose needed was significantly lowest in the Group D, followed by the Group M, and highest in the Group C.
Opioids are widely used for the treatment of moderate to severe pain in pediatric patients, particularly in the immediate postoperative period. However, opioids are associated with a range of side effects, including nausea, vomiting, constipation, urinary retention, pruritus, sedation, respiratory depression, and opioid-induced hyperalgesia.18,19,20 Opioid‐sparing approaches to postoperative analgesia, including IONB should be considered to avoid the complications of opioids during postoperative recovery.
El-Emam EM at al.21 compared Dex against dexamethasone as adjuvants for bupivacaine in IONB and they noticed that Dex resulted in a more prolonged duration of analgesia and lower pain scores. Our study results are consistent with the study by Sumalatha G et al., who showed that 0.5 μg/kg Dex added to bupivacaine increased the duration of analgesia when compared to plain bupivacaine in IONB in children undergoing cleft lip surgery, and the number of patients who requested rescue analgesics were less.22 Other studies supported our results, and proved that the addition of Dex to ropivacaine in supraclavicular brachial plexus block significantly prolongs the duration of analgesia.23,24
Dexmedetomidine and other alpha-2 selective adrenergic agonists are effective analgesics when combined with local anesthetics for peripheral blocks.25 It inhibits current channels that help neurons return from a hyperpolarized state to their normal resting potential. Dex also selectively prevents C-fiber neurons from firing additional action potentials, causing analgesia. The majority of analgesic and sedative effects on the CNS are mediated by α2A-subtype receptors.26
On the other hand, the addition of MgSO4 as an adjuvant to bupivacaine as explained by Verma V, et al., significantly prolongs the duration of analgesia and decreases the analgesic requirement in ultrasound-guided supraclavicular brachial plexus block.27 Similarly, he concluded that MgSO4 and ketamine were effective as adjuvants to levobupivacaine in erector spinae block for postoperative analgesia in breast cancer surgery, but with better analgesia provided by MgSO4.
MgSO4 is an N-methyl-d-aspartate (NMDA) receptor antagonist that works to reduce excitatory neurotransmission by restricting intracellular calcium levels through NMDA receptor antagonism.29 Contrary to our results, Sayed et al. investigated and proved that magnesium had a prolonged analgesic effect compared with Dex.
We demonstrated in our results that postoperative pain perception at different time points was lowest in the Group D with a more frequent sedation level, followed by Group M and the highest pain perception with the least sedation level in the control group, Simultaneously, these differences were recorded by a systematic review and meta-analysis conducted by Vorobeichik et al. that perineural Dex was followed by excessive postoperative sedation that was recorded using many scales.30 On the other hand, Obayah et al. did not demonstrate a sedative effect in their result but, this can be due to the heterogeneity of the scales used.31
Side effects demonstrated in our study as POV was non-significantly less frequent in the dexmedetomidine group, followed by the MgSO4 group, and most frequent in the control group, and there were no other serious side effects. Our results were concomitant with Elsonbaty M, et al.32 who proved that, the IONB technique has minimal complication rate with greater parental satisfaction. Other researchers proved that Dex and MgSO4 as adjuvants showed satisfactory pain relief without serious side effects. 21,28
Our study recorded no relevant intraoperative and postoperatively cardiovascular events. The heart rate remained on the lower side in the Group D but did not require any intervention. Consistent with our results, the results of several studies have demonstrated that Dex can prolong analgesia significantly without inducing significant hypotension, or bradycardia.21,31
Our results suggest that there is a benefit of adding dexmedetomidine or MgSO4 to bupivacaine in IONB in cleft lip surgery. However, dexmedetomidine demonstrated superiority compared to MgSO4 concerning prolonged postoperative analgesia.
6. Data availability
The numerical data is available with the corresponding author and can be provided on request.
7. Conflict of interests
The authors declare no conflict of interest. No funding, either internal or external, was involved in this study.
8. Ethical approval
This prospective, randomized, clinical study was approved by the University of Ain Shams Institutional ethics board review (FMASU R176/2022).
9. Authors' contribution
MA: Concept, data collection, data analysis, literature search, revised and approved the manuscript.
AA, MM and MA: Designed the study protocol, manuscript writing and editing, literature search, revised and approved the manuscript.
Author affiliation:
- Amin Mohamed Alansary, Department of Anesthesiology, Intensive Care & Pain Management, Faculty of Medicine, Ain Shams University, Cairo, Egypt; E-mail: aminalansary@yahoo.com; ORCID: {0000-0002-6615-186X}
- Mohamed Mourad Ali, Department of Anesthesiology, Intensive Care & Pain Management, Faculty of Medicine, Ain Shams University, Cairo, Egypt; E-mail: Mohamed_mourad@med.asu.edu.eg; ORCID: {0000-0003-4667-5719}
- Minatallah Ali Elshafie, Department of Anesthesia, National Liver Institute, Menoufia University, Sheeben Elkom City, Egypt; E-mail: menna80mas@gmail.com; ORCID: {0000-0002-4752-7913}
ABSTRACT
Background & Objective: Cleft lip surgery is routinely performed in children under general anesthesia (GA). Infraorbital nerve block (IONB) has been used by some anesthetists to enhance the perioperative pain management in addition to the routine intravenous analgesics. We compared the addition of dexmedetomidine (Dex) plus bupivacaine with magnesium sulphate (MgSO4) plus bupivacaine for IONB in combination with GA, regarding their efficacy, effect on the duration of postoperative analgesia, and any adverse events.
Methodology: A total of 75 patients, aged 3 months to 7 y, of either sex, were randomly allocated into three equal groups. After induction of GA with a standardized method, Group D received IONB with Dex + bupivacaine; Group M received the nerve block with MgSO4 + bupivacaine, and a control group (Group C) received block with bupivacaine only. Acetaminophen infusion was used when additional analgesic was required in the postop period. The primary outcome was the duration of time until the first analgesic was administered, while the secondary outcomes were the amount of acetaminophen taken within the first 24 h following surgery, pain scores, and the frequency of side effects.
Results: The mean time to first requested analgesia was significantly longer in the Group D, followed by the Group M, and it was the shortest in the Group C (13.9 ± 1.7 h, 11.5 ± 2 h, 5.9 ± 1.3 h respectively, P < 0.001). Total acetaminophen consumption and pain scores were significantly lower among the Group D than the Group M and highest in the Group C (P < 0.001). Emergence agitation and vomiting were non-significantly less frequent in the Group D than the Group M and more frequent in the Group C. No significant difference regarding hypotension, bradycardia, and shivering, was observed among all the groups. Respiratory depression was not recorded in any of the groups.
Conclusion: Dexmedetomidine and magnesium sulphate, both offered prolonged analgesia when added to bupivacaine for infraorbital nerve block for perioperative analgesia in pediatric patients undergoing cleft lip surgery under general anesthesia. However, dexmedetomidine was superior to magnesium sulphate regarding the duration of postoperative analgesia.
Abbreviations: ASA-PS - American Society of Anesthesiologists Physical Status classification; Dex – Dexmedetomidine; FiO2 - Fraction of inspired oxygen; IONB - Infraorbital nerve block; MBP - Mean blood pressure; NIBP - Non-invasive blood pressure; PACU - Post Anesthesia Care Unit
Key words Bupivacaine; Cleft Lip; Dexmedetomidine; Infraorbital Nerve Block; Magnesium Sulfate
Citation: Alansary AM, Ali MM, Elshafie MA. A randomized controlled trial of dexmedetomidine vs magnesium sulfate as adjuvants to bupivacaine in infraorbital nerve block for perioperative analgesia in pediatric patients undergoing cleft lip surgery. Anaesth. pain intensive care 2023;27(4):514−522; DOI: 10.35975/apic.v27i4.2261
Received: May 22, 2023; Reviewed: June 02, 2023; Accepted: June 11, 2023
1. INTRODUCTION
Cleft lip is a congenital craniofacial birth anomaly with a high prevalence. It is described as an upper lip fissure that was present at birth. It may be unilateral, bilateral, complete (extending to the nasal cavity), or incomplete. It may also be accompanied by a palatal cleft.1
The most widely used anesthetic method for cleft lip repair is general anesthesia (GA) combined with infraorbital nerve block (IONB). Combined use of GA and IONB reduces intraoperative anesthetic requirements, postoperative pain, and total opioid use.2 IONBs have been claimed to be effective for cleft lip repair;3 however, the duration and effectiveness of the regional block following a single local anesthetic dose are limited. Hence, adjuvants have to be added to local anesthetics to potentiate and prolong the local analgesic effect.4
Compared to clonidine, Dex is a more selective α2- adrenoreceptor agonist. It also has more analgesic and opioid-sparing effects.5 As an adjuvant to local anesthetics in peripheral nerve blocks, Dex has been recently introduced.6 Perineural Dex has been demonstrated to decrease opioid consumption while also extending the duration of the postoperative sensory block.7
The analgesic effect of MgSO4 has recently been recognized.8 When combined with local anesthetics, MgSO4 acts as an N-methyl-D-aspartate (NMDA) receptor antagonist and has been shown to decrease acute postoperative pain, analgesic consumption, or both.9,10 In pediatric patients, MgSO4 may be effective as an analgesic adjuvant in locoregional anesthesia.11
Moreover, adding MgSO4 as an adjuvant to regional blocks improves and extends the analgesic effect of local anesthetics, speeds up recovery from surgery, and reduces the likelihood of emergence agitation.12,13
We aimed to compare the effectiveness of IONB using a combination of bupivacaine with Dex or MgSO4 for perioperative analgesia as well as anesthesia-related adverse effects in pediatric patients scheduled for cleft lip repair.
2. METHODOLOGY
Formal approval of this study was obtained from the research ethics committee of the Faculty of Medicine, Ain-Shams University (No. FMASU R 176/2022), and it was registered at clinical trials.gov with ID NCT05624151 on November 21, 2022.
This prospective, randomized, controlled trial was carried out at the orthodontics and dentofacial surgery unit of Ain-Shams University hospitals. Patient enrollment was started on November 25, 2022, and ended on May 2, 2023. All patients’ guardians provided their written, informed consent. The Declaration of Helsinki's guiding principles were followed in conducting the study.
A total of 75 pediatric patients of both sexes, 3 months to 7 y old, with an ASA-PS I or II, scheduled for elective cleft lip repair (cheiloplasty) under GA, were enrolled.
Patients with local infection at the injection site, generalized sepsis, coagulopathy, thrombocytopenia, hemophilia, complex congenital heart disease, renal failure, major illnesses, allergy, or contraindications to the study medication, and parental or guardian’s dissent were excluded from the study.
During the preoperative visit, all patients underwent medical evaluation, focusing on the heart, lungs, and airways to identify any associated conditions or abnormalities. Routine laboratory investigations, e.g., a chest X-ray, complete blood count, and coagulation profile, were performed.
Instructions were passed to abstain from clear fluids like water and non-particulate juices for two hours, breast milk for four hours, formula or solid food for six hours, and fat-containing meals for eight hours.
Before induction of anesthesia, standard monitors were attached in the operating room, and basal readings for the patient's heart rate (HR), mean blood pressure (MBP), and oxygen saturation (SpO2) were recorded.
Conventional GA was administered to every child. Patients were randomly assigned into one of the three groups (25 in each group) using computer-generated randomization numbers with a closed-seal envelope.
The first group (Group D) received bilateral IONB before surgical incision with one ml of a mixture of bupivacaine 0.25% plus 0.5 μg/kg Dex, while patients in the 2nd group (Group M) received bilateral IONB with one ml of a mixture of bupivacaine 0.25% with 2 mg/kg MgSO4 to a maximum of 50 mg. Patients in the 3rd group (Group C) served as control, and received bilateral IONB with one ml of bupivacaine 0.25%.
Sevoflurane in an O2/air mixture (FiO2 = 0.8) with a sealed face mask was used to induce anesthesia in spontaneously breathing patients. A peripheral venous cannula was inserted after the patients' consciousness was lost. Fentanyl 1–2 μg/kg and propofol 1–2 mg/kg were administered to achieve a deep plane of anesthesia. Rocuronium 0.9 mg/kg was administered intravenously to facilitate endotracheal intubation with a preformed Ring–Adair–Elwyn (RAE) endotracheal tube, which was fixed centrally over the lower lip. Capnography confirmed the correct placement of the tube.
After fixing the endotracheal tube, pressure-controlled ventilation was adjusted to maintain normocapnia by continuously monitoring end-tidal CO2 for adequate ventilation. According to age and body weight, Ringer's solution was infused in all patients. Sevoflurane in O2/air mixture (FiO2 = 0.3) at 1% minimum alveolar concentration and rocuronium supplementation at 0.15 mg/kg were used to maintain anesthesia.
The technique of IONB
Bilateral IONB was performed on all participants using the intraoral approach before surgical repair. The upper lip was pulled back after the infraorbital foramen was palpated, and a 28 G needle was then advanced to the foramen parallel to the maxillary premolar.
The needle was advanced cephalad by positioning a finger at the level of the infraorbital foramen. After negative aspiration on each side, the target volume was injected (Figure 1).
A pediatric anesthesiologist with five years of experience in pediatric regional nerve blockade performed IONBs.
Cardiovascular monitoring (HR, MBP) was maintained throughout the procedure; readings were taken every 5 minutes and recorded at specific intervals (baseline, after intubation, 10 minutes after block, mid-operative, and after extubation). Any adverse events, such as bradycardia or hypotension, were immediately dealt with.
When the procedure was finished, inhalational anesthesia was stopped, the minimal to moderate amount of blood and oral secretions in the oropharynx were carefully suctioned, and reversal agents (atropine 10-15μg/kg and neostigmine 0.05 mg/kg) were administered once the neuromuscular blockade had sufficiently recovered and adequate spontaneous breathing had been regained. An infant who was awake, presented with regular breathing and had good muscle tone underwent extubation after his or her airway reflexes had returned.
Patients were then transported to the Post-Anesthesia Care Unit (PACU) when they were stable from both cardiovascular and respiratory standpoints. A pediatric anesthesiologist and nurse, who were blinded to the study methodology, observed them. Hemodynamic measurements were recorded in the PACU at Minute 30, as well as at intervals of 1, 2, 4, 6, 12, and 24 h starting from the time of patient arrival. The child was discharged to the ward after meeting the standard discharge criteria.
FLACC scale 15 was used by a blinded observer anesthesiologist to assess pain in patients during the first 24 h (ranging from 0–10, where 0 = no pain, 10 = worst pain), at the time of arrival to the PACU, at postoperative minute 30, and then at 1, 2, 4, 6, 12 and 24 h.
Acetaminophen was administered intravenously at a dosage of 10 mg/kg whenever the FLACC Score was greater than 4. If the FLACC score was ≥ 4, the dose was repeated every six hours until they could tolerate oral intake. The time to the first analgesic requirement and the total acetaminophen consumption over the first 24 h postoperatively were recorded.
The Pediatric Anesthesia Emergence Delirium (PAED) scale 16 was used to measure the incidence of emergence agitation at 0, 5, 10, 20, 30, and 60 min. Additionally, postoperative vomiting (POV) within the first 24 h following surgery was noted. If POV developed, ondansetron 0.1 mg/kg was prescribed intravenously.
Hypotension, bradycardia, shivering, and respiratory depression were among the other adverse side effects that were noted. The primary outcome was the time to the first analgesic request, while the secondary outcomes were the total amount of acetaminophen consumed in the first 24 h following surgery, pain assessments, and adverse drug reactions.
Sample size calculation
Using the STATA program, the sample size was calculated with the type 1 error (α) set to 0.05 and the power (1-β) set to 0.9. The result from a previous study by Sayed et al.,17 showed that there was a significant difference between the study groups concerning the frequency of acetaminophen administrations; as 63% of cases in the Group D had paracetamol more than one time, compared to only 13% of patients of Group M. Calculation according to these values produced a sample size of 22 cases per group. To compensate for drop-outs, we included 25 cases in each group (a total sample of 75 cases).
Statistical methodology
The gathered data were coded, tabulated, and statistically analyzed using IBM SPSS statistics (Statistical Package for Social Sciences) software, version 28.0, IBM Corp., Chicago, USA, 2021. Shapiro-Wilk test was used to determine the normality of quantitative data, which was followed by mean and SD (standard deviation) descriptions and an ANOVA test to compare them. For variables with low expected values, Fisher's Exact and Chi-Square tests were used to compare qualitative data that are expressed as numbers and percentages. Pairwise comparisons were made by using the post hoc Bonferroni test. P < 0.050 was considered significant.
3. RESULTS
The study's eligibility requirements were checked on 86 patients. Four patients did not meet the inclusion criteria, and seven patient guardians declined to participate, resulting in the exclusion of eleven patients. In the end, 75 patients—25 for each group—completed the study and their data were analyzed (Figure 2).
Patients in the three groups didn’t differ regarding their demographic data (age, weight, sex, ASA-PS), repair type, and duration of surgery or anesthesia (Table 1).
There was no significant difference in all groups regarding HR and MBP in the intraoperative time (baseline, after intubation, 10 min after block, and mid-operative) as well as from postoperative min-0 to 4 h. HR and MBP at 6, 12, and 24 h were the lowest in the Group D, followed by the Group M, and the highest in the Group C, the differences were significant only in the Group D at 6 h, while the differences were between all the study groups at 12 and 24 h.
| Table 1. Comparison regarding baseline characteristics | ||||||
| Variables | Group D
(n = 25) |
Group M
(n = 25) |
Group C
(n = 25) |
p-value | ||
| Age (y) | < 1 | 15 (60.0) | 16 (64.0) | 14 (56.0) | #0.846 | |
| 1 – 7 | 10 (40.0) | 9 (36.0) | 11 (44.0) | |||
| Sex | Male | 16 (64.0) | 18 (72.0) | 19 (76.0) | #0.637 | |
| Female | 9 (36.0) | 7 (28.0) | 6 (24.0) | |||
| Weight (kg) | 15.8 ± 5.3 | 15.9 ± 5.6 | 16.5 ± 3.4 | ^0.866 | ||
| ASA (n, %) | I | 19 (76.0) | 22 (88.0) | 19 (76.0) | #0.472 | |
| II | 6 (24.0) | 3 (12.0) | 6 (24.0) | |||
| Repair type
|
Primary | 18 (72.0) | 20 (80.0) | 17 (68.0) | #0.620 | |
| Revision | 7 (28.0) | 5 (20.0) | 8 (32.0) | |||
| Duration of surgery (min) | 100.7 ± 9.9 | 98.4 ± 9.6 | 96.1 ± 17.4 | ^0.444 | ||
| Duration of anesthesia (min) | 117.5 ± 10.3 | 115.8 ± 10.1 | 114.3 ± 17.3 | ^0.685 | ||
| Data presented as Mean ± SD or n (%). ^ANOVA test. #Chi square test. §Fisher’s Exact test. | ||||||
Postoperative pain scores at different time points were non-significantly lowest in the Group D, followed by the Group M, and were the highest in the Group C, the differences were significant only in the Group C at 6 h, while the differences were between all the study groups at 12 and 24 h (Figure 3).
Time to first requested analgesia was significantly longest in the Group D, followed by the Group M, and shortest in the Group C (13.9 ± 1.7 h, 11.5 ± 2.0 h, 5.9 ± 1.3 h) respectively (Figure 4).
In addition, the rate of analgesic doses was significantly less frequent in the Group D followed by Mgso4, and more frequent in the Group C. Furthermore, total postoperative acetaminophen consumption was significantly lower in the Group D, followed by the Group M, and highest in the Group C (Figure 4).
Regarding postoperative side effects, emergence agitation, and POV were non-significantly less frequent in the Group D, followed by the Group M, and most frequent in the Group C. PAED scale at different time points was non-significantly lowest in the Group D, followed by the Group M, and highest in the Group C. Sedation was non-significantly most frequent in the Group D, followed by the Group M, and least frequent in the Group C. Bradycardia non-significantly occurred only in the Group D. Hypotension was non-significantly least frequent in the Group M, with equal incidences in Group D and Group C. Shivering was non-significantly most frequent in the Group C, with equal incidences in Group M and Group C. Respiratory depression did not occur in all studied groups (Table 2).
| Table 2. The comparison regarding PAED score and postoperative side effects | |||||
| Time | Group D
(n = 25) |
Group M
(n = 25) |
Group C
(n = 25) |
p-value | |
| Emergence agitation | 4 (16.0%) | 5 (20.0%) | 7 (28.0%) | #0.573 | |
| PAED scale | Min-0 | 6.8 ± 4.3 | 7.7 ± 4.7 | 8.0 ± 5.2 | ^0.612 |
| Min-5 | 6.0 ± 4.0 | 6.8 ± 4.5 | 7.1 ± 5.2 | ^0.652 | |
| Min-10 | 4.4 ± 3.7 | 5.2 ± 4.0 | 5.8 ± 5.2 | ^0.488 | |
| Min-20 | 3.2 ± 2.8 | 3.8 ± 3.5 | 4.2 ± 4.4 | ^0.618 | |
| Min-30 | 1.8 ± 1.7 | 2.2 ± 2.7 | 2.7 ± 3.6 | ^0.535 | |
| Min-60 | 0.7 ± 1.1 | 0.9 ± 1.5 | 1.2 ± 2.2 | ^0.596 | |
| Vomiting | 1 (4.0) | 2 (8.0) | 4 (16.0) | §0.487 | |
| Sedation | 4 (16.0) | 2 (8.0) | 0 (0.0) | §0.155 | |
| Bradycardia | 3 (12.0) | 0 (0.0) | 0 (0.0) | §0.102 | |
| Hypotension | 3 (12.0) | 2 (8.0) | 3 (12.0) | §0.999 | |
| Shivering | 1 (4.0) | 1 (4.0) | 5 (20.0) | §0.200 | |
| Respiratory depression | 0 (0.0) | 0 (0.0) | 0 (0.0) | NA | |
| Data presented as Mean ± SD unless mentioned otherwise. PO: Postoperative. NA: Not applicable. ^ANOVA test. *Significant. Homogenous groups had the same symbol “a,b,c" based on the post hoc Bonferroni test. | |||||
4. DISCUSSION
Perioperative pain management after cleft lip repair is very challenging, as the procedure is very painful and it's difficult to assess and manage pain at this age. We aimed for effective prolonged analgesia to avoid a vigorous child in pain which is considered as one of the risk factors for postoperative bleeding.
Our results reported that the time to first request rescue analgesia was significantly increased in the dexmedetomidine group, followed by the MgSO4 group, and shortest in the control group. The total acetaminophen dose needed was significantly lowest in the Group D, followed by the Group M, and highest in the Group C.
Opioids are widely used for the treatment of moderate to severe pain in pediatric patients, particularly in the immediate postoperative period. However, opioids are associated with a range of side effects, including nausea, vomiting, constipation, urinary retention, pruritus, sedation, respiratory depression, and opioid-induced hyperalgesia.18,19,20 Opioid‐sparing approaches to postoperative analgesia, including IONB should be considered to avoid the complications of opioids during postoperative recovery.
El-Emam EM at al.21 compared Dex against dexamethasone as adjuvants for bupivacaine in IONB and they noticed that Dex resulted in a more prolonged duration of analgesia and lower pain scores. Our study results are consistent with the study by Sumalatha G et al., who showed that 0.5 μg/kg Dex added to bupivacaine increased the duration of analgesia when compared to plain bupivacaine in IONB in children undergoing cleft lip surgery, and the number of patients who requested rescue analgesics were less.22 Other studies supported our results, and proved that the addition of Dex to ropivacaine in supraclavicular brachial plexus block significantly prolongs the duration of analgesia.23,24
Dexmedetomidine and other alpha-2 selective adrenergic agonists are effective analgesics when combined with local anesthetics for peripheral blocks.25 It inhibits current channels that help neurons return from a hyperpolarized state to their normal resting potential. Dex also selectively prevents C-fiber neurons from firing additional action potentials, causing analgesia. The majority of analgesic and sedative effects on the CNS are mediated by α2A-subtype receptors.26
On the other hand, the addition of MgSO4 as an adjuvant to bupivacaine as explained by Verma V, et al., significantly prolongs the duration of analgesia and decreases the analgesic requirement in ultrasound-guided supraclavicular brachial plexus block.27 Similarly, he concluded that MgSO4 and ketamine were effective as adjuvants to levobupivacaine in erector spinae block for postoperative analgesia in breast cancer surgery, but with better analgesia provided by MgSO4.
MgSO4 is an N-methyl-d-aspartate (NMDA) receptor antagonist that works to reduce excitatory neurotransmission by restricting intracellular calcium levels through NMDA receptor antagonism.29 Contrary to our results, Sayed et al. investigated and proved that magnesium had a prolonged analgesic effect compared with Dex.
We demonstrated in our results that postoperative pain perception at different time points was lowest in the Group D with a more frequent sedation level, followed by Group M and the highest pain perception with the least sedation level in the control group, Simultaneously, these differences were recorded by a systematic review and meta-analysis conducted by Vorobeichik et al. that perineural Dex was followed by excessive postoperative sedation that was recorded using many scales.30 On the other hand, Obayah et al. did not demonstrate a sedative effect in their result but, this can be due to the heterogeneity of the scales used.31
Side effects demonstrated in our study as POV was non-significantly less frequent in the dexmedetomidine group, followed by the MgSO4 group, and most frequent in the control group, and there were no other serious side effects. Our results were concomitant with Elsonbaty M, et al.32 who proved that, the IONB technique has minimal complication rate with greater parental satisfaction. Other researchers proved that Dex and MgSO4 as adjuvants showed satisfactory pain relief without serious side effects. 21,28
Our study recorded no relevant intraoperative and postoperatively cardiovascular events. The heart rate remained on the lower side in the Group D but did not require any intervention. Consistent with our results, the results of several studies have demonstrated that Dex can prolong analgesia significantly without inducing significant hypotension, or bradycardia.21,31
5. CONCLUSION
Our results suggest that there is a benefit of adding dexmedetomidine or MgSO4 to bupivacaine in IONB in cleft lip surgery. However, dexmedetomidine demonstrated superiority compared to MgSO4 concerning prolonged postoperative analgesia.
6. Data availability
The numerical data is available with the corresponding author and can be provided on request.
7. Conflict of interests
The authors declare no conflict of interest. No funding, either internal or external, was involved in this study.
8. Ethical approval
This prospective, randomized, clinical study was approved by the University of Ain Shams Institutional ethics board review (FMASU R176/2022).
9. Authors' contribution
MA: Concept, data collection, data analysis, literature search, revised and approved the manuscript.
AA, MM and MA: Designed the study protocol, manuscript writing and editing, literature search, revised and approved the manuscript.
10. REFERENCES
- Denning S, Ng E, Wong Riff KWY. Anaesthesia for cleft lip and palate surgery. BJA Educ. 2021;21(10):384-389. [PubMed] DOI: 1016/j.bjae.2021.06.002
- Feriani G, Hatanaka E, Torloni MR, da Silva EM. Infraorbital nerve block for postoperative pain following cleft lip repair in children. Cochrane Database Syst Rev. 2016;4(4):CD011131. [PubMed] DOI: 1002/14651858.CD011131.pub2
- Jöhr M. Regional anaesthesia in neonates, infants and children: an educational review. Eur J Anaesthesiol. 2015;32(5):289-97. [PubMed] DOI: 1097/EJA.0000000000000239
- Ping Y, Ye Q, Wang W, Ye P, You Z. Dexmedetomidine as an adjuvant to local anesthetics in brachial plexus blocks: A meta-analysis of randomized controlled trials. Medicine (Baltimore). 2017;96(4):e5846. [PubMed] DOI: 1097/MD.0000000000005846
- Mason KP, Lerman J. Review article: Dexmedetomidine in children: current knowledge and future applications. Anesth Analg. 2011;113(5):1129-42. [PubMed] DOI: 1213/ANE.0b013e31822b8629
- Sivakumar RK, Panneerselvam S, Cherian A, Rudingwa P, Menon J. Perineural vs. intravenous dexmedetomidine as an adjunct to bupivacaine in ultrasound guided fascia iliaca compartment block for femur surgeries: A randomised control trial. Indian J Anaesth. 2018;62(11):851-857. [PubMed] DOI: 4103/ija.IJA_397_18
- Abdallah FW, Dwyer T, Chan VW, Niazi AU, Ogilvie-Harris DJ, Oldfield S, et al. IV and Perineural Dexmedetomidine Similarly Prolong the Duration of Analgesia after Interscalene Brachial Plexus Block: A Randomized, Three-arm, Triple-masked, Placebo-controlled Trial. Anesthesiology. 2016;124(3):683-95. [PubMed] DOI: 1097/ALN.0000000000000983
- Telci L, Esen F, Akcora D, Erden T, Canbolat AT, Akpir K. Evaluation of effects of magnesium sulphate in reducing intraoperative anaesthetic requirements. Br J Anaesth. 2002;89(4):594-8. [PubMed] DOI: 1093/bja/aef238
- Woolf CJ, Thompson SWN. The induction and maintenance of central sensitization is dependent on N-methyl-D-aspartic acid receptor activation; implications for the treatment of post-injury pain hypersensitivity states. Pain. 1991;44(3):293-299. [PubMed] DOI: 1016/0304-3959(91)90100-C
- Herroeder S, Schönherr ME, De Hert SG, Hollmann MW. Magnesium--essentials for anesthesiologists. Anesthesiology. 2011;114(4):971-93. [PubMed] DOI: 1097/ALN.0b013e318210483d
- Do SH. Magnesium: a versatile drug for anesthesiologists. Korean J Anesthesiol. 2013;65(1):4-8. [PubMed] DOI: 4097/kjae.2013.65.1.4
- Sun J, Wu X, Zhao X, Chen F, Wang W. Pre-emptive peritonsillar infiltration of magnesium sulphate and ropivacaine vs. ropivacaine or magnesium alone for relief of post-adenotonsillectomy pain in children. Int J Pediatr Otorhinolaryngol. 2015;79(4):499-503. [PubMed] DOI: 1016/j.ijporl.2015.01.009
- Kim EM, Kim MS, Han SJ, Moon BK, Choi EM, Kim EH, et al. Magnesium as an adjuvant for caudal analgesia in children. Paediatr Anaesth. 2014;24(12):1231-8. [PubMed] DOI: 1111/pan.12559
- Rajamani A, Kamat V, Rajavel VP, Murthy J, Hussain SA. A comparison of bilateral infraorbital nerve block with intravenous fentanyl for analgesia following cleft lip repair in children. Paediatr Anaesth. 2007;17(2):133-9. D [PubMed] DOI: 1111/j.1460-9592.2006.02032.x
- Voepel-Lewis T, Zanotti J, Dammeyer JA, Merkel S. Reliability and validity of the face, legs, activity, cry, consolability behavioral tool in assessing acute pain in critically ill patients. Am J Crit Care. 2010;19(1):55-61. [PubMed] DOI: 4037/ajcc2010624
- Russell PSS, Mammen PM, Shankar SR, Viswanathan SA, Rebekah G, Russell S, et al. Pediatric Anesthesia Emergence Delirium Scale: A diagnostic meta-analysis. World J Clin Pediatr. 20229;11(2):196-205. [PubMed] DOI: 5409/wjcp.v11.i2.196
- Sayed JA, Kamel EZ, Riad MAF, Abd-Elshafy SK, Hanna RS. Dexmedetomidine with magnesium sulfate as adjuvants in caudal block to augment anesthesia and analgesia in pediatric lower abdominal surgeries. Egyptian J of Anesthesia. 2018;34:115-122. DOI: 1016/j.egja.2018.06.001
- Romberg R, Sarton E, Teppema L, Matthes HW, Kieffer BL, Dahan A. Comparison of morphine-6-glucuronide and morphine on respiratory depressant and antinociceptive responses in wild type and mu-opioid receptor deficient mice. Br J Anaesth. 2003;91(6):862-70. [PubMed] DOI: 1093/bja/aeg279
- Nee J, Zakari M, Sugarman MA, Whelan J, Hirsch W, Sultan S, et al. Efficacy of Treatments for Opioid-Induced Constipation: Systematic Review and Meta-analysis. Clin Gastroenterol Hepatol. 2018;16(10):1569-1584.e2. [PubMed] DOI: 1016/j.cgh.2018.01.021
- Konopka KH, van Wijhe M. Opioid-induced hyperalgesia: pain hurts? Br J Anaesth. 2010;105(5):555-7. [PubMed] DOI: 1093/bja/aeq286
- El-Emam EM, El Motlb EAA. Comparative Evaluation of Dexamethasone and Dexmedetomidine as Adjuvants for Bupivacaine in Ultrasound-Guided Infraorbital Nerve Block for Cleft Lip Repair: A Prospective, Randomized, Double-Blind Study. Anesth Essays Res. 2019;13(2):354-358. [PubMed] DOI: 4103/aer.AER_14_19
- Sumalatha G, Ravichandra R. Dexmedetomidine as an adjuvant to infraorbital block in children undergoing cleft lip surgery – A clinical comparative study. Indian J Clin Anaesth. 2020;7:12-5. DOI: 18231/j.ijca.2020.004
- Hamed MA, Ghaber S, Reda A. Dexmedetomidine and Fentanyl as an Adjunct to Bupivacaine 0.5% in Supraclavicular Nerve Block: A Randomized Controlled Study. Anesth Essays Res. 2018;12(2):475-479. [PubMed] DOI: 4103/aer.AER_50_18
- Mangal V, Mistry T, Sharma G, Kazim M, Ahuja N, Kulshrestha A. Effects of dexmedetomidine as an adjuvant to ropivacaine in ultrasound-guided supraclavicular brachial plexus Block: A prospective, randomized, double-blind study. J Anaesthesiol Clin Pharmacol. 2018;34(3):357-361. [PubMed] DOI: 4103/joacp.JOACP_182_17
- Verma V, Rana S, Chaudhary SK, Singh J, Verma RK, Sood S. A dose-finding randomised controlled trial of magnesium sulphate as an adjuvant in ultrasound-guided supraclavicular brachial plexus block. Indian J Anaesth. 2017;61(3):250-255. [PubMed] DOI: 4103/ija.IJA_466_16
- Schnabel A, Reichl SU, Weibel S, Kranke P, Zahn PK, Pogatzki-Zahn EM, et al. Efficacy and safety of dexmedetomidine in peripheral nerve blocks: A meta-analysis and trial sequential analysis. Eur J Anaesthesiol. 2018;35(10):745-758. [PubMed] DOI: 1097/EJA.0000000000000870
- Fairbanks CA, Stone LS, Wilcox GL. Pharmacological profiles of alpha 2 adrenergic receptor agonists identified using genetically altered mice and isobolographic analysis. Pharmacol Ther. 2009;123(2):224-38. [PubMed] DOI: 1016/j.pharmthera.2009.04.001
- El Sherif FA, Youssef HA, Fares KM, Mohamed SA, Ali AR, Thabet AM. Efficacy of Ketamine versus Magnesium Sulphate as Adjuvants to Levobupivacaine in Ultrasound Bilevel Erector Spinae Block in Breast Cancer Surgery (a Double-Blinded Randomized Controlled Study). Local Reg Anesth. 202223;15:87-96. [PubMed] DOI: 2147/LRA.S379194
- Kaptanoglu E, Beskonakli E, Solaroglu I, Kilinc A, Taskin Y. Magnesium sulfate treatment in experimental spinal cord injury: emphasis on vascular changes and early clinical results. Neurosurg Rev. 2003;26(4):283-7. [PubMed] DOI: 1007/s10143-003-0272-y
- Vorobeichik L, Brull R, Abdallah FW. Evidence basis for using perineural dexmedetomidine to enhance the quality of brachial plexus nerve blocks: a systematic review and meta-analysis of randomized controlled trials. Br J Anaesth. 2017;118(2):167-181. [PubMed] DOI: 1093/bja/aew411
- Obayah GM, Refaie A, Aboushanab O, Ibraheem N, Abdelazees M. Addition of dexmedetomidine to bupivacaine for greater palatine nerve block prolongs postoperative analgesia after cleft palate repair. Eur J Anaesthesiol. 2010;27(3):280-4. [PubMed] DOI: 1097/EJA.0b013e3283347c15
- Elsonbaty M, Maher M, Reda A, Sarhan K. Peri-Operative Pain Management for Cleft Lip Repair in Children, Bilateral Infraorbital Nerve Block Versus Combined Intravenous Fentanyl with Peri-Incisional Infiltration. A Randomized Comparative Study. Egyptian J Hospital Med. 2021;82(1):25-31. [FreeFullText]