Abstract
Methodology: We enrolled 30 patients (14 males and 16 females) with chronic neck pain and respiratory dysfunction fulfilling inclusion criteria. Two trials of CAROM measurement for flexion, extension, left and right lateral flexion and left and right rotation were performed, with a gap of one week to measure test retest reliability of CROM device. Intraclass correlation coefficient (ICC), standard errors of measurement (SEM) and minimal detectable change (MDC) were calculated to test the intrarater reliability.
Results: Intrarater reliability of repeated measurements of CAROM using the CROM device was found to be good. The ICC values ranged between 0.88-0.97 for flexion, 0.93-0.98 for extension, 0.92-0.98 for right lateral flexion,0.93-0.98 for left lateral flexion. For right rotation it was 0.88-0.97, for left lateral rotation it was 0.95-0.99. The standard error of measurement for these movements ranged from 1.5° to 2.9°. Minimal detectable change ranged from 3.5°for extension to 6.8°for left lateral flexion.
Conclusion: Cervical range of motion device is a reliable tool for measuring cervical active range of motion in patients simultaneously suffering from chronic neck pain and respiratory dysfunction.
Abbreviations: CAROM - cervical active range of motion; CROM - cervical range of motion; ICC - Intraclass correlation coefficient; SEM - standard errors of measurement; MDC - minimal detectable change
Key words: Adult; Exercise Therapy / methods; Female; Humans; Male; Neck Pain / physiopathology; Neck Pain / therapy; Pain Measurement; Pulmonary function; Range of Motion, Articular; Reliability
Citation: Anwar S, Arsalan SA, Zafar H, Ahmad A, Gillani SA, Hanif A. Intrarater reliability of cervical range of motion device in measuring cervical active range of motion in patients with chronic neck pain and respiratory dysfunction. Anaesth. pain intensive care 2022;26(4):503-509; DOI: 10.35975/apic.v26i4.1957
Received: September 29, 2021; Reviewed: April 21, 2022; Accepted: May 10, 2022
Introduction
Patients suffering from chronic neck pain can experience associated musculoskeletal disorders mostly due to compensatory postural adjustments and muscle activation patterns.1,2 Emerging new technologies and gadgets are causing more postural problems than ever and are contributing to the increased prevalence of neck pain;3 although any correlation between neck pain and the duration of usage of these devices is not established.4,5
Some chronic neck pain patients can also develop respiratory dysfunction.6 In the recent past many studies have investigated the impact of chronic neck pain on respiratory functions.7,8,9 Respiration is a multidimensional phenomenon which is influenced by number of factors such as biomechanical, biochemical, physiological, psychological and social.10 Major neck related factors having negative influence on normal respiratory function are reported to be (a) the decreased strength of deep neck flexors and extensors, (b) the hyperactivity and increased fatigability of superficial neck flexors, (c) the limitation of range of motion of neck (d) the decrease in proprioception and disturbances in neuromuscular control of neck (e) the existence of chronic pain in neck and back and many other factors.11,12,13,14
Cervical spine has unique kinetics allowing movement in all six directions, i.e. flexion, extension, side flexion and rotation on both sides. It has a crucial role in supporting the weight of head and providing anchorage to the associated respiratory muscles proximally, so that they can participate in the necessary function of respiration on another end. Any alteration in the cervical spine kinetics can influence the action of one muscle over the other by altering force length curve, and thus altering their force exerting properties.15,16 It is reported that chronic neck pain causes inhibition of core muscles of the neck (longus coli, longus capitis) and increased activation of superficial muscles such as sternocleidomastoid and anterior scalene.17,18 As chronic neck pain patients assume a forward head posture a correlation study conducted on 33 healthy subjects demonstrated a strong negative correlation between craniovertebral angle and sternocleidomastoid activation ratio.19 Muscular imbalance, postural changes and segmental instability due to weakness of deep neck muscles may contribute to thoracic spine instability and changes in rib cage mechanics.20,21 Changes in Proprioceptive feedback, psychological influence of pain and resulting kinesiophobia can further exaggerate the respiratory dysfunction. Increased neck muscle fatigability, decreased cervical range of motion (CROM) due to pain can further contribute to changes in biomechanics of ribs which can finally lead to respiratory dysfunction.6
CROM is a valid objective outcome measure in clinical setups.22 It not only helps in differentiating articular dysfunction from non-articular dysfunction but also it is one of the strongest parameters to be used as baseline assessment and to record progression in the treatment. Many studies have been conducted to assess quantitative measurement of cervical active range of motion.23 The different studies have shown that the CROM device,24 the Spin-T goniometer25 and the universal goniometer,26 were valid and reliable for this purpose.24 Audette et al. compared the CROM device reliability in 20 healthy subjects with the fast track motion analysis system, and found that the test retest reliability of the CROM device was good with intraclass correlation coefficient (ICC) values ranging between 0.89-0.98.27 A recent study by on healthy adults measured reliability of CROM device with a week interval and found it to be moderate to good with ICC values ranging between 0.65-0.28 Many other studies have assessed the intrarater reliability of CROM device on healthy as well as patient population and concluded that results with CROM device were reproducible within the same session.29
Patients who suffer from chronic neck pain show a decline in optimal respiratory function and often assume a forward neck posture due to over activation of superficial neck flexors.18 This posture somehow compromises the actual ranges measured with CROM device. Although the reliability of the CROM device has previously been evaluated in healthy subjects as well as in patients suffering from different conditions, but not in patients simultaneously suffering from chronic neck pain and respiratory dysfunction. Therefore, we evaluated the intrarater reliability of CROM device in patients simultaneously suffering from chronic neck pain and respiratory dysfunction.
Methodology
A total of 30 patients, consisting of 14 males and 16 females, suffering from neck pain and mild respiratory dysfunction were recruited through effect size method to obtain a statistical power of 0.80 and an effect size of 0.6. After approval from ethical committee of University of Lahore, permission was also obtained from the hospital administration for data collection. The patients visiting physiotherapy department of the university hospital for the treatment of neck pain were recruited from March to August 2020. Written informed consent was obtained from each participant prior to the study.


Participants between the age of 25-50 years, with neck pain for more than 3 months, pain score of ≥ 3 on visual analogue scale (VAS), and FEV1/FVC ratio between 60-69% of the predicted ratio were eligible for the study.


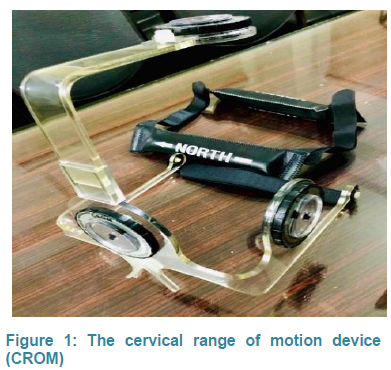
The age range of 25-50 y was based on the fact that with increasing age the pliability of lungs gradually decreases. Mild pain < 3 is unlikely to be accompanied by a respiratory dysfunction. FEV1/FVC% less than 60 is indicative of severe respiratory illness and value more than 69% is indicative of no respiratory dysfunction at all. FEV1/FVC ratio was calculated through pulmonary function testing with a portable spirometer ‘MIR Spirolab 4™’, in sitting position by a trained respiratory technician. Whereas patients with neck pain of traumatic origin, and congenital deformity of cervical spine were excluded.29 The ‘CROM Basic’ by Performance Attainment AssociatesTM is a device to measure cervical ROM during flexion/extension, left / right lateral flexion and left / right rotation (Figure 1). Two gravity-based inclinometers positioned in the sagittal and frontal planes, measure lexion/extension
and lateral flexion, respectively. Whereas a magnet base compass like gadget positioned in the transverse plane above the head, measures cervical rotation movement with the help of magnets placed on the thorax. Both the inclinometers and the compass like gadget are attached to a plastic frame that fits on the head conveniently and is secured by Velcro straps.30
Six cervical movements; flexion/extension, left and right-side flexion and left and right rotations were demonstrated in front of each participant. Patients were thoroughly guided to maintain a neutral head and neck position with gaze pointing straight throughout the testing procedures. Starting position was a neutral head and neck position with straight back against a wooden chair, arms by the side while shoulders were relaxed and tilted backwards. Knees were bent at 90° while feet lied flat on the ground. Patients were asked to perform all six movements with evaluator’s cues to get familiar
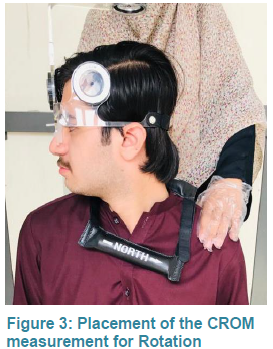
with the whole test. For flexion and extension patient was guided to perform full range flexion after tucking the chin in (Figure 2). Similarly, extension was performed after chin raised up to participants’ limit. For side flexion and rotations patients were advised not to move their shoulders and look forward (Figure 3, Figure 4).
CROM device was placed on the patient’s head with adjustment of nose clip and magnetic collar was hanged around shoulder to prevent any rotation of the trunk. The patients were asked to perform all six cervical range of movements. The order of the movement performed was randomly picked by every patient from
a list of all six movements. For flexion /extension and both side flexions relevant dial of inclinometer was read by the author at start of the movement and at the end range. For rotation, dial was set at zero and movement was performed in the same manner. Values were recorded by the recorder. The same set of measurements was performed one week after the first measurement. The order of the measurement was randomized by a similar method and evaluator was blind about the previous values. Recorder bias was minimized by testing of active range of motion (AROM) which is purely under patient’s control. Procedure was performed by a registered physical therapist who had specialized in orthopedic manual physical therapy with 10-year clinical experience, including the use of CROM.
Statistical analysis
Data was analyzed using SPSS software version 21.
Normality of data was checked through histograms, which was normally distributed. Descriptive statistics were calculated in the form of means and standard deviations for the age, VAS score, FEV1/FVC ratio and for all six ranges of motion of neck.
To determine the test-retest reliability of the CROM measurements, the ICC mixed model 3,1 designated as 2 -way analysis of variance (ANOVA) for absolute agreement of single measure with 95% confidence interval (CI) was used.
The standard error of the measurement (SEM) was calculated using the following formula;
SEM=SD√1-rα. (r; reliability of the measure).34 The minimal detectable change at the 90% CI was calculated as MDC90 equals 1.65(z score for 90%CI)*SEM*√2.
Results
Based on the inclusion and exclusion criteria, 30 subjects, (14 male and 16 females) were included in the study. Descriptive statistics of the baseline values are described in Table 1.
Table 2 shows the descriptive and intrarater reliability statistics for measurements of cervical active range of motion (CAROM) in patients with chronic neck pain and respiratory dysfunction in session 1 and session 2. The intraclass coefficient values for intrarater reliability were; flexion 0.94 (0.88-0.97), extension 0.97 (0.93-0.98), right lateral flexion 0.96 (0.92-0.98), left lateral flexion 0.96 (0.93-0.98) right rotation 0.94 (0.88-0.97) and left lateral rotation 0.95 (0.95-0.99). The standard error of measurement ranges from 1.5° to 2.9°. Standard error of measurements were; flexion 2.6° extension 1.5°, right lateral flexion 2.9°, left lateral flexion 2.9°, right rotation 2.5° and left rotation 2°.
Discussion
This study was conducted to assess the reliability of results by CROM device in patients simultaneously suffering from neck pain and respiratory dysfunction. According to the results it is clear that ICC values were greater than 0.90, which show that CROM device for calculation of CAROM in patients with neck pain and respiratory dysfunction has excellent reliability. The intraclass coefficient above 0.90 for all six ranges lies in excellent range according to ICC model interpretation.32
Wolan et al. assessed inter and intrarater reliability of CROM device on 95 healthy individuals between ages of 20-24 y, and the difference at two weeks in retesting. According to their findings highest intrarater and
interrater concordance was observed in the measure of extension. Result of the present study shows similar trend where ICC value for cervical extension (0.97) was the highest when compared to ICC values from the other five analyzed movements. However, healthy population with age (20-25 y) was included in their study. Our study was different than previous CROM reliability studies as it was conducted in patients who suffered from neck pain along with respiratory dysfunction and investigated the CAROM in all six possible ranges with strict protocols and clear methods.33
The results of this study are in coherence with another study on neck pain patients in which average ICCs for CROM device was greater than 0.80; whereas, ICCs values for universal goniometer and visual estimation were less than 0.80.34 The three tools (CROM device, universal goniometer and visual screening) were used in 3 data collection sessions and 60 subjects were tested in three groups having 20 subjects in each group. However, the methodology of this study is different in terms of measurement of six planes of CAROM instead of a single plane in the said study. In a study for reproducibility of cervical active and passive range measurements after sub-acute whiplash disorder CROM device was found to be a reliable tool with ICC range (0.82-0.99).35 In this study 39 and 19 subjects were tested for intra and inter-observer studies respectively, both active and passive cervical ranges were measured and CROM was proved to be a reliable device for symptomatic neck pain patients. Apart from reliability measurement calculation of SEM and MDC are additional merits of this study; however, only active cervical ranges were observed, whereas Williams et al. measured passive range of motion as well. In another study CROM device was found useful in repositioning head accuracy and reliable in measurement of cervical ranges in patients with cervical radiculopathy.36
According to a systematic review by Williams et al. in a number of studies reliabilities of CROM device has been proved. Fifty-six studies were reviewed and 12 different methods were evaluated. Most of the studies were conducted on healthy population or to measure a single particular range such as flexion-extension of neck or forward head posture. In another study, researchers evaluated the intrarater reliability of CROM device for measuring proprioception of cervical spine in healthy individuals and described it to be a reliable tool.37 Apart from the difference of neck pain population studied in this study it has an additional merit of measuring standard error of measurement and minimal detectable change, which was lacking in the study by Reddy et al. In another study CROM device showed high reliability in patients suffering from migraine but only 50 young females with average age 35 y were studied.38 Our study minimized the gender bias by including both genders.
Limitations
We measured only the intrarater reliability, in a small sample. Future researchers should explore this phenomenon with large population assessing both interrater and intrarater reliability. It is necessary to rule out more factors which may influence the objective outcome measures of cervical spine due to coexistence of respiratory dysfunction.
Conclusion
CROM device is a reliable tool for intrarater analysis in measuring cervical active range of motion in patients with chronic neck pain and respiratory dysfunction. This device seems to be reliable in measuring cervical active range of motion in all six directions.
Trial registration
Registered as Trial No. IRCT 20200226046623N1 https://www.irct.ir/trial/46240
Data availability
The numerical data generated in this study is available with the authors.
Disclaimer
This study is based on an ongoing trial conducted as a part of PhD study at University of Lahore.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared by the authors.
Author contribution
SA: Conception and design of the study, Data collection, Data interpretation, Drafting
HZ: Drafting
AA: Data interpretation, Drafting
AH: Statistical Analysis
All authors read the final draft and approved.
References
Methodology: We enrolled 30 patients (14 males and 16 females) with chronic neck pain and respiratory dysfunction fulfilling inclusion criteria. Two trials of CAROM measurement for flexion, extension, left and right lateral flexion and left and right rotation were performed, with a gap of one week to measure test retest reliability of CROM device. Intraclass correlation coefficient (ICC), standard errors of measurement (SEM) and minimal detectable change (MDC) were calculated to test the intrarater reliability.
Results: Intrarater reliability of repeated measurements of CAROM using the CROM device was found to be good. The ICC values ranged between 0.88-0.97 for flexion, 0.93-0.98 for extension, 0.92-0.98 for right lateral flexion,0.93-0.98 for left lateral flexion. For right rotation it was 0.88-0.97, for left lateral rotation it was 0.95-0.99. The standard error of measurement for these movements ranged from 1.5° to 2.9°. Minimal detectable change ranged from 3.5°for extension to 6.8°for left lateral flexion.
Conclusion: Cervical range of motion device is a reliable tool for measuring cervical active range of motion in patients simultaneously suffering from chronic neck pain and respiratory dysfunction.
Abbreviations: CAROM - cervical active range of motion; CROM - cervical range of motion; ICC - Intraclass correlation coefficient; SEM - standard errors of measurement; MDC - minimal detectable change
Key words: Adult; Exercise Therapy / methods; Female; Humans; Male; Neck Pain / physiopathology; Neck Pain / therapy; Pain Measurement; Pulmonary function; Range of Motion, Articular; Reliability
Citation: Anwar S, Arsalan SA, Zafar H, Ahmad A, Gillani SA, Hanif A. Intrarater reliability of cervical range of motion device in measuring cervical active range of motion in patients with chronic neck pain and respiratory dysfunction. Anaesth. pain intensive care 2022;26(4):503-509; DOI: 10.35975/apic.v26i4.1957
Received: September 29, 2021; Reviewed: April 21, 2022; Accepted: May 10, 2022
Introduction
Patients suffering from chronic neck pain can experience associated musculoskeletal disorders mostly due to compensatory postural adjustments and muscle activation patterns.1,2 Emerging new technologies and gadgets are causing more postural problems than ever and are contributing to the increased prevalence of neck pain;3 although any correlation between neck pain and the duration of usage of these devices is not established.4,5
Some chronic neck pain patients can also develop respiratory dysfunction.6 In the recent past many studies have investigated the impact of chronic neck pain on respiratory functions.7,8,9 Respiration is a multidimensional phenomenon which is influenced by number of factors such as biomechanical, biochemical, physiological, psychological and social.10 Major neck related factors having negative influence on normal respiratory function are reported to be (a) the decreased strength of deep neck flexors and extensors, (b) the hyperactivity and increased fatigability of superficial neck flexors, (c) the limitation of range of motion of neck (d) the decrease in proprioception and disturbances in neuromuscular control of neck (e) the existence of chronic pain in neck and back and many other factors.11,12,13,14
Cervical spine has unique kinetics allowing movement in all six directions, i.e. flexion, extension, side flexion and rotation on both sides. It has a crucial role in supporting the weight of head and providing anchorage to the associated respiratory muscles proximally, so that they can participate in the necessary function of respiration on another end. Any alteration in the cervical spine kinetics can influence the action of one muscle over the other by altering force length curve, and thus altering their force exerting properties.15,16 It is reported that chronic neck pain causes inhibition of core muscles of the neck (longus coli, longus capitis) and increased activation of superficial muscles such as sternocleidomastoid and anterior scalene.17,18 As chronic neck pain patients assume a forward head posture a correlation study conducted on 33 healthy subjects demonstrated a strong negative correlation between craniovertebral angle and sternocleidomastoid activation ratio.19 Muscular imbalance, postural changes and segmental instability due to weakness of deep neck muscles may contribute to thoracic spine instability and changes in rib cage mechanics.20,21 Changes in Proprioceptive feedback, psychological influence of pain and resulting kinesiophobia can further exaggerate the respiratory dysfunction. Increased neck muscle fatigability, decreased cervical range of motion (CROM) due to pain can further contribute to changes in biomechanics of ribs which can finally lead to respiratory dysfunction.6
CROM is a valid objective outcome measure in clinical setups.22 It not only helps in differentiating articular dysfunction from non-articular dysfunction but also it is one of the strongest parameters to be used as baseline assessment and to record progression in the treatment. Many studies have been conducted to assess quantitative measurement of cervical active range of motion.23 The different studies have shown that the CROM device,24 the Spin-T goniometer25 and the universal goniometer,26 were valid and reliable for this purpose.24 Audette et al. compared the CROM device reliability in 20 healthy subjects with the fast track motion analysis system, and found that the test retest reliability of the CROM device was good with intraclass correlation coefficient (ICC) values ranging between 0.89-0.98.27 A recent study by on healthy adults measured reliability of CROM device with a week interval and found it to be moderate to good with ICC values ranging between 0.65-0.28 Many other studies have assessed the intrarater reliability of CROM device on healthy as well as patient population and concluded that results with CROM device were reproducible within the same session.29
Patients who suffer from chronic neck pain show a decline in optimal respiratory function and often assume a forward neck posture due to over activation of superficial neck flexors.18 This posture somehow compromises the actual ranges measured with CROM device. Although the reliability of the CROM device has previously been evaluated in healthy subjects as well as in patients suffering from different conditions, but not in patients simultaneously suffering from chronic neck pain and respiratory dysfunction. Therefore, we evaluated the intrarater reliability of CROM device in patients simultaneously suffering from chronic neck pain and respiratory dysfunction.
Methodology
A total of 30 patients, consisting of 14 males and 16 females, suffering from neck pain and mild respiratory dysfunction were recruited through effect size method to obtain a statistical power of 0.80 and an effect size of 0.6. After approval from ethical committee of University of Lahore, permission was also obtained from the hospital administration for data collection. The patients visiting physiotherapy department of the university hospital for the treatment of neck pain were recruited from March to August 2020. Written informed consent was obtained from each participant prior to the study.
| Figure 3: Placement of the CROM measurement for Rotation |
| Figure 1: The cervical range of motion device (CROM) |

| Figure 4: Placement of CROM for measurement of flexion. Please note the patient’s posture. |

| Figure 2: Placement of the CROM for lateral cervical flexion |
and lateral flexion, respectively. Whereas a magnet base compass like gadget positioned in the transverse plane above the head, measures cervical rotation movement with the help of magnets placed on the thorax. Both the inclinometers and the compass like gadget are attached to a plastic frame that fits on the head conveniently and is secured by Velcro straps.30
Six cervical movements; flexion/extension, left and right-side flexion and left and right rotations were demonstrated in front of each participant. Patients were thoroughly guided to maintain a neutral head and neck position with gaze pointing straight throughout the testing procedures. Starting position was a neutral head and neck position with straight back against a wooden chair, arms by the side while shoulders were relaxed and tilted backwards. Knees were bent at 90° while feet lied flat on the ground. Patients were asked to perform all six movements with evaluator’s cues to get familiar
with the whole test. For flexion and extension patient was guided to perform full range flexion after tucking the chin in (Figure 2). Similarly, extension was performed after chin raised up to participants’ limit. For side flexion and rotations patients were advised not to move their shoulders and look forward (Figure 3, Figure 4).
CROM device was placed on the patient’s head with adjustment of nose clip and magnetic collar was hanged around shoulder to prevent any rotation of the trunk. The patients were asked to perform all six cervical range of movements. The order of the movement performed was randomly picked by every patient from
a list of all six movements. For flexion /extension and both side flexions relevant dial of inclinometer was read by the author at start of the movement and at the end range. For rotation, dial was set at zero and movement was performed in the same manner. Values were recorded by the recorder. The same set of measurements was performed one week after the first measurement. The order of the measurement was randomized by a similar method and evaluator was blind about the previous values. Recorder bias was minimized by testing of active range of motion (AROM) which is purely under patient’s control. Procedure was performed by a registered physical therapist who had specialized in orthopedic manual physical therapy with 10-year clinical experience, including the use of CROM.
Statistical analysis
Data was analyzed using SPSS software version 21.
Normality of data was checked through histograms, which was normally distributed. Descriptive statistics were calculated in the form of means and standard deviations for the age, VAS score, FEV1/FVC ratio and for all six ranges of motion of neck.
To determine the test-retest reliability of the CROM measurements, the ICC mixed model 3,1 designated as 2 -way analysis of variance (ANOVA) for absolute agreement of single measure with 95% confidence interval (CI) was used.
The standard error of the measurement (SEM) was calculated using the following formula;
SEM=SD√1-rα. (r; reliability of the measure).34 The minimal detectable change at the 90% CI was calculated as MDC90 equals 1.65(z score for 90%CI)*SEM*√2.
Results
Based on the inclusion and exclusion criteria, 30 subjects, (14 male and 16 females) were included in the study. Descriptive statistics of the baseline values are described in Table 1.
| Table 1: Demographic and descriptive baseline values | |
| Parameter | Value (Mean ± SD) |
| Age(y) | 38.73 ± 5.66 |
| Gender (M:F) | 14:16 |
| VAS score | 2.83 ± 0.59 |
| FEV1/FVC (%) | 64.76 ± 2.19 |
| Height (cm) | 158.1 ± 6.33 |
| Weight (kg) | 64.85 ± 8.15 |
| BMI (kg/m2) | 25.84 ± 1.51 |
| VAS - visual analogue scale; FEV1/FVC - Forced expiratory volume in 1 min/ forced vital capacity; BMI -Body Mass Index | |
Table 2 shows the descriptive and intrarater reliability statistics for measurements of cervical active range of motion (CAROM) in patients with chronic neck pain and respiratory dysfunction in session 1 and session 2. The intraclass coefficient values for intrarater reliability were; flexion 0.94 (0.88-0.97), extension 0.97 (0.93-0.98), right lateral flexion 0.96 (0.92-0.98), left lateral flexion 0.96 (0.93-0.98) right rotation 0.94 (0.88-0.97) and left lateral rotation 0.95 (0.95-0.99). The standard error of measurement ranges from 1.5° to 2.9°. Standard error of measurements were; flexion 2.6° extension 1.5°, right lateral flexion 2.9°, left lateral flexion 2.9°, right rotation 2.5° and left rotation 2°.
Discussion
This study was conducted to assess the reliability of results by CROM device in patients simultaneously suffering from neck pain and respiratory dysfunction. According to the results it is clear that ICC values were greater than 0.90, which show that CROM device for calculation of CAROM in patients with neck pain and respiratory dysfunction has excellent reliability. The intraclass coefficient above 0.90 for all six ranges lies in excellent range according to ICC model interpretation.32
Wolan et al. assessed inter and intrarater reliability of CROM device on 95 healthy individuals between ages of 20-24 y, and the difference at two weeks in retesting. According to their findings highest intrarater and
| Table 2: Descriptive and intrarater reliability statistics for measurement of CAROM in patients
with chronic neck pain and respiratory dysfunction using CROM device |
||||||
| Movement | Session-1
(Mean ± SD) |
Session-2
(Mean ± SD) |
ICC | 95%CI for ICC | SEM | MDC
90%CI |
| Flexion | 43.63 ± 2.76 | 43.86 ± 2.63 | .94 | 0.88-0.97 | 2.6° | 6.1° |
| Extension | 52.56 ± 2.50 | 53.36 ± 2.48 | .97 | 0.93-0.98 | 1.5° | 3.5° |
| Right lateral flexion | 41.73 ± 2.11 | 42.23 ± 1.97 | .96 | 0.92-0.98 | 2.9° | 6.8° |
| Left lateral flexion | 42.06 ± 2.04 | 42.26 ± 1.98 | .96 | 0.93-0.98 | 2.9° | 6.8° |
| Right rotation | 42.26 ± 1.04 | 42.46 ± 1.10 | .94 | 0.88-0.97 | 2.5° | 5.8° |
| Left rotation | 42.56 ± 1.45 | 42.76 ± 1.40 | .95 | 0.95-0.99 | 2.0° | 4.7° |
| Abbreviations: AROM, active range of motion: SD, standard deviation; ICC, intraclass correlation coefficient, model 3,1; SEM, standard error of the measurement; MDC minimal detectable change at 90% confidence level | ||||||
interrater concordance was observed in the measure of extension. Result of the present study shows similar trend where ICC value for cervical extension (0.97) was the highest when compared to ICC values from the other five analyzed movements. However, healthy population with age (20-25 y) was included in their study. Our study was different than previous CROM reliability studies as it was conducted in patients who suffered from neck pain along with respiratory dysfunction and investigated the CAROM in all six possible ranges with strict protocols and clear methods.33
The results of this study are in coherence with another study on neck pain patients in which average ICCs for CROM device was greater than 0.80; whereas, ICCs values for universal goniometer and visual estimation were less than 0.80.34 The three tools (CROM device, universal goniometer and visual screening) were used in 3 data collection sessions and 60 subjects were tested in three groups having 20 subjects in each group. However, the methodology of this study is different in terms of measurement of six planes of CAROM instead of a single plane in the said study. In a study for reproducibility of cervical active and passive range measurements after sub-acute whiplash disorder CROM device was found to be a reliable tool with ICC range (0.82-0.99).35 In this study 39 and 19 subjects were tested for intra and inter-observer studies respectively, both active and passive cervical ranges were measured and CROM was proved to be a reliable device for symptomatic neck pain patients. Apart from reliability measurement calculation of SEM and MDC are additional merits of this study; however, only active cervical ranges were observed, whereas Williams et al. measured passive range of motion as well. In another study CROM device was found useful in repositioning head accuracy and reliable in measurement of cervical ranges in patients with cervical radiculopathy.36
According to a systematic review by Williams et al. in a number of studies reliabilities of CROM device has been proved. Fifty-six studies were reviewed and 12 different methods were evaluated. Most of the studies were conducted on healthy population or to measure a single particular range such as flexion-extension of neck or forward head posture. In another study, researchers evaluated the intrarater reliability of CROM device for measuring proprioception of cervical spine in healthy individuals and described it to be a reliable tool.37 Apart from the difference of neck pain population studied in this study it has an additional merit of measuring standard error of measurement and minimal detectable change, which was lacking in the study by Reddy et al. In another study CROM device showed high reliability in patients suffering from migraine but only 50 young females with average age 35 y were studied.38 Our study minimized the gender bias by including both genders.
Limitations
We measured only the intrarater reliability, in a small sample. Future researchers should explore this phenomenon with large population assessing both interrater and intrarater reliability. It is necessary to rule out more factors which may influence the objective outcome measures of cervical spine due to coexistence of respiratory dysfunction.
Conclusion
CROM device is a reliable tool for intrarater analysis in measuring cervical active range of motion in patients with chronic neck pain and respiratory dysfunction. This device seems to be reliable in measuring cervical active range of motion in all six directions.
Trial registration
Registered as Trial No. IRCT 20200226046623N1 https://www.irct.ir/trial/46240
Data availability
The numerical data generated in this study is available with the authors.
Disclaimer
This study is based on an ongoing trial conducted as a part of PhD study at University of Lahore.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared by the authors.
Author contribution
SA: Conception and design of the study, Data collection, Data interpretation, Drafting
HZ: Drafting
AA: Data interpretation, Drafting
AH: Statistical Analysis
All authors read the final draft and approved.
References
- Ghaderi F, Javanshir K, Jafarabadi MA, Moghadam AN, Arab AM. Chronic neck pain and muscle activation characteristics of the shoulder complex. J Bodyw Mov Ther. 2019;23(4):913-7.[PubMed] DOI: 1016/j.jbmt.2019.02.019
- Scarabottolo CC, Pinto R, Oliveira C, Zanuto E, Cardoso J, Christofaro D. Back and neck pain prevalence and their association with physical inactivity domains in adolescents. Eur Spine J. 2017;26(9):2274-80.[PubMed]
- Budianto P, Kirana DH, Hafizhan M, Putra SE, Mirawati DK, Prabaningtyas HR. The effect of duration gadget uses during COVID-19 pandemic on neck pain, neck disability, and sleep quality. International Journal of Public Health. 2022;11(2):581-8. [google scholar]
- Bertozzi L, Negrini S, Agosto D, Costi S, Guccione AA, Lucarelli P, et al. Posture and time spent using a smartphone are not correlated with neck pain and disability in young adults: a cross-sectional study. Journal of bodywork and movement therapies.2020;26(2):220-226.[PubMed] https://doi.org/10.1016/j.jbmt.2020.09.006
- Al-Hadidi F, Bsisu I, AlRyalat SA, Al-Zu’bi B, Bsisu R, Hamdan M, et al. Association between mobile phone use and neck pain in university students: A cross-sectional study using numeric rating scale for evaluation of neck pain. PloS one. 2019;14(5):217-231. [PubMed] DOI: 1371/journal.pone.0217231
- Kahlaee AH, Ghamkhar L, Arab AM. The association between neck pain and pulmonary function: a systematic review. Am J Phys Med Rehabil. 2017;96(3):203-10. [PubMed] DOI: 1097/PHM.0000000000000608
- Dimitriadis Z, Kapreli E, Strimpakos N, Oldham J. Respiratory dysfunction in patients with chronic neck pain: What is the current evidence? J Bodyw Mov Ther. 2016;20(4):704-14. https://pubmed.ncbi.nlm.nih.gov/27814848/
- Dimitriadis Z, Kapreli E, Strimpakos N, Oldham J. Pulmonary function of patients with chronic neck pain: a spirometry study. Respir Care. 2014;59(4):543-9. [PubMed] DOI: 4187/respcare.01828
- Kapreli E, Vourazanis E, Strimpakos N. Neck pain causes respiratory dysfunction. Med hypotheses. 2008;70(5):1009-13. [PubMed] DOI: 1016/j.mehy.2007.07.050
- Vidotto LS, Carvalho CRFd, Harvey A, Jones M. Dysfunctional breathing: what do we know? J Bras Pneumol. 2019;45(1)e 20170347. [PubMed] DOI: 1590/1806-3713/e20170347
- Cheon JH, Lim NN, Lee GS, Won KH, Lee SH, Kang EY, et al. Differences of Spinal Curvature, Thoracic Mobility, and Respiratory Strength Between Chronic Neck Pain Patients and People Without Cervical Pain. Ann Rehabil Med. 2020;44(1):58. [PubMed] DOI: 5535/arm.2020.44.1.58
- Kirthika SV, Sudhakar S, Padmanabhan K, Ramanatha n K. Impact of upper crossed syndrome on pulmonary function among the recreational male players: A preliminary report. Saudi J Sports Med. 2018;18(2):71. [google scholar] [Free full text]
- Nierat M-C, Demiri S, Dupuis-Lozeron E, Allali G, Morélot-Panzini C, Similowski T, et al. When breathing interferes with cognition: experimental inspiratory loading alters timed up-and-go test in normal humans. PLoS One. 2016;11(3):e0151625. [PubMed] DOI: 1371/journal.pone.0151625
- Yeater TD, Clark DJ, Hoyos L, Valdes-Hernandez PA, Peraza JA, Allen KD, et al. Chronic pain is associated with reduced sympathetic nervous system reactivity during simple and complex walking tasks: Potential cerebral mechanisms. Chronic Stress(Thousand Oaks). 2021;5:24705470211030273. [PubMed] DOI: 1177/24705470211030273
- O'leary S, Falla D, Elliott JM, Jull G. Muscle dysfunction in cervical spine pain: implications for assessment and management. J Orthop Sports Phys Ther. 2009;39(5):324-33. [PubMed] DOI: 2519/jospt.2009.2872
- Han J, Park S, Kim Y, Choi Y, Lyu H. Effects of forward head posture on forced vital capacity and respiratory muscles activity. J Phys Ther Sci. 2016;28(1):128-31. [PubMed] DOI: 1589/jpts.28.128
- Bonilla-Barba L, Florencio LL, Rodríguez-Jiménez J, Falla D, Fernández-de-Las-Peñas C, Ortega-Santiago R. Women with mechanical neck pain exhibit increased activation of their superficial neck extensors when performing the cranio-cervical flexion test. Musculoskelet Sci Pract. 2020;49:102222. [PubMed] DOI: 1016/j.msksp.2020.102222
- Dimitriadis Z, Kapreli E, Strimpakos N, Oldham J. Respiratory weakness in patients with chronic neck pain. Man Ther. 2013;18(3):248-53. [PubMed] DOI: 1016/j.math.2012.10.014
- Kim M-S, Cha Y-J, Choi J-D. Correlation between forward head posture, respiratory functions, and respiratory accessory muscles in young adults. J Back Musculoskelet Rehabil. 2017;30(4):711-5. [PubMed] DOI: 3233/BMR-140253
- Kaur P, Pattnaik M, Mohanty PP. Relationship of cervicothoracic curvature with muscle strength and endurance in subjects with neck pain. Indian Journal of Physiotherapy and Occupational Therapy. 2013;7(3):156. [Google Scholar]
- Dimitriadis Z, Kapreli E, Strimpakos N, Oldham J. Hypocapnia in patients with chronic neck pain: association with pain, muscle function, and psychologic states. Am J Phys Med Rehabil. 2013;92(9):746-54. [PubMed] DOI: 1097/PHM.0b013e31829e74f7
- Lemeunier N, Jeoun E, Suri M, Tuff T, Shearer H, Mior S, et al. Reliability and validity of clinical tests to assess posture, pain location, and cervical spine mobility in adults with neck pain and its associated disorders: Part 4. A systematic review from the cervical assessment and diagnosis research evaluation (CADRE) collaboration. Musculoskelet Sci Pract. 2018;38:128-47. [PubMed] DOI: 1016/j.msksp.2018.09.013
- Pan F, Arshad R, Zander T, Reitmaier S, Schroll A, Schmidt H. The effect of age and sex on the cervical range of motion–a systematic review and meta-analysis. J Biomech. 2018;75:13-27. [PubMed] DOI: 1016/j.jbiomech.2018.04.047
- Williams MA, McCarthy CJ, Chorti A, Cooke MW, Gates S. A systematic review of reliability and validity studies of methods for measuring active andPassive cervical range of motion. J Manipulative Physiol Ther. 2010;33(2):138-55. [PubMed] DOI: 1016/j.jmpt.2009.12.009
- Agarwal S, Allison GT, Singer KP. Validation of the spin-T goniometer, a cervical range of motion device. J Manipulative Physiol Ther. 2005;28(8):604-9. [PubMed] DOI: 1016/j.jmpt.2005.08.015
- Farooq MN, Bandpei MAM, Ali M, Khan GA. Reliability of the universal goniometer for assessing active cervical range of motion in asymptomatic healthy persons. Pak J Med Sci. 2016;32(2):457. [PubMed] PMCID:PMC4859044 DOI: 12669/pjms.322.8747
- Audette I, Dumas J-P, Côté JN, De Serres SJ. Validity and between-day reliability of the cervical range of motion (CROM) device. J Orthop Sports Phys Ther. 2010;40(5):318-23. [PubMed] DOI: 2519/jospt.2010.3180
- Inokuchi H, Tojima M, Mano H, Ishikawa Y, Ogata N, Haga N. Neck range of motion measurements using a new three-dimensional motion analysis system: validity and repeatability. Eur Spine J. 2015 Dec;24(12):2807-15. [PubMed] DOI: 1007/s00586-015-3913-2
- Fletcher JP, Bandy WD. Intrarater reliability of CROM measurement of cervical spine active range of motion in persons with and without neck pain. J Orthop Sports Phys Ther. 2008;38(10):640-5. [PubMed] DOI: 2519/jospt.2008.2680
- Florêncio LL, Pereira PA, Silva ER, Pegoretti KS, Gonçalves MC, Bevilaqua-Grossi D. Agreement and reliability of two non-invasive methods for assessing cervical range of motion among young adults. Rev Bras Fisioter. 2010;14(2):175-81. [PubMed]
- Stokes EK. Rehabilitation outcome measures: Churchill Livingstone. Edinburgh; 2011.
- Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiro Med. 2016;15(2):155-63. [PubMed] PMCID:PMC4913118 DOI: 1016/j.jcm.2016.02.012
- Gugliotti M, Tau J, Gallo K, Sagliocca N, Horan M, Sussman N, et al. Between-week reliability of the cervical range of motion (CROM) device for upper cervical rotation. J Man Manip Ther. 2021;29(3):176-180. [PubMed] DOI: 1080/10669817.2020.1805691
- Youdas JW, Carey JR, Garrett TR. Reliability of measurements of cervical spine range of motion—comparison of three methods. Phys Ther. 1991;71(2):98-104. [PubMed] DOI: 1093/ptj/71.2.98
- Williams MA, Williamson E, Gates S, Cooke MW. Reproducibility of the cervical range of motion (CROM) device for individuals with sub-acute whiplash associated disorders. Eur Spine J. 2012;21(5):872-8. [PubMed] PMCID:PMC3337911 DOI: 1007/s00586-011-2096-8
- Wibault J, Vaillant J, Vuillerme N, Dedering Å, Peolsson A. Using the cervical range of motion (CROM) device to assess head repositioning accuracy in individuals with cervical radiculopathy in comparison to neck-healthy individuals. Man Ther. 2013;18(5):403-9. [PubMed] DOI: 11016/j.math.2013.02.004
- Alahmari K, Reddy RS, Silvian P, Ahmad I, Nagaraj V, Mahtab M. Intra-and inter-rater reliability of neutral head position and target head position tests in patients with and without neck pain. Braz J Phys Ther. 2017;21(4):259-67. [PubMed] PMCID: PMC5537472 DOI: 1016/j.bjpt.2017.05.003
- Oliveira-Souza AIS, Carvalho GF, Florêncio LL, Fernández-de-Las-Peñas C, Dach F, Bevilaqua-Grossi D. Intrarater and Interrater Reliability of the Flexion Rotation Test and Cervical Range of Motion in People With Migraine. J Manipulative Physiol Ther. 2020 ;43(9):874-881[PubMed] DOI: 1016/j.jmpt.2019.11.005