Hussein Hassan Al-Qarni
MSc of Advanced Nursing, Teaching Assistant, Adult Health Nursing Department, King Khalid University, Abha, Saudi Arabia.
Correspondence: Hussein Hassan Al-Qarni; E-mail: hhgalqarni@gmail.com
Abstract
Background & objectives: Ventilator-associated pneumonia (VAP) is an intensive care acquired iatrogenic pulmonary infection that affects the pulmonary parenchyma of patients who are mechanically ventilated. Worldwide, incidence of VAP can increase the mortality rate and delay therapy progress in ventilated patients; therefore, it is necessary to identify the best practice for reducing incidence of VAP. Oral hygiene is one of the basic procedures for minimising respiratory infection and reducing VAP, with 2% chlorhexidine being an oral care solution that is used to protect and enhance the mouth environment. Also, it can be used to reduce the colonisation of organisms that lead to infection.
This paper aims to determine whether the usage of 2% chlorhexidine mouthwash is effective in reducing the incidence of VAP.
Methodology: This paper is a part of literature review regarding the effectiveness of 2% chlorohexidine mouthwash in prevention of VAP. The review was conducted over three months (September–December 2020). In this review, a systematic search through the MEDLINE and Cumulative Index of Nursing and Allied Health (CINAHL) databases was undertaken to determine if chlorhexidine reduces VAP incidence.
Results: The results showed that 2% chlorhexidine is effective in reducing the incidence of VAP by diminishing the colonisation of pathogens in the mouth cavity and in the airway.
Conclusion: The use of 2% chlorhexidine as a mouthwash agent demonstrates an appropriate effect in reducing pathogen colonisation and reducing VAP incidence. Therefore, health professionals should make oral health care (OHC) a priority in ICU patients to reduce mortality among ventilated patients and improve the performance of the health service.
Key words: Ventilation, mechanical; Adult patient; Ventilator; Oral care; Mouth rinse; Chlorhexidine; Ventilator associated pneumonia; VAP
Citation: Al-Qarni HH. Effectiveness of 2% chlorhexidine mouthwash in minimizing ventilator-associated pneumonia in ventilated patients: evidence-based practice. Anaesth. pain intensive care 2021;25(5):633-637
DOI: 10.35975/apic.v25i5.1631 Received: February 10, 2021, Reviewed: June 18, 2021, Accepted: August 23, 2021
Introduction
VAP is an intensive care acquired iatrogenic pulmonary infection that occurs in the pulmonary parenchyma of ventilated patients.1 VAP occurs within 48 hours of the patients being initiated with ventilator therapy, and is classified as the second infection that is acquired in an intensive care unit (ICU).2 It affects 10-30% of ventilated patients.3 According to the Centre for DiseaseControl and Prevention (CDC), the main reason for VAP is colonisation of bacteria in a dry mouth, which is a side effect of the ventilator process. The normal flora that are located in the mouth cavity can colonise and cause infection because of placement of the endotracheal tube.4 The incidence of VAP can increase mortality among ventilated patients and lead to their rapid deterioration.4 This worsening of the general health can increase the cost of treatment, and at the same time
.
lengthen the hospital stay and ventilation period and increase the overuse of antibiotics.5 Therefore, seeking the best practice to provide oral health care (OHC) and to reduce colonisation is of critical importance for today’s health practitioner.
To find the relationship between the use of 2% chlorhexidine as a mouthwash solution and the incidence of VAP, a clinical question was formulated to find the best evidence. The clinical question is: In adult ventilated patients, does mouthwash with 2% chlorhexidine solution reduce the incidence of ventilator associated pneumonia (VAP)?
The answer to this question can enhance the quality of mouthcare and shed light on the importance of OHC in reducing the incidence of VAP. If optimal OHC is achieved, VAP incidence will be reduced, the complications of VAP will be managed and the quality of care will be improved.
This research aims to help ICU nurses identify the best practice regarding the use of 2% chlorhexidine for prevention of VAP.
Methodology
In this review, the search strategy used to find the evidence is explained. Then, the evidence is synthesised to find the best results. Based on these results, the recommendations for nurses and researchers are developed.
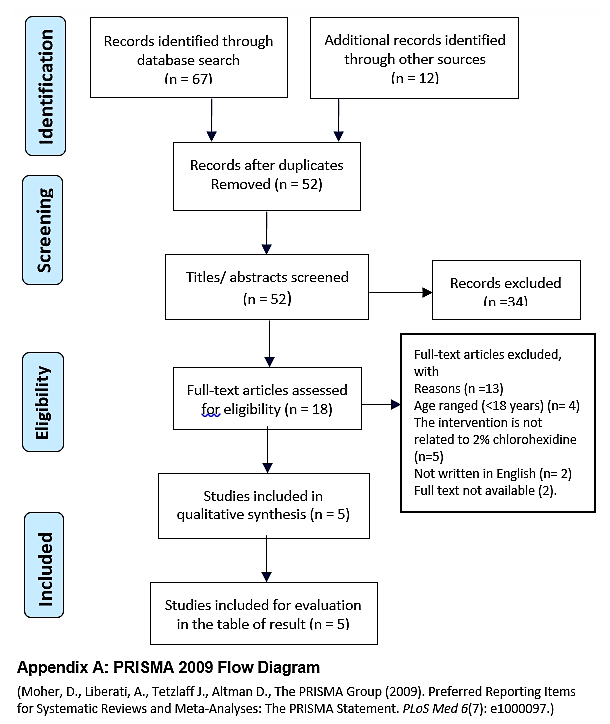
Search strategy In this project, the Cumulative Index of Nursing and Allied Health (CINAHL) and MEDLINE databases were utilised for the search using the components of the PICO question. These keywords, the MeSH terms, and CINAHL subject headings were utilised in the search (see Table I). The Boolean operators were utilised to join the terms within the same concepts with OR. However, the results of the search were joined with AND. To limit the search, articles in English published from 1970 to date were included because chlorhexidine began to be used in 1970.6 Also, only adult patients 18 y and older were involved in search. Additionally, to find all available evidence, all pyramid levels were searched. However, the search aimed to find studies that involved a randomised control trial (RCT), systematic review and/or meta-analysis to obtain the most valuable results. The reference lists of the articles found were also reviewed to find new sources that were not available in the databases. The PRISMA flow chart illustrates further the results of the database search (see Appendix A).
.
Evidence synthesis and interpretation
The best evidence to answer this clinical question is systematic reviews and RCT studies. These studies are the most relevant for finding the relationships between cause and effect and measuring the impacts of interventions on outcomes.7 According to the Joanna Briggs Institution,8 the systematic review of RCT and RCT studies are located on a high level of evidence. Systematic reviews are located on 1.a and RCTs are located on 1.c. These high levels of evidence can provide reliable and measurable results that can answer clinical questions.9 The inclusion criteria for this search were examining the effectiveness of chlorhexidine and adult patients at least 18 y old who were connected to a ventilator for more than 48 hours. In terms of the effect of chlorhexidine in minimising VAP incidence, two systematic reviews and three RCTs met the inclusion criteria, so they were reviewed to answer this research question (see Table). The total number of patients across all studies was 12,814.
Results
The results of these studies showed an effect on the incidence of VAP by using chlorhexidine compared with other OHC solutions. The incidence of VAP was reduced in the chlorhexidine group.
Incidence of VAP The two systematic reviews showed VAP incidence in the chlorhexidine group was lower than the control group. The systematic review by Kocaçal Güler and Türk (2019)10 stated that 2% chlorhexidine had an effect in reducing VAP. Two of the studies they reviewed found VAP to have late onset in the 2% chlorhexidine group, while two other studies showed there was a lower percentage of VAP incidence in the 2% chlorhexidine group. However, two studies reviewed found no differences between the 2% chlorhexidine group and the 0.9% NaCl group. Similarly, in 2013, Richard conducted a systematic review that proved the ability of chlorhexidine in reducing the incidence of VAP by 40% with a strong statistical significance (OR 0.60, 95% confidence intervals (CI) 0.47 to 0.77, P < 0.001).11
In the RCT studies, Koeman et al.’s (2006) RCT showed that the incidence of VAP was reduced in the chlorhexidine group by 35%. Similarly, in the RCT of Özçaka et al. (2012), the odds of contracting VAP were three times higher in the normal saline group than in the chlorhexidine group and they are at risk to develop VAP eight times than normal saline group (OR= 3.12, CI = 1,9 – 8,91, P= 0.03).12 However, one RCT showed that chlorhexidine is not effective in reducing VAP, with the incidence of VAP being higher in the chlorhexidine group (four patients developed VAP) compared with the 0.9% NaCl group (two patients).13 It is worth noting that in this RCT, the size of the sample was small and the average age of patients in the chlorhexidine group was in a different age range to the placebo group (mean age is 51.3 compared with placebo group 41). However, the result of this study was not statistically significant (RR=0.51, 95% CI 0.27-0.98; P=0.011).13 In all studies, all participants were randomly located, and the intervention was double blinded. Randomisation and blinding help to equally distribute the confounding factors between the control and intervention groups and hence improve the quality of the studies.9 These high-quality studies help researchers to find the relationships between effect and cause. 9
Confounding factors There are confounding factors in RCT studies such as ICU setting and antibiotic use. The trials were conducted in different countries and different ICU settings such as Brazil, 13 Turkey,12 and the Netherlands.14 Also, the settings included mixed ICU settings such as the RCT of Tuon et al.13 and Koeman et al., 14 or just a respiratory setting, such as the trial of Özçaka et al.12 Different ICU settings could affect the validity of the results because of the variety of health care services and patient conditions and co-morbidities. Use of antibiotics is another confounding factor that can affect the presence of pathogens; hence, the sample result will affect the statistical analysis of the studies.
All participants in all studies were adults patients who needed a ventilator for at least 48 hours, because VAP always develops after 48 hours.15 Regardless of the variation in geographic location of the studies, the results were consistent. All reviews and studies showed that chlorhexidine minimises the pathogen colonisation. Also, all studies, except Richard’s review, showed that the chlorhexidine group had a lower percentage of VAP incidence compared with the placebo group.
The results of the studies provided promising evidence. However, some studies should be interpreted with caution. First, there is a heterogeneous sample in systematic review studies. With more homogeneous sample, a meta-analysis can be conducted to enhance the result. Second, two of the RCTs had a small sample size,
.
which can affect the quality of the result. Third, none of the studies mentioned if there are side effects of using chlorhexidine. Finally, the frequency of using chlorhexidine varied between studies. Without a similar frequency of use, it is difficult to draw a conclusion about which frequency may provide more benefit from chlorhexidine.
The exemplary study Despite the old publication date of 2006 of the RCT of Koeman and his colleagues, this RCT is an exemplary study for identifying the relationship between chlorhexidine and VAP incidence. The PICO elements of this RCT are similar to this study’s clinical question. Also, the process of randomisation and blinding is applied well. Moreover, the size sample was large and provided sufficient evidence.
Recommendations
It is worth mentioning that VAP is known to be caused by different pathogens.4 Also, VAP occurs as a result of accumulation of pathogens in a dry mouth. The infection can occur within 48 hours after intubation. 15
The recommendations of this study for practitioners are that ICU nurses should apply 2% chlorhexidine as a mouthwash for ventilated adult patients. Also, they should keep ventilated patients’ mouths clean and clear from pathogens. OHC is the paramount goal for preventing VAP incidence. 15 Moreover, chlorhexidine is the best choice based on the results of this evidence. Moreover, ICU nurses should be aware of the signs and symptoms of VAP, the risk factors, complications, and the best infection control method to curb VAP among ventilated patients. This awareness can enhance the quality of care and reduce VAP incidence.
Other recommendations for researchers are that more research needs to be conducted in order to detect the most useful frequency and amount of mouthwash to use. There is currently no agreement in the evidence about the most useful frequency. Also, the side-effects of chlorhexidine need to be tested, especially in vulnerable patients such as pregnant women and elderly patients. More studies need to be conducted to detect the most pathogens that cause VAP and which mouthcare solution can target these pathogens.
Conclusion
The objective of this review was to assess previous studies that investigated the effectiveness of chlorohexidine in reducing VAP incidence. The results show that using chlorhexidine as a mouthwash provides a promising treatment. It can minimise the incidence of VAP and minimise the colonisation of the pathogens that can cause VAP or other respiratory infections. Hence, better quality of care, shorter duration of hospital stay, and shorter the ventilation period.
Finally, it is recommended that future studies look at measuring the most useful frequency, the safety, and which pathogens are related to VAP incidence.
Conflict of interests
None declared by the authors. The study did not involve funding from any source.
Authors’ contribution
HHA is the sole researcher and the author of this manuscript.
References
Correspondence: Hussein Hassan Al-Qarni; E-mail: hhgalqarni@gmail.com
Abstract
Background & objectives: Ventilator-associated pneumonia (VAP) is an intensive care acquired iatrogenic pulmonary infection that affects the pulmonary parenchyma of patients who are mechanically ventilated. Worldwide, incidence of VAP can increase the mortality rate and delay therapy progress in ventilated patients; therefore, it is necessary to identify the best practice for reducing incidence of VAP. Oral hygiene is one of the basic procedures for minimising respiratory infection and reducing VAP, with 2% chlorhexidine being an oral care solution that is used to protect and enhance the mouth environment. Also, it can be used to reduce the colonisation of organisms that lead to infection.
This paper aims to determine whether the usage of 2% chlorhexidine mouthwash is effective in reducing the incidence of VAP.
Methodology: This paper is a part of literature review regarding the effectiveness of 2% chlorohexidine mouthwash in prevention of VAP. The review was conducted over three months (September–December 2020). In this review, a systematic search through the MEDLINE and Cumulative Index of Nursing and Allied Health (CINAHL) databases was undertaken to determine if chlorhexidine reduces VAP incidence.
Results: The results showed that 2% chlorhexidine is effective in reducing the incidence of VAP by diminishing the colonisation of pathogens in the mouth cavity and in the airway.
Conclusion: The use of 2% chlorhexidine as a mouthwash agent demonstrates an appropriate effect in reducing pathogen colonisation and reducing VAP incidence. Therefore, health professionals should make oral health care (OHC) a priority in ICU patients to reduce mortality among ventilated patients and improve the performance of the health service.
Key words: Ventilation, mechanical; Adult patient; Ventilator; Oral care; Mouth rinse; Chlorhexidine; Ventilator associated pneumonia; VAP
Citation: Al-Qarni HH. Effectiveness of 2% chlorhexidine mouthwash in minimizing ventilator-associated pneumonia in ventilated patients: evidence-based practice. Anaesth. pain intensive care 2021;25(5):633-637
DOI: 10.35975/apic.v25i5.1631 Received: February 10, 2021, Reviewed: June 18, 2021, Accepted: August 23, 2021
Introduction
VAP is an intensive care acquired iatrogenic pulmonary infection that occurs in the pulmonary parenchyma of ventilated patients.1 VAP occurs within 48 hours of the patients being initiated with ventilator therapy, and is classified as the second infection that is acquired in an intensive care unit (ICU).2 It affects 10-30% of ventilated patients.3 According to the Centre for DiseaseControl and Prevention (CDC), the main reason for VAP is colonisation of bacteria in a dry mouth, which is a side effect of the ventilator process. The normal flora that are located in the mouth cavity can colonise and cause infection because of placement of the endotracheal tube.4 The incidence of VAP can increase mortality among ventilated patients and lead to their rapid deterioration.4 This worsening of the general health can increase the cost of treatment, and at the same time
| Table I: Key words and MESH terms used in search strategy | ||||
| Population | Intervention | Comparison | Outcome | |
| Key terms | Ventilated patients, adult adj2 patient, mechanical* ventilator* patient | ‘oral care’, ‘mouth rinse’, chlorhexidine |
Oral health care, Saline Solution |
ventilator associated pneumonia, VAP |
| MeSH | Respiration, Artificial | Oral Hygiene, chlorhexidine |
Oral Health, Chlorhexidine |
Pneumonia, Ventilator-Associated |
| CINAHL subject headings | Ventilator patients. | Oral Health, Chlorhexidine |
Pneumonia, Aspiration. | |
| Mesh: The Medical Subject Headings; CINAHL: Cumulative Index of Nursing and Allied Health | ||||
lengthen the hospital stay and ventilation period and increase the overuse of antibiotics.5 Therefore, seeking the best practice to provide oral health care (OHC) and to reduce colonisation is of critical importance for today’s health practitioner.
To find the relationship between the use of 2% chlorhexidine as a mouthwash solution and the incidence of VAP, a clinical question was formulated to find the best evidence. The clinical question is: In adult ventilated patients, does mouthwash with 2% chlorhexidine solution reduce the incidence of ventilator associated pneumonia (VAP)?
The answer to this question can enhance the quality of mouthcare and shed light on the importance of OHC in reducing the incidence of VAP. If optimal OHC is achieved, VAP incidence will be reduced, the complications of VAP will be managed and the quality of care will be improved.
This research aims to help ICU nurses identify the best practice regarding the use of 2% chlorhexidine for prevention of VAP.
Methodology
In this review, the search strategy used to find the evidence is explained. Then, the evidence is synthesised to find the best results. Based on these results, the recommendations for nurses and researchers are developed.
Search strategy In this project, the Cumulative Index of Nursing and Allied Health (CINAHL) and MEDLINE databases were utilised for the search using the components of the PICO question. These keywords, the MeSH terms, and CINAHL subject headings were utilised in the search (see Table I). The Boolean operators were utilised to join the terms within the same concepts with OR. However, the results of the search were joined with AND. To limit the search, articles in English published from 1970 to date were included because chlorhexidine began to be used in 1970.6 Also, only adult patients 18 y and older were involved in search. Additionally, to find all available evidence, all pyramid levels were searched. However, the search aimed to find studies that involved a randomised control trial (RCT), systematic review and/or meta-analysis to obtain the most valuable results. The reference lists of the articles found were also reviewed to find new sources that were not available in the databases. The PRISMA flow chart illustrates further the results of the database search (see Appendix A).
.
Evidence synthesis and interpretation
The best evidence to answer this clinical question is systematic reviews and RCT studies. These studies are the most relevant for finding the relationships between cause and effect and measuring the impacts of interventions on outcomes.7 According to the Joanna Briggs Institution,8 the systematic review of RCT and RCT studies are located on a high level of evidence. Systematic reviews are located on 1.a and RCTs are located on 1.c. These high levels of evidence can provide reliable and measurable results that can answer clinical questions.9 The inclusion criteria for this search were examining the effectiveness of chlorhexidine and adult patients at least 18 y old who were connected to a ventilator for more than 48 hours. In terms of the effect of chlorhexidine in minimising VAP incidence, two systematic reviews and three RCTs met the inclusion criteria, so they were reviewed to answer this research question (see Table). The total number of patients across all studies was 12,814.
Results
The results of these studies showed an effect on the incidence of VAP by using chlorhexidine compared with other OHC solutions. The incidence of VAP was reduced in the chlorhexidine group.
Incidence of VAP The two systematic reviews showed VAP incidence in the chlorhexidine group was lower than the control group. The systematic review by Kocaçal Güler and Türk (2019)10 stated that 2% chlorhexidine had an effect in reducing VAP. Two of the studies they reviewed found VAP to have late onset in the 2% chlorhexidine group, while two other studies showed there was a lower percentage of VAP incidence in the 2% chlorhexidine group. However, two studies reviewed found no differences between the 2% chlorhexidine group and the 0.9% NaCl group. Similarly, in 2013, Richard conducted a systematic review that proved the ability of chlorhexidine in reducing the incidence of VAP by 40% with a strong statistical significance (OR 0.60, 95% confidence intervals (CI) 0.47 to 0.77, P < 0.001).11
In the RCT studies, Koeman et al.’s (2006) RCT showed that the incidence of VAP was reduced in the chlorhexidine group by 35%. Similarly, in the RCT of Özçaka et al. (2012), the odds of contracting VAP were three times higher in the normal saline group than in the chlorhexidine group and they are at risk to develop VAP eight times than normal saline group (OR= 3.12, CI = 1,9 – 8,91, P= 0.03).12 However, one RCT showed that chlorhexidine is not effective in reducing VAP, with the incidence of VAP being higher in the chlorhexidine group (four patients developed VAP) compared with the 0.9% NaCl group (two patients).13 It is worth noting that in this RCT, the size of the sample was small and the average age of patients in the chlorhexidine group was in a different age range to the placebo group (mean age is 51.3 compared with placebo group 41). However, the result of this study was not statistically significant (RR=0.51, 95% CI 0.27-0.98; P=0.011).13 In all studies, all participants were randomly located, and the intervention was double blinded. Randomisation and blinding help to equally distribute the confounding factors between the control and intervention groups and hence improve the quality of the studies.9 These high-quality studies help researchers to find the relationships between effect and cause. 9
Confounding factors There are confounding factors in RCT studies such as ICU setting and antibiotic use. The trials were conducted in different countries and different ICU settings such as Brazil, 13 Turkey,12 and the Netherlands.14 Also, the settings included mixed ICU settings such as the RCT of Tuon et al.13 and Koeman et al., 14 or just a respiratory setting, such as the trial of Özçaka et al.12 Different ICU settings could affect the validity of the results because of the variety of health care services and patient conditions and co-morbidities. Use of antibiotics is another confounding factor that can affect the presence of pathogens; hence, the sample result will affect the statistical analysis of the studies.
All participants in all studies were adults patients who needed a ventilator for at least 48 hours, because VAP always develops after 48 hours.15 Regardless of the variation in geographic location of the studies, the results were consistent. All reviews and studies showed that chlorhexidine minimises the pathogen colonisation. Also, all studies, except Richard’s review, showed that the chlorhexidine group had a lower percentage of VAP incidence compared with the placebo group.
The results of the studies provided promising evidence. However, some studies should be interpreted with caution. First, there is a heterogeneous sample in systematic review studies. With more homogeneous sample, a meta-analysis can be conducted to enhance the result. Second, two of the RCTs had a small sample size,
| Table 2: Result table | ||||||
| Author (year) | Source of evidence | Study design | Level of evidence | Sample/ setting | Key findings or outcomes | Strength and limitation |
| Kocaçal Güler, & Türk (2019). | Synthesis | Sys Rev | 1. a | 12 RCTs include 917 adult ventilated patients. (Population of two studies were 15 y old, and in the rest of the studies, the population was 18 y old). |
§ This review aimed to compare which concentration of chlorhexidine is more effective in reducing VAP. Then the results were compared with other solutions (normal saline and herbal) to check which the most effective solution was. § 12 RCTs were reviewed. § Seven of the RCTs (out of 12) showed a positive impact of using chlorohexidine as being a mouthwash agent capable of minimising VAP incidence among ventilator patients. |
Strengths:
§ The comprehensive search. § The evaluation of the methodological quality of the studies included. Limitations: § Heterogeneity in population, intervention, and outcomes which prevents conduct meta-analysis. |
| Veitz-Keenan, & Ferraiolo (2017). | Synthesis | Sys Rev | 1. a | 38 RCTs include 6061 ventilated patients. | § This review aims to evaluate the using of chlorhexidine in oral care to reduce the incidence of VAP. § 38 RCTs were reviewed. § 18 RCTs showed evidence that chlorhexidine reduces VAP incidence from 25% to 19%. (RR 0.74, 95% confidence intervals (CI) 0.61 to 0.89, P = 0.002, heterogeneity I2 = 31%). Number needed to treat (NNT) = 17 (95% CI 10 to 33). § There are no differences in secondary outcomes between using chlorhexidine and other mouthwash agents. |
Strength
§ Eleven databases were searched. § 38 RCTs were reviewed. Limitations § Population in this review include all ventilated patients which can increase the risk of confounding factors. § Intervention includes several mouthwash agents |
| Richards (2013) | Synthesis | Sys Rev | 1. a | 35 RCTs include 5374 ventilated patients from different age groups. | § This review was conducted to evaluate the effectiveness of chlorhexidine in preventing VAP incidence. § 17 RCTs (out of 35) were reviewed. § The review proved that using chlorohexidine reduces the incidence of VAP in groups that used chlorhexidine compared with the placebo group (OR 0.60, 95% confidence intervals (CI) 0.47 to 0.77, P < 0.001, I2 = 21%) A number needed to treat (NNT) of 15 (95% CI 10 to 34). § The same RCTs did not provide evidence that using chlorohexidine can affect the mortality, duration of stay in ICU, or using antibiotics. |
Strengths
§ The search follows Cochrane methodology. Limitations § Population in this review includes all ventilated patients which can increase the risk of confounding factors. § - Intervention and comparison include several mouthwash agents. |
| Tuon, Gavrilko, de Almeida, Sumi, Alberto, Rocha, & Rosa (2017) | Primary original study | RCT | 1.c | 16 adult ventilated patients from mixed ICU setting in Brazil. | § This prospective RCT was conducted to measure the effectiveness of 2% chlorhexidine in minimizing bacterial infection and VAP incidence compared with 0.9% NaCl solution. § The primary outcome was four patients of chlorhexidine group developed VAP and two patients of placebo group developed VAP. § However, there was a low percentage of bacterial colonisation in the chlorhexidine group compared with placebo group (RR=0.51, 95% CI 0.27-0.98; P=0.011) |
Strength
§ The RCT was double blinded and well randomized. Limitation § Small size sample. |
| Özçaka et al. (2012) | Primary original study | RCT | 1.c | 61 adult ventilated patients from respiratory ICU in Turkey. | § This RCT was conducted to measure the effectiveness of chlorhexidine in preventing VAP incidence. § 61 patients were randomised to two groups. § Intervention group (n = 29) received the chlorhexidine, and another (n = 32) received normal saline. § The incidence of VAP among the intervention group was 41.4% (12 out of 29). § In the control group, the incidence was 68.6% (22 out of 32). § There were no significant differences between the two groups in the type of pathogens, the length of mechanical ventilation, the length of stay in ICU, and the mortality rate. |
Strength
§ The randomization of participants and blindness of intervention Limitations § Small sample size. § The trial was conducted in respiratory ICU which can be a confounding factor |
| Koeman et al. (2006) | Primary original study | RCT | 1.c | 385 Adult ventilated patients from mixed ICU in the Netherlands. | § This study aimed to compare the effectiveness of 2% chlorhexidine in minimizing VAP incidence with placebo agent. § 385 patients randomly located in three groups. § The risk of VAP incidence reduced to 65% (hazard ratio [HR]=0.352; 95% confidence interval [CI], 0.160, 0. 791; p=0.012) for CHX. § The chlorhexidine affects the colonisation of gram-positive microorganisms. § No differences between groups in duration of hospital stay and ventilation period. |
Strength
§ Large sample. § Randomized and blinded of study. Limitation § Compared three agents at the same time. |
which can affect the quality of the result. Third, none of the studies mentioned if there are side effects of using chlorhexidine. Finally, the frequency of using chlorhexidine varied between studies. Without a similar frequency of use, it is difficult to draw a conclusion about which frequency may provide more benefit from chlorhexidine.
The exemplary study Despite the old publication date of 2006 of the RCT of Koeman and his colleagues, this RCT is an exemplary study for identifying the relationship between chlorhexidine and VAP incidence. The PICO elements of this RCT are similar to this study’s clinical question. Also, the process of randomisation and blinding is applied well. Moreover, the size sample was large and provided sufficient evidence.
Recommendations
It is worth mentioning that VAP is known to be caused by different pathogens.4 Also, VAP occurs as a result of accumulation of pathogens in a dry mouth. The infection can occur within 48 hours after intubation. 15
The recommendations of this study for practitioners are that ICU nurses should apply 2% chlorhexidine as a mouthwash for ventilated adult patients. Also, they should keep ventilated patients’ mouths clean and clear from pathogens. OHC is the paramount goal for preventing VAP incidence. 15 Moreover, chlorhexidine is the best choice based on the results of this evidence. Moreover, ICU nurses should be aware of the signs and symptoms of VAP, the risk factors, complications, and the best infection control method to curb VAP among ventilated patients. This awareness can enhance the quality of care and reduce VAP incidence.
Other recommendations for researchers are that more research needs to be conducted in order to detect the most useful frequency and amount of mouthwash to use. There is currently no agreement in the evidence about the most useful frequency. Also, the side-effects of chlorhexidine need to be tested, especially in vulnerable patients such as pregnant women and elderly patients. More studies need to be conducted to detect the most pathogens that cause VAP and which mouthcare solution can target these pathogens.
Conclusion
The objective of this review was to assess previous studies that investigated the effectiveness of chlorohexidine in reducing VAP incidence. The results show that using chlorhexidine as a mouthwash provides a promising treatment. It can minimise the incidence of VAP and minimise the colonisation of the pathogens that can cause VAP or other respiratory infections. Hence, better quality of care, shorter duration of hospital stay, and shorter the ventilation period.
Finally, it is recommended that future studies look at measuring the most useful frequency, the safety, and which pathogens are related to VAP incidence.
Conflict of interests
None declared by the authors. The study did not involve funding from any source.
Authors’ contribution
HHA is the sole researcher and the author of this manuscript.
References
- Fernando SM, Tran A, Cheng W, Klompas M, Kyeremanteng K, Mehta S, et al. Diagnosis of ventilator-associated pneumonia in critically ill adult patients—a systematic review and meta-analysis. Intensive Care Med. 2020 Jun;46(6):1170-1179. [PubMed] DOI: 1007/s00134-020-06036-z
- Mahmoodpoor A, Sanaie S, Parthvi R, Shadvar K, Hamishekar H, Iranpour A, et al. A clinical trial of silver-coated and tapered cuff plus supraglottic suctioning endotracheal tubes in preventing ventilator-associated pneumonia. J Crit Care. 2020;56:171-6. [PubMed] DOI: 1016/j.jcrc.2019.12.024
- Batra P, Mathur P, John NV, Nair SA, Aggarwal R, Soni KD, et al. Impact of multifaceted preventive measures on ventilator-associated pneumonia at a single surgical centre. Intensive care Med. 2015;41(12):2231-2. [PubMed] DOI: 1007/s00134-015-4047-z
- Charles MP, Kali A, Easow JM, Joseph NM, Ravishankar M, Srinivasan S, et al. Ventilator-associated pneumonia. The Australas Med J. 2014;7(8):334. [PubMed] DOI: 4066/AMJ.2014.2105
- Younan D, Delozier SJ, Adamski J, Loudon A, Violette A, Ustin J, et al. Factors predictive of ventilator-associated pneumonia in critically ill trauma patients. World J Surg. 2020;44(4):1121-5. [PubMed] DOI: 1007/s00268-019-05286-3
- Löe H, Rindom Schiøtt C. The effect of mouthrinses and topical application of chlorhexidine on the development of dental plaque and gingivitis in man. J Periodontal Res. 1970;5(2):79-83. [PubMed] DOI: 1111/j.1600-0765.1970.tb00696.x
- Hariton E, Locascio JJ. Randomised controlled trials—the gold standard for effectiveness research. BJOG. 2018;125(13):1716. [PubMed] DOI: 1111/1471-0528.15199
- Aromataris E, Munn Z. Joanna Briggs Institute Reviewers’ Manual. Adelaide: Joanna Briggs Institute; 2017. DOI: 46658/JBIMES-20-04
- Melnyk BM, Fineout-Overholt E. Evidence-based practice in nursing & healthcare: A guide to best practice: Lippincott Williams & Wilkins; 2011.
- Kocaçal Güler E, Türk G. Oral chlorhexidine against ventilator-associated pneumonia and microbial colonization in intensive care patients. West J Nurs Res. 2019;41(6):901-19. [PubMed] DOI: 1177/0193945918781531
- Richards D. Oral hygiene regimes for mechanically ventilated patients that use chlorhexidine reduce ventilator-associated pneumonia. Evid Based Dent. 2013;14(3):91-2. [PubMed] DOI: 1038/sj.ebd.6400957
- Özçaka Ö, Başoğlu Ö, Buduneli N, Taşbakan M, Bacakoğlu F, Kinane D. Chlorhexidine decreases the risk of ventilator‐associated pneumonia in intensive care unit patients: a randomized clinical trial. J Periodontal Res. 2012;47(5):584-92. [PubMed] DOI: 1111/j.1600-0765.2012.01470.x
- Tuon FF, Gavrilko O, de Almeida S, Sumi ER, Alberto T, Rocha JL, et al. Prospective, randomised, controlled study evaluating early modification of oral microbiota following admission to the intensive care unit and oral hygiene with chlorhexidine. J Glob Antimicrob Resist. 2017;8:159-63. [PubMed] DOI: 10.1016/j.jgar.2016.12.007
- Koeman M, van der Ven AJ, Hak E, Joore HC, Kaasjager K, de Smet AG, et al. Oral decontamination with chlorhexidine treduces he incidence of ventilator-associated pneumonia. Am J Respir Crit Care Med. 2006;173(12):1348-55. [PubMed] DOI: 1164/rccm.200505-820OC
- Hua F, Xie H, Worthington HV, Furness S, Zhang Q, Li C. Oral hygiene care for critically ill patients to prevent ventilator‐associated pneumonia. Cochrane Database Syst Rev. 2016 Oct 25;10(10):CD008367. [PubMed] DOI: 1002/14651858.CD008367.pub3