Klein Dantis 1, Vimesh Rajput 2, Habib Md Reazaul Karim 3
Author affiliations:
Key words: Chest tubes; Drainage; COVID-19; Pneumothorax; Thoracic injuries
Citation: Dantis K, Rajput V, Karim HMR. Chest tube management in COVID-19 thoracic trauma care unit. Anaesth. pain intensive care 2021;25(4):550–551.
DOI: 10.35975/apic.v25i4.1578
.
Thoracic injury is one of the most common forms of trauma requiring admissions in more than 10% of the cases to an acute trauma care unit.1 Pneumothorax is the most common presentation after blunt or penetrating trauma, which requires chest tube insertion to prevent lung collapse. Spontaneous pneumothorax and barotrauma-related pneumothorax are well-known complications of COVID-19, who are being mechanically ventilated.2 Though pneumothorax is not a threatening condition at the initial stage, it can evolve as a potentially life-threatening condition. Chest tubes have a definite role in the management of pneumothorax in the acute care setting. In a pandemic, such management becomes even more challenging; and it depends upon the availability of the healthcare facilities. Although a concern regarding the surface transmission by the virus during the initial phase of the COVID-19 pandemic had been shown, but the latest research suggests the most common mode of transmission is through the aerosol route.3 Hence, in case of thoracic emergency intervention, patients should be assumed to be COVID-19 positive until proven otherwise, and a chest tube inserted, if indicated, under real-time thoracic ultrasonography by an experienced person. Various recommendations by different societies and authorities have been provided, which can be applied during the chest tube insertion procedure (Box 1)
Technical points to be considered:
The chest tube has to be clamped before insertion. In patients on mechanical ventilation, hold ventilation before piercing the parietal pleura. Following chest tube placement, the chest tube must be connected to the drainage system and then it needs to be unclamped to form a complete circuit. It prevents and avoids aerosol transmission.
Setting up a chest drainage system
The chest drainage systems can be of two types. The first is the simple chest drainage system, and the second is the valved dry seal chest drainage system.
A simple chest drainage system (Figure 1) can be used in any resource constraint setting. Here, the water seal drainage system is filled with a sterilizing solution, mainly betadine, rather than water alone to reduce the viral load. Bleach or sodium hypochlorite in the ratio of 1:50 of water can also be used.8 An antiviral filter needs to be attached to the vent of the water seal drainage system to avoid aerosol transmission. On the requirement of negative pressure, suction is connected to the antiviral filter's tubing's distal end.
A valved dry seal chest drainage system (Figure 1) is a single-valved system, which might play a significant role in the COVID-19 care unit. Scheffler valve and suction bulb evacuate fluid more rapidly than conventional drain. Sterilizing solution is not required as this system itself acts as a complete dry sealed closed system, reducing the viral load and preventing aerosol transmission. The vent of this system is attached to an antiviral filter to reduce further aerosol transmission. In severe trauma with significant blood loss, these can be used in autotransfusion.
Chest tube removal
It is necessary to hold ventilation on patients with mechanical ventilation. When not on a ventilator, it is better to remove at-end inspiration to avoid aerosol transmission. The closure of the site can be achieved by an occlusive dressing or tightening the preplaced suture at the closure site to prevent a gush of air into the atmosphere.
Follow up
It can be done with a portable X-ray device in the acute care unit with predetermined transport routes to prevent contamination.
References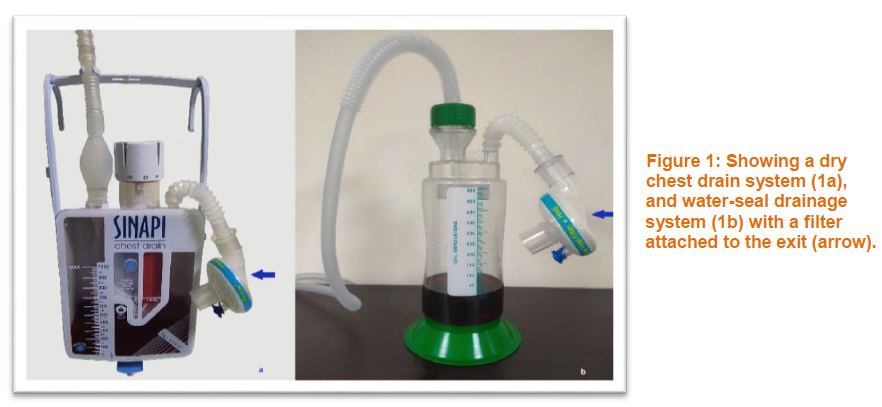
Author affiliations:
- Department of CTVS. All India Institute of Medical Sciences, Raipur. India. ORCID {0000-0003-2348-2797}
- Department of Thoracic Surgery. National Institute of Tuberculosis and Respiratory Disease, New Delhi. India. ORCID {0000-0001-99503-9941}
- Department of Anesthesiology, Critical Care and Pain Medicine. All India Institute of Medical Sciences, Raipur. India. ORCID {0000-0002-6632-0491}
Key words: Chest tubes; Drainage; COVID-19; Pneumothorax; Thoracic injuries
Citation: Dantis K, Rajput V, Karim HMR. Chest tube management in COVID-19 thoracic trauma care unit. Anaesth. pain intensive care 2021;25(4):550–551.
DOI: 10.35975/apic.v25i4.1578
| Box 1: Necessary recommendations that need to be followed during chest tube procedure:
· The procedure has to be performed in a negative pressure airborne infection isolation room (AIIR). In the absence of AIIR, a non-essential person should be restricted from entering the procedure room.4 · Full personal protective equipment- gowns, glasses, double gloves, N-95 surgical masks are highly recommended.5, 6 · Minimum transfer of the patients within the acute care setting is advised. · Diagnostic procedures that would not affect the decision have to be avoided. · Minimize the surgical equipment and personnel at the site of the intervention.7 · Ensure the presence of an antiviral filter.8 · The chest drainage system has to be prepared before the procedure. · For tension pneumothorax 12–14 F pigtail catheter is preferred. · In hemo- or hydropneumothorax, 24–28 Fr chest tube is used. · Doffing, as recommended by the Centers for Disease Control.5 |
Thoracic injury is one of the most common forms of trauma requiring admissions in more than 10% of the cases to an acute trauma care unit.1 Pneumothorax is the most common presentation after blunt or penetrating trauma, which requires chest tube insertion to prevent lung collapse. Spontaneous pneumothorax and barotrauma-related pneumothorax are well-known complications of COVID-19, who are being mechanically ventilated.2 Though pneumothorax is not a threatening condition at the initial stage, it can evolve as a potentially life-threatening condition. Chest tubes have a definite role in the management of pneumothorax in the acute care setting. In a pandemic, such management becomes even more challenging; and it depends upon the availability of the healthcare facilities. Although a concern regarding the surface transmission by the virus during the initial phase of the COVID-19 pandemic had been shown, but the latest research suggests the most common mode of transmission is through the aerosol route.3 Hence, in case of thoracic emergency intervention, patients should be assumed to be COVID-19 positive until proven otherwise, and a chest tube inserted, if indicated, under real-time thoracic ultrasonography by an experienced person. Various recommendations by different societies and authorities have been provided, which can be applied during the chest tube insertion procedure (Box 1)
Technical points to be considered:
The chest tube has to be clamped before insertion. In patients on mechanical ventilation, hold ventilation before piercing the parietal pleura. Following chest tube placement, the chest tube must be connected to the drainage system and then it needs to be unclamped to form a complete circuit. It prevents and avoids aerosol transmission.
Setting up a chest drainage system
The chest drainage systems can be of two types. The first is the simple chest drainage system, and the second is the valved dry seal chest drainage system.
A simple chest drainage system (Figure 1) can be used in any resource constraint setting. Here, the water seal drainage system is filled with a sterilizing solution, mainly betadine, rather than water alone to reduce the viral load. Bleach or sodium hypochlorite in the ratio of 1:50 of water can also be used.8 An antiviral filter needs to be attached to the vent of the water seal drainage system to avoid aerosol transmission. On the requirement of negative pressure, suction is connected to the antiviral filter's tubing's distal end.
A valved dry seal chest drainage system (Figure 1) is a single-valved system, which might play a significant role in the COVID-19 care unit. Scheffler valve and suction bulb evacuate fluid more rapidly than conventional drain. Sterilizing solution is not required as this system itself acts as a complete dry sealed closed system, reducing the viral load and preventing aerosol transmission. The vent of this system is attached to an antiviral filter to reduce further aerosol transmission. In severe trauma with significant blood loss, these can be used in autotransfusion.
Chest tube removal
It is necessary to hold ventilation on patients with mechanical ventilation. When not on a ventilator, it is better to remove at-end inspiration to avoid aerosol transmission. The closure of the site can be achieved by an occlusive dressing or tightening the preplaced suture at the closure site to prevent a gush of air into the atmosphere.
Follow up
It can be done with a portable X-ray device in the acute care unit with predetermined transport routes to prevent contamination.
References
- Dennis BM, Bellister SA, Guillamondegui OD. Thoracic Trauma. Surg Clin North Am. 2017 Oct;97(5):1047-1064. [PubMed] doi: 1016/j.suc.2017.06.009
- Martinelli AW, Ingle T, Newman J, Nadeem I, Jackson K, Lane ND, et al. COVID-19 and pneumothorax: a multicentre retrospective case series. Eur Respir J. 2020 Nov 19;56(5):2002697. [PubMed] DOI: 1183/13993003.02697-2020
- The Lancet Respiratory Medicine. COVID-19 transmission-up in the air. Lancet Respir Med. 2020 Dec;8(12):1159. [PubMed] DOI: 1016/S2213-2600(20)30514-2.
- van Doremalen N, Bushmaker T, Morris DH, Holbrook MG, Gamble A, Williamson BN, Taemin A, Harcourt JL, Thornburg NJ, Gerber SI, Lloyd-Smith JO, de Wit E, Munster VJ. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1. N Engl J Med. 2020 Apr 16;382(16):1564-1567. [PubMed] doi: 1056/NEJMc2004973
- Centers for Disease Control and Prevention. Interim Infection Prevention and Control Recommendations for Healthcare Personnel During the Coronavirus Disease 2019 (COVID-19) Pandemic. Last updated Feb 23, 2021 [Last accessed Mar 9, 2021]. Available from https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-recommendations.html
- Casanova LM, Rutala WA, Weber DJ, Sobsey MD. Effect of single- versus double-gloving on virus transfer to health care workers' skin and clothing during removal of personal protective equipment. Am J Infect Control. 2012 May;40(4):369-74. [PubMed] doi: 1016/j.ajic.2011.04.324
- Brindle ME, Gawande A. Managing COVID-19 in Surgical Systems. Ann Surg. 2020 Jul;272(1):e1-e2. [PubMed] doi: 1097/SLA.0000000000003923
- Pieracci FM, Burlew CC, Spain D, Livingston DH, Bulger EM, Davis KA, Michetti C. Tube thoracostomy during the COVID-19 pandemic: guidance and recommendations from the AAST Acute Care Surgery and Critical Care Committees. Trauma Surg Acute Care Open. 2020 Apr 30;5(1):e000498. [PubMed] doi: 1136/tsaco-2020-000498.