Priya Dixit1, Vinita Singh1, Sateesh Verma1, Gyan Prakash Singh1, Manish Kumar Singh1, Santosh Kumar2
Author affiliations:
Abstract
Background: Inflammation and postoperative pain plays an important role in the causation of postoperative cognitive dysfunction (POCD). Celecoxib – a COX–2 inhibitor, because of its anti–inflammatory and analgesic effects is used for the treatment of acute pain. In this study, we evaluated the effects of celecoxib on POCD and the postoperative pain in the elderly patients undergoing surgical reduction of fracture neck of femur under spinal anesthesia.
Methodology: We enrolled 84 patients of either sex, age more than 65 y, ASA grade I to III, who were planned for surgical reduction of fracture neck femur under spinal anesthesia. The patients were randomly divided into two groups and treated with either celecoxib (Group-A) or placebo (Group-B) for one week starting from one day before surgery. Mini–Mental State Examination (MMSE) was done at one day before the surgery and at day seven after surgery. POCD was diagnosed if MMSE score was below 24 (out of 30). Numerical rating scale (NRS) was used to measure pain intensity one day before surgery and at postoperative days one, three and seven. The results were analysed using descriptive statistics and making comparisons among various groups.
Results: MMSE at day 1 was 25.74 ± 1.45 vs. 26.45 ± 1.56 (p = 0.033) in Group-A and Group-B respectively. At postoperative day 7 it was 26.45 ± 1.56 vs. 23.64 ± 2.13 (p < 0.001) in Group-A and B respectively. NRS scores at postoperative day 1, 3 and 7 were 3.26 ± 1.43 vs. 3.62 ± 0.82 (p = 0.165), 3.38 ± 0.66 vs. 2.93 ± 0.68 (p = 0.003) and 1.19 ± 0.71 vs. 31 ± 0.72 (p = 0.445) in Group-A and Group-B respectively.
Conclusion: The results of our study conclude that celecoxib decreases the incidence of early postoperative cognitive dysfunction (POCD) in elderly patients undergoing surgical reduction of fracture neck of femur under spinal anesthesia. The administration of celecoxib also decreases intensity of the pain among patients in this surgical setting during recovery period especially on day 3.
Key words: Postoperative cognitive dysfunction; Celecoxib; NRS; Elderly patients; MMSE; Neuropsychological Tests; neuroinflammation
Abbreviations: POCD – Postoperative cognitive dysfunction; COX-2 – cyclooxygenase-2; MMSE – Mini Mental State Examination; BMI – Basal metabolic rate; NRS – Numerical Rating Scale
Citation: Dixit P, Singh V, Verma S, Singh GP, Singh MK, Kumar S. The effect of celecoxib on early postoperative cognitive dysfunction in elderly patients of fracture neck of femur: a prospective randomised double-blind study. Anaesth. pain intensive care 2021;25(3):287–294.
DOI: 10.35975/apic.v25i3.1519
Received: April 5, 2020; Reviewed: May 19, 2021; Revised: June 27, 2021; Accepted: June 27, 2020
Introduction
Postoperative cognitive dysfunction (POCD) is a relatively common phenomenon in elderly surgical patients, associated with increase in hospital stay, withdrawal from work.1,2 Inflammation is considered as the main cause for development of POCD.3,4 It has been reported that peripheral surgical trauma influences inflammatory processes in the brain.5–8 Russmussen et al. found that at 7th day the incidence of POCD was found to be 19.7%, [14.3–26.1%]) after general anesthesia and 12.5%, [8.0–18.3%]) after regional anesthesia (p = 0.06). After 3 months, POCD was 14.3%, [9.5–20.4%]) after general anesthesia vs. 13.9%, [9.0–20.2%]) after regional anesthesia (p = 0.93).9
There have been various studies regarding reduction of incidence of POCD using different drug like parecoxib, parecoxib with morphine, celecoxib, parecoxib sodium pre–treatment combined with dexmedetomidine and intraoperative infusion of dexmedetomidine.
It has been suggested in animal studies that surgery–induced neuro–inflammation is mediated by pro–inflammatory cytokines.6,7 presence of pro–inflammatory cytokines causes impairment in hippocampus–dependent cognitive memory.5 In multiple neuro–inflammation related neuro–degenerative diseases, such as multiple sclerosis, Alzheimer's disease, elevated COX–2 levels were found.10 This finding was proved effective in the treatment of surgery–mediated neuro–inflammation and cognitive impairment in animals.11,12
Celecoxib is a highly selective COX–2 inhibitor, because of its anti–inflammatory and analgesic effects, might potentially alleviate POCD. It has been used extensively for the treatment in various painful joint diseases and for the management of acute pain. Its role against the development of POCD in the clinical practice is still not clear.
Femur fracture is a common occurrence in the elderly population. Early pain management using regional anesthesia as a part of multimodal approach should be used in the perioperative period.13
The present study was aimed to study the efficacy of celecoxib on early postoperative cognitive dysfunction (POCD) and pain management in elderly patients with fracture neck femur to be managed surgically under spinal anesthesia.
Methodology
After obtaining institutional ethical committee approval and informed written from each patient this prospective randomised, double blinded study was conducted on 84 elderly patients. Patients of ASA physical status I, II and III, aged ≥ 65 y, undergoing surgery for fracture neck femur under spinal anesthesia were included. However, patients not willing to participate, BMI > 35, the Mini–Mental State Examination (MMSE) score < 23, peptic ulcer disease, cardiac–cerebral vascular disease, hepatic or chronic kidney diseases, neurological or psychiatric disorders, and allergic reactions to NSAIDs were excluded from study. Baseline MMSE score for cognition and Numerical Rating Scale (NRS) for pain was recorded. Study drugs were given in a sealed envelope to all patients, 1st dose 12hrs before surgery and thereafter 12 hourly for 7 days after surgery. We minimized the difference between the placebo and drug using same-colored capsules. Patients, doctors and investigators who were part of this study were blinded regarding assigning of groups. No sedative drugs were given to the patients. The patients were randomly allocated to one of the two groups using computer generated random number
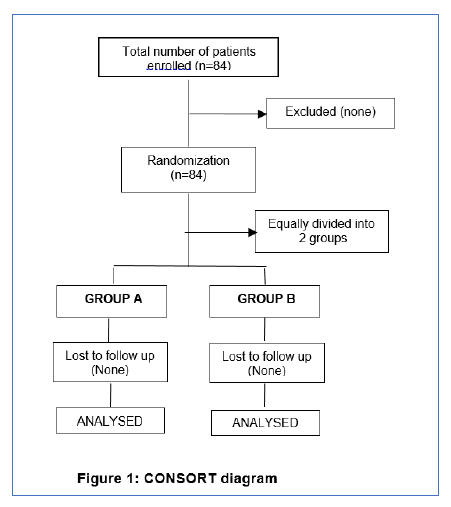
The patients were randomly allocated to one of the two groups using computer generated random number table:
All patients included in the study were operated under spinal anesthesia using bupivacaine 0.5% 3 ml (15 mg) with fentanyl 25 µg. Patients with failed spinals or converted to general anesthesia for any reason were excluded from the study.
Additional requirement of analgesia postoperatively in both the groups was managed with inj. tramadol (100 mg) I/M as and when required.
The cognitive function was assessed using Mini Mental State Examination (MMSE) one day before and at 1 week after surgery. This MMSE, a neuro–cognitive test measured registration (repeating named prompts), attention and calculation, recall, language ability to follow simple commands, orientation and visuospatial ability. MMSE is a simple but accurate with a sensitivity of 87% and specificity of 82% (Tombaugh and McIntyre14, Mallory et al.15). According to the definition a patient who’s postoperative MMSE declined less than 24/30 or decreased by less than 4 as compared to each preoperative MMSE score was classified to have POCD.16 NRS was used to assess pain one day before surgery at the time of preanesthetic check–up, and at day 1, 3 and day 7, postoperatively.
Statistical analysis: Sample size was calculated on the basis of 34% incidence in a previously published study.26 Thus at 95% confidence and 90% power, the calculated sample size was 74. After adding for a contingency @ 10% and rounding off to nearest 10 we got a sample size of 84 which was equally divided into two groups of 42 patients each. The results were analysed using descriptive statistics and making comparisons among various groups.
Results
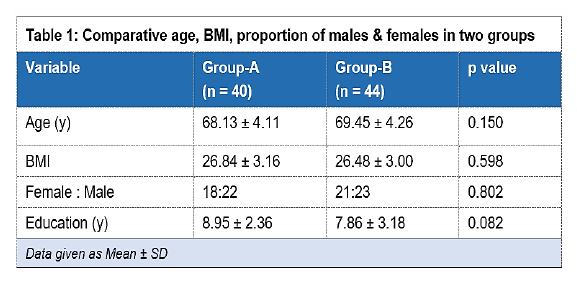
No significant difference was found in age (p = 0.156) and BMI of the two groups (p = 0.737). Proportion of males & females between the two groups (p = 0.827) were comparable. No significant difference was found in education level between the groups (p = 0.089) (Table 1).
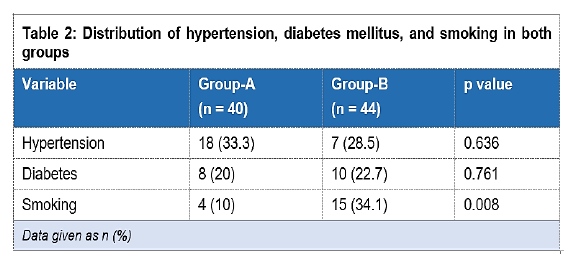
Both groups were similar with respect to distribution of hypertension and diabetes mellitus. Both group were comparable for drinking habits, however, statistically significant difference has been noted regarding smoking habit (Table 2).
Statistically significant difference was found in MMSE score between the groups. The intragroup comparison from pre–operative to POD 7 showed statistically significant changes in both groups though the changes in placebo groups were clinically significant in comparison to celecoxib group. Similarly, on POD 7, significant difference were found in the Attention and Calculation Score (2.98 ± 0.68 vs. 2.40 ± 0.77, p < 0.001), the Language Functioning Score (6.24 ± 0.58 vs. 5.76 ± 0.55, p = 0.007), Orientation Score (9.14 ± 0.68 vs. 8.40 ± 0.77, p < 0.001). However, no significant difference was found in the Immediate Memory Score (2.93 ± 0.26 vs. 2.83 ± 0.38, p = 0.182); the Recall Score (2.76 ± 0.43 vs. 2.86 ± 0.35, p = 0.399), the Visuo–spatial Score between the groups (0.67 ± 0.48 vs. 0.52 ± 0.51, p = 0.187) as shown in Table 3.
No significant difference was found in NRS at preoperative, on POD 1and POD 7 between the groups. However, statistically significant difference was found in NRS on POD 3 between the groups. Intragroup comparison between preoperative and POD 7 showed statistically significant difference (Table 4).
Discussion
Postoperative cognitive dysfunction is a recognized clinical phenomenon. As it was explained by Bedford as “Adverse cerebral effects of anesthesia on old people” in Lancet.17 Chung and Assmann18 very clearly showed its relevance in immediate postoperative period. Article describes two cases of
.
.
young patients who suffered of road traffic accidents due to postoperative cognitive impairment after undergoing ambulatory surgery. The cause of POCD is due to certain expression in the brain induced by pro inflammatory cytokine.12,19,20 Cytokine production can be induced by cyclooxygenase. These cytokines increase the permeability of blood brain barrier.
Celecoxib can easily cross the blood brain barrier; therefore, it can block COX–2 cytokines action in the central nervous system. Celecoxib also has anti–inflammatory effect through a COX–2–independent pathway which causes decrease in the infiltration of the inflammatory cells into the central nervous system and the expression of adhesion molecules.21 The specific mechanism of action of celecoxib made us to study the efficacy of celecoxib for the prevention of POCD. Celecoxib also decreases inflammation in central and peripheral tissues.
There are many factors which are related to incidence of POCD. Increasing Age, anesthesia time, low literacy, number of surgeries, postoperative infection, and respiratory complications were the probable risk factors for POCD.22,23,24 However, in our study, the differences between the two groups regarding these risk factors were minimal, their influence affecting the results were unlikely.
In most of the studies regarding POCD, mode of anesthesia was general anesthesia but in our study we have chosen regional anesthesia since it is more feasible in our centre as well as it is cost effective for the patients. Williams–Russo et al. also demonstrated there was no difference in the incidence of postoperative delirium between the general and epidural anesthesia groups at 1 week and 3 months, postoperatively.25
In our study, we assessed the effect of celecoxib on postoperative cognitive dysfunction (POCD) in elderly patients. Patients in both the groups were comparable regarding age, gender, BMI, and educational status. These results were consistent with various studies.26,27,28 Comorbidities were comparable in both the groups i.e., hypertension and diabetes mellitus. These results were consistent with the study by Zhu et al.26
As risk factors of POCD alcohol abuse, an anxious & depressed basal mood have been identified. In our study both the groups were comparable regarding alcohol abuse. The significant difference was found in proportion of smokers between the groups (p = 0.019). This result was in contrast with the study of Zhu et al.26 History of smoking seems to decrease the risk of POCD which is in accordance to our study.29
There are many methods for the clinical diagnosis of POCD, there is no general consensus. Because of many tools used, significant differences in the incidence of POCD are reported. Many studies use a decrease in performance in two or three items in battery of neuropsychiatric tests to diagnose POCD.25,30 In our study, we used the MMSE score; a widely used method for assessment of cognitive function. It is a simple but accurate test with a sensitivity of 87% and a specificity of 82%.14,15
In our study we found significant postoperative difference in total MMSE score at POD 7 in celecoxib group than control group. The incidence of POCD in celecoxib group was 14.28 % (6 out of 42); however, in placebo group it was 38% (16 out of 42). This incidence was found to be higher in our study as compared to the developed countries. It was 12 % in celecoxib group and 34 % in placebo group in a study done by Zhu et al. in China.26 This can be explained by low educational status of patients in developing countries admitted to government hospitals.
Similarly, on POD 7, significant difference was found in the Attention and Calculation Score, the Language Functioning Score, and the Orientation Score. However, no significant difference was found in the Immediate Memory Score, the Recall Score, the Visuo–spatial Score between the groups. There is no study regarding subsets of MMSE score till date; in our study we found that the Attention and Calculation Score and Orientation Score are affected the most, while the Recall Score is affected least, followed by the Immediate Memory Score and the Visuo–spatial Score.
Neuroinflammation is induced by pain, therefore postoperative pain might be critical in augmenting POCD & satisfactory analgesia may decrease the incidence of POCD following hip fracture in geriatric patients. In our study, at POD 1 the NRS of Group-A was 3.26 ± 1.43 while for the cases of group–B the NRS was 3.62 ± 0.82. No significant difference was found in NRS at this time between the groups (p = 0.165). At POD 3 the NRS of Group-A was 3.38 ± 0.66 while for the cases of group–B the NRS was 2.93 ± 0.68. The significant difference was found in NRS at this time between the groups (p = 0.003). On POD 7 the NRS of Group-A was 1.19 ± 0.71 while for the cases of group–B the NRS was 1.31 ± 0.72. No significant difference was found in NRS at this time between the groups (p=0.445). These findings indicated that the effective postoperative analgesia with celecoxib might have reduced the incidence of early POCD in geriatric patients.
Limitations
There were certain limitations of our study like it was a single centre small sample size study. Therefore, more multi–centre, large sample, randomized trials are recommended to confirm the findings. Follow–up period was relatively short; we didn’t include blood biomarker measurements in our study. The sample size in this study is small due to strict inclusion and exclusion criteria. One of the most important limitation was difficulties associated with implementing any neuro–cognitive tests due to low educational status of the patients.
Conclusion
In conclusion, our study showed that the administration of celecoxib in postoperative period in patients of fracture neck femur has protective effect in the development of postoperative cognitive dysfunction (POCD). The findings of our study also demonstrate that the administration of celecoxib decreases intensity of the pain among patients in this surgical setting during recovery period especially on day 3 i.e., in the middle of the recovery phase
Conflict of interest
None declared by the authors
Authors’ contribution
PD: Researcher
VS.: Guide
SV: Co–guide literature search
GS: Co–guide, statistical analysis
SK: Co–guide orthopedic team
MKS: Manuscript editing
References
Author affiliations:
- Department of Anesthesiology, King George Medical University (KGMU), Lucknow, UP, India 226001.
- Department of Orthopedics, King George Medical University (KGMU), Lucknow, UP, India 226001.
Abstract
Background: Inflammation and postoperative pain plays an important role in the causation of postoperative cognitive dysfunction (POCD). Celecoxib – a COX–2 inhibitor, because of its anti–inflammatory and analgesic effects is used for the treatment of acute pain. In this study, we evaluated the effects of celecoxib on POCD and the postoperative pain in the elderly patients undergoing surgical reduction of fracture neck of femur under spinal anesthesia.
Methodology: We enrolled 84 patients of either sex, age more than 65 y, ASA grade I to III, who were planned for surgical reduction of fracture neck femur under spinal anesthesia. The patients were randomly divided into two groups and treated with either celecoxib (Group-A) or placebo (Group-B) for one week starting from one day before surgery. Mini–Mental State Examination (MMSE) was done at one day before the surgery and at day seven after surgery. POCD was diagnosed if MMSE score was below 24 (out of 30). Numerical rating scale (NRS) was used to measure pain intensity one day before surgery and at postoperative days one, three and seven. The results were analysed using descriptive statistics and making comparisons among various groups.
Results: MMSE at day 1 was 25.74 ± 1.45 vs. 26.45 ± 1.56 (p = 0.033) in Group-A and Group-B respectively. At postoperative day 7 it was 26.45 ± 1.56 vs. 23.64 ± 2.13 (p < 0.001) in Group-A and B respectively. NRS scores at postoperative day 1, 3 and 7 were 3.26 ± 1.43 vs. 3.62 ± 0.82 (p = 0.165), 3.38 ± 0.66 vs. 2.93 ± 0.68 (p = 0.003) and 1.19 ± 0.71 vs. 31 ± 0.72 (p = 0.445) in Group-A and Group-B respectively.
Conclusion: The results of our study conclude that celecoxib decreases the incidence of early postoperative cognitive dysfunction (POCD) in elderly patients undergoing surgical reduction of fracture neck of femur under spinal anesthesia. The administration of celecoxib also decreases intensity of the pain among patients in this surgical setting during recovery period especially on day 3.
Key words: Postoperative cognitive dysfunction; Celecoxib; NRS; Elderly patients; MMSE; Neuropsychological Tests; neuroinflammation
Abbreviations: POCD – Postoperative cognitive dysfunction; COX-2 – cyclooxygenase-2; MMSE – Mini Mental State Examination; BMI – Basal metabolic rate; NRS – Numerical Rating Scale
Citation: Dixit P, Singh V, Verma S, Singh GP, Singh MK, Kumar S. The effect of celecoxib on early postoperative cognitive dysfunction in elderly patients of fracture neck of femur: a prospective randomised double-blind study. Anaesth. pain intensive care 2021;25(3):287–294.
DOI: 10.35975/apic.v25i3.1519
Received: April 5, 2020; Reviewed: May 19, 2021; Revised: June 27, 2021; Accepted: June 27, 2020
Introduction
Postoperative cognitive dysfunction (POCD) is a relatively common phenomenon in elderly surgical patients, associated with increase in hospital stay, withdrawal from work.1,2 Inflammation is considered as the main cause for development of POCD.3,4 It has been reported that peripheral surgical trauma influences inflammatory processes in the brain.5–8 Russmussen et al. found that at 7th day the incidence of POCD was found to be 19.7%, [14.3–26.1%]) after general anesthesia and 12.5%, [8.0–18.3%]) after regional anesthesia (p = 0.06). After 3 months, POCD was 14.3%, [9.5–20.4%]) after general anesthesia vs. 13.9%, [9.0–20.2%]) after regional anesthesia (p = 0.93).9
There have been various studies regarding reduction of incidence of POCD using different drug like parecoxib, parecoxib with morphine, celecoxib, parecoxib sodium pre–treatment combined with dexmedetomidine and intraoperative infusion of dexmedetomidine.
It has been suggested in animal studies that surgery–induced neuro–inflammation is mediated by pro–inflammatory cytokines.6,7 presence of pro–inflammatory cytokines causes impairment in hippocampus–dependent cognitive memory.5 In multiple neuro–inflammation related neuro–degenerative diseases, such as multiple sclerosis, Alzheimer's disease, elevated COX–2 levels were found.10 This finding was proved effective in the treatment of surgery–mediated neuro–inflammation and cognitive impairment in animals.11,12
Celecoxib is a highly selective COX–2 inhibitor, because of its anti–inflammatory and analgesic effects, might potentially alleviate POCD. It has been used extensively for the treatment in various painful joint diseases and for the management of acute pain. Its role against the development of POCD in the clinical practice is still not clear.
Femur fracture is a common occurrence in the elderly population. Early pain management using regional anesthesia as a part of multimodal approach should be used in the perioperative period.13
The present study was aimed to study the efficacy of celecoxib on early postoperative cognitive dysfunction (POCD) and pain management in elderly patients with fracture neck femur to be managed surgically under spinal anesthesia.
Methodology
After obtaining institutional ethical committee approval and informed written from each patient this prospective randomised, double blinded study was conducted on 84 elderly patients. Patients of ASA physical status I, II and III, aged ≥ 65 y, undergoing surgery for fracture neck femur under spinal anesthesia were included. However, patients not willing to participate, BMI > 35, the Mini–Mental State Examination (MMSE) score < 23, peptic ulcer disease, cardiac–cerebral vascular disease, hepatic or chronic kidney diseases, neurological or psychiatric disorders, and allergic reactions to NSAIDs were excluded from study. Baseline MMSE score for cognition and Numerical Rating Scale (NRS) for pain was recorded. Study drugs were given in a sealed envelope to all patients, 1st dose 12hrs before surgery and thereafter 12 hourly for 7 days after surgery. We minimized the difference between the placebo and drug using same-colored capsules. Patients, doctors and investigators who were part of this study were blinded regarding assigning of groups. No sedative drugs were given to the patients. The patients were randomly allocated to one of the two groups using computer generated random number
The patients were randomly allocated to one of the two groups using computer generated random number table:
- Group-A: Patients were given capsule containing celecoxib 200 mg.
- Group-B: Patients were given capsule containing placebo.
All patients included in the study were operated under spinal anesthesia using bupivacaine 0.5% 3 ml (15 mg) with fentanyl 25 µg. Patients with failed spinals or converted to general anesthesia for any reason were excluded from the study.
| Box 1: Mini Mental State Examination (MMSE) | |||
| One point for each answer Date | |||
| ORIENTATION
Year Season Month Date Time Country Town District Hospital Ward/Floor |
………/5 ………/5 |
………/5 ………/5 |
………/5 ………/5 |
| REGISTRATION
Examiner name three objects (e.g., apple, table, penny) and asks the patient to repeat (1 point for each correct. Then the patient learns the 3 names repeating until correct). |
………/3 |
………/3 |
………/3 |
| ATTENTION AND CALCULATION
Subtract 7 from 100, then repeat from result. Continue five times: 100, 93, 86, 79, 65. (Alternative: spell “World” backwards: DLROW). |
………/5 |
………/5 |
………/5 |
| RECALL
Ask for the names of the three objects learned earlier. |
………/3 |
………/3 |
………/3 |
| LANGUAGE
Name the objects (e.g., pen, watch) Repeat “No ifs, ands, or buts” Give a three–stage command, Score 1 for each stage. (e.g., ”place index finger of right hand on your nose and then on your left ear”) Ask the patient to read and obey a written command on a piece of paper. The written instruction is: “Close your eyes”. Ask the patient to write a sentence. Score 1 if it is sensible and has a subject and a verb. |
………/2 ………/1 ………/3 ………/1 ………/1 |
………/2 ………/1 ………/3 ………/1 ………/1 |
………/2 ………/1 ………/3 ………/1 ………/1 |
| Copying: Ask the patient to copy a pair of intersecting pentagons |
………/1 | ………/1 | ………/1 |
| Total score | ………/30 | ………/30 | ………/30 |
| MMSE scoring: 24–30: no cognitive impairment; 18–23: mild cognitive impairment; 0–17: severe cognitive impairment | |||
The cognitive function was assessed using Mini Mental State Examination (MMSE) one day before and at 1 week after surgery. This MMSE, a neuro–cognitive test measured registration (repeating named prompts), attention and calculation, recall, language ability to follow simple commands, orientation and visuospatial ability. MMSE is a simple but accurate with a sensitivity of 87% and specificity of 82% (Tombaugh and McIntyre14, Mallory et al.15). According to the definition a patient who’s postoperative MMSE declined less than 24/30 or decreased by less than 4 as compared to each preoperative MMSE score was classified to have POCD.16 NRS was used to assess pain one day before surgery at the time of preanesthetic check–up, and at day 1, 3 and day 7, postoperatively.
Statistical analysis: Sample size was calculated on the basis of 34% incidence in a previously published study.26 Thus at 95% confidence and 90% power, the calculated sample size was 74. After adding for a contingency @ 10% and rounding off to nearest 10 we got a sample size of 84 which was equally divided into two groups of 42 patients each. The results were analysed using descriptive statistics and making comparisons among various groups.
Results
No significant difference was found in age (p = 0.156) and BMI of the two groups (p = 0.737). Proportion of males & females between the two groups (p = 0.827) were comparable. No significant difference was found in education level between the groups (p = 0.089) (Table 1).
Both groups were similar with respect to distribution of hypertension and diabetes mellitus. Both group were comparable for drinking habits, however, statistically significant difference has been noted regarding smoking habit (Table 2).
Statistically significant difference was found in MMSE score between the groups. The intragroup comparison from pre–operative to POD 7 showed statistically significant changes in both groups though the changes in placebo groups were clinically significant in comparison to celecoxib group. Similarly, on POD 7, significant difference were found in the Attention and Calculation Score (2.98 ± 0.68 vs. 2.40 ± 0.77, p < 0.001), the Language Functioning Score (6.24 ± 0.58 vs. 5.76 ± 0.55, p = 0.007), Orientation Score (9.14 ± 0.68 vs. 8.40 ± 0.77, p < 0.001). However, no significant difference was found in the Immediate Memory Score (2.93 ± 0.26 vs. 2.83 ± 0.38, p = 0.182); the Recall Score (2.76 ± 0.43 vs. 2.86 ± 0.35, p = 0.399), the Visuo–spatial Score between the groups (0.67 ± 0.48 vs. 0.52 ± 0.51, p = 0.187) as shown in Table 3.
No significant difference was found in NRS at preoperative, on POD 1and POD 7 between the groups. However, statistically significant difference was found in NRS on POD 3 between the groups. Intragroup comparison between preoperative and POD 7 showed statistically significant difference (Table 4).
Discussion
Postoperative cognitive dysfunction is a recognized clinical phenomenon. As it was explained by Bedford as “Adverse cerebral effects of anesthesia on old people” in Lancet.17 Chung and Assmann18 very clearly showed its relevance in immediate postoperative period. Article describes two cases of
| Table 3: Comparative MMSE scores between the groups | ||||
| Variable | Group-A
(n = 40) |
Group-B
(n = 44) |
p value | |
| Orientation | Preop | 9.10 ± 0.67 | 9.38 ± 0.58 | 0.089 |
| POD 7 | 9.14 ± 0.56 | 8.40 ± 0.77 | < 0.001 | |
| Recall | Preop | 2.90 ± 0.30 | 2.86 ± 0.35 | 0.506 |
| POD 7 | 2.80 ± 0.42 | 2.36 ± 0.35 | 0.399 | |
| Immediate Memory | Preop | 3.00 ± 0.00 | 3.00 ± 0.00 | NA |
| POD 7 | 2.93 ± 0.26 | 2.83 ± 0.38 | 0.182 | |
| Language functioning | Preop | 5.88 ± 0.80 | 6.31 ± 0.95 | 0.028 |
| POD7 | 6.24 ± 0.58 | 5.76 ± 0.96 | 0.007 | |
| Attention and calculation | Preop | 3.60 ± 1.15 | 3.95 ± 0.62 | 0.080 |
| POD 7 | 2.98 ± 0.68 | 2.39 ± 0.77 | 0.001 | |
| Visio–spatial | Preop | 0.74 ± 0.45 | 0.83 ± 0.38 | 0.293 |
| POD 7 | 0.67 ± 0.48 | 0.52 ± 0.51 | 0.187 | |
| MMSE | Preop | 25.74 ± 1.38 | 26.45 ± 1.56 | 0.033 |
| POD 7 | 24.88 ± 1.29 | 23.64 ± 2.13 | < 0.001 | |
| Data given as Mean ± SD | ||||
| Table 4: NRS at preoperative, on POD 1, POD3 and POD 7 between the groups | ||||
| NRS | Group-A
(n = 40) |
Group-B
(n = 44) |
t–value | p value |
| Before Surgery | 2.14 ± 0.84 | 2.02 ± 0.52 | 0.78 | 0.438 |
| Day 1 | 3.26 ± 1.43 | 3.62 ± 0.82 | –1.40 | 0.165 |
| Day 3 | 3.38 ± 0.66 | 2.93 ± 0.68 | 3.10 | 0.003 |
| Day 7 | 1.19 ± 0.71 | 1.31 ± 0.72 | 0.77 | 0.445 |
| t–value, p–value | t = 6.105, p < 0.001 | t = 5.194, p < 0.001 | ||
| Data given as Mean ± SD | ||||
young patients who suffered of road traffic accidents due to postoperative cognitive impairment after undergoing ambulatory surgery. The cause of POCD is due to certain expression in the brain induced by pro inflammatory cytokine.12,19,20 Cytokine production can be induced by cyclooxygenase. These cytokines increase the permeability of blood brain barrier.
Celecoxib can easily cross the blood brain barrier; therefore, it can block COX–2 cytokines action in the central nervous system. Celecoxib also has anti–inflammatory effect through a COX–2–independent pathway which causes decrease in the infiltration of the inflammatory cells into the central nervous system and the expression of adhesion molecules.21 The specific mechanism of action of celecoxib made us to study the efficacy of celecoxib for the prevention of POCD. Celecoxib also decreases inflammation in central and peripheral tissues.
There are many factors which are related to incidence of POCD. Increasing Age, anesthesia time, low literacy, number of surgeries, postoperative infection, and respiratory complications were the probable risk factors for POCD.22,23,24 However, in our study, the differences between the two groups regarding these risk factors were minimal, their influence affecting the results were unlikely.
In most of the studies regarding POCD, mode of anesthesia was general anesthesia but in our study we have chosen regional anesthesia since it is more feasible in our centre as well as it is cost effective for the patients. Williams–Russo et al. also demonstrated there was no difference in the incidence of postoperative delirium between the general and epidural anesthesia groups at 1 week and 3 months, postoperatively.25
In our study, we assessed the effect of celecoxib on postoperative cognitive dysfunction (POCD) in elderly patients. Patients in both the groups were comparable regarding age, gender, BMI, and educational status. These results were consistent with various studies.26,27,28 Comorbidities were comparable in both the groups i.e., hypertension and diabetes mellitus. These results were consistent with the study by Zhu et al.26
As risk factors of POCD alcohol abuse, an anxious & depressed basal mood have been identified. In our study both the groups were comparable regarding alcohol abuse. The significant difference was found in proportion of smokers between the groups (p = 0.019). This result was in contrast with the study of Zhu et al.26 History of smoking seems to decrease the risk of POCD which is in accordance to our study.29
There are many methods for the clinical diagnosis of POCD, there is no general consensus. Because of many tools used, significant differences in the incidence of POCD are reported. Many studies use a decrease in performance in two or three items in battery of neuropsychiatric tests to diagnose POCD.25,30 In our study, we used the MMSE score; a widely used method for assessment of cognitive function. It is a simple but accurate test with a sensitivity of 87% and a specificity of 82%.14,15
In our study we found significant postoperative difference in total MMSE score at POD 7 in celecoxib group than control group. The incidence of POCD in celecoxib group was 14.28 % (6 out of 42); however, in placebo group it was 38% (16 out of 42). This incidence was found to be higher in our study as compared to the developed countries. It was 12 % in celecoxib group and 34 % in placebo group in a study done by Zhu et al. in China.26 This can be explained by low educational status of patients in developing countries admitted to government hospitals.
Similarly, on POD 7, significant difference was found in the Attention and Calculation Score, the Language Functioning Score, and the Orientation Score. However, no significant difference was found in the Immediate Memory Score, the Recall Score, the Visuo–spatial Score between the groups. There is no study regarding subsets of MMSE score till date; in our study we found that the Attention and Calculation Score and Orientation Score are affected the most, while the Recall Score is affected least, followed by the Immediate Memory Score and the Visuo–spatial Score.
Neuroinflammation is induced by pain, therefore postoperative pain might be critical in augmenting POCD & satisfactory analgesia may decrease the incidence of POCD following hip fracture in geriatric patients. In our study, at POD 1 the NRS of Group-A was 3.26 ± 1.43 while for the cases of group–B the NRS was 3.62 ± 0.82. No significant difference was found in NRS at this time between the groups (p = 0.165). At POD 3 the NRS of Group-A was 3.38 ± 0.66 while for the cases of group–B the NRS was 2.93 ± 0.68. The significant difference was found in NRS at this time between the groups (p = 0.003). On POD 7 the NRS of Group-A was 1.19 ± 0.71 while for the cases of group–B the NRS was 1.31 ± 0.72. No significant difference was found in NRS at this time between the groups (p=0.445). These findings indicated that the effective postoperative analgesia with celecoxib might have reduced the incidence of early POCD in geriatric patients.
Limitations
There were certain limitations of our study like it was a single centre small sample size study. Therefore, more multi–centre, large sample, randomized trials are recommended to confirm the findings. Follow–up period was relatively short; we didn’t include blood biomarker measurements in our study. The sample size in this study is small due to strict inclusion and exclusion criteria. One of the most important limitation was difficulties associated with implementing any neuro–cognitive tests due to low educational status of the patients.
Conclusion
In conclusion, our study showed that the administration of celecoxib in postoperative period in patients of fracture neck femur has protective effect in the development of postoperative cognitive dysfunction (POCD). The findings of our study also demonstrate that the administration of celecoxib decreases intensity of the pain among patients in this surgical setting during recovery period especially on day 3 i.e., in the middle of the recovery phase
Conflict of interest
None declared by the authors
Authors’ contribution
PD: Researcher
VS.: Guide
SV: Co–guide literature search
GS: Co–guide, statistical analysis
SK: Co–guide orthopedic team
MKS: Manuscript editing
References
- Rundshagen I. Postoperative cognitive dysfunction. Dtsch Arztebl Int. 2014 Feb;111(8):119–25. [PubMed] DOI: 3238/arztebl.2014.0119
- Terrando N, Eriksson LI, Ryu JK, Yang T, Monaco C, Feldmann M, et al. Resolving postoperative neuroinflammation and cognitive decline. Ann Neurol. 2011 Dec;70(6):986–95. [PubMed] DOI: 1002/ana.22664
- Li Y, Pan K, Chen L, Ning JL, Li X, Yang T, et al. Deferoxamine regulates neuroinflammation and iron homeostasis in a mouse model of postoperative cognitive dysfunction. J Neuroinflammation. 2016 Dec;13(1):268. [PubMed] DOI: 1186/s12974-016-0740-2
- Zhang X, Dong H, Li N, Zhang S, Sun J, Zhang S, et al. Activated brain mast cells contribute to postoperative cognitive dysfunction by evoking microglia activation and neuronal apoptosis. J Neuroinflammation. 2016;13:127. [PubMed] DOI: 1186/s12974-016-0592-9
- .Rosczyk HA, Sparkman NL, Johnson RW. Neuroinflammation and cognitive function in aged mice following minor surgery. Exp Gerontol. 2008 Sep 1;43(9):840-6. [PubMed] DOI: 1016/j.exger.2008.06.004
- Terrando N, Monaco C, Ma D, Foxwell BM, Feldmann M, Maze M. Tumor necrosis factor–α triggers a cytokine cascade yielding postoperative cognitive decline. Proc Natl Acad Sci U S A. 2010 Nov 23;107(47):20518–22. [PubMed] DOI: 1073/pnas.1014557107
- Cibelli M, Fidalgo AR, Terrando N, Ma D, Monaco C, Feldmann M, et al. Role of interleukin‐1β in postoperative cognitive dysfunction. Ann Neurol. 2010 Sep;68(3):360–8. [PubMed] DOI: 1002/ana.22082
- Hirsch J, Vacas S, Terrando N, Yuan M, Sands LP, Kramer J, et al. Perioperative cerebrospinal fluid and plasma inflammatory markers after orthopedic surgery. J Neuroinflammation. 2016 Dec;13(1):211. [PubMed] DOI: 1186/s12974-016-0681-9
- Rasmussen LS, Johnson T, Kuipers HM, Kristensen D, Siersma VD, Vila P, et al. Does anaesthesia cause postoperative cognitive dysfunction? A randomised study of regional versus general anaesthesia in 438 elderly patients. Acta Anaesthesiol Scand. 2003 Mar;47(3):260–6. [PubMed] DOI: 1034/j.1399-6576.2003.00057.x
- Luo D, Long Y, Chen GJ. Cyclooxygenase–2 gene polymorphisms and risk of Alzheimer's disease: A meta–analysis. J Neurol Sci. 2015 Dec 15;359(1–2):100–5. [PubMed] DOI: 1016/j.jns.2015.10.053
- Kamer AR, Galoyan SM, Haile M, Kline R, Boutajangout A, Li YS, et al. Meloxicam improves object recognition memory and modulates glial activation after splenectomy in mice. Eur J Anaesthesiol. 2012 Jul 1;29(7):332–7. [PubMed] DOI: 1097/EJA.0b013e3283534f56
- Peng M, Wang YL, Wang FF, Chen C, Wang CY. The cyclooxygenase–2 inhibitor celecoxib inhibits surgery–induced proinflammatory cytokine expression in the hippocampus in aged rats. J Surg Res. 2012;178:e1–8. [PubMed] DOI: 1016/j.jss.2012.08.030
- Moon A, Gray A, Deehan D. Neck of femur fractures in patient’s aged more than 85 years—are they a unique subset? Geriatr Orthop Surgery Rehabil. 2011 Jul;2(4):123–7. [PubMed] DOI: 1177/2151458511414562
- Tombaugh TN, McIntyre NJ. The mini‐mental state examination: a comprehensive review. J Am Geriatr Soc. 1992 Sep;40(9):922–35. [PubMed] DOI: 1111/j.1532-5415.1992.tb01992.x
- Mallory P, Cummings J, Coffey C, Duffy J, Fink M, Lauterbach E. Cognitive screening instruments in neuropsychiatry: a report of the Committee on Research of the American Neuropsychiatric Association. J Neuropsychiatry Clin Neurosci. 1997;9(2):189–97. [PubMed] DOI: 1176/jnp.9.2.189
- Boos GL, Soares LF, Oliveira Filho GR. Postoperative cognitive dysfunction: prevalence and associated factors. Rev Bras Anestesiol. 2005 Oct;55(5):517–24. [PubMed] DOI: 1590/s0034-70942005000500006
- Bedford PD. Adverse cerebral effects of anaesthesia on old people. Lancet. 1955 Aug 6;266(6884):259–63. [PubMed] DOI: 1016/s0140-6736(55)92689-1
- Chung F, Assmann N. Car accidents after ambulatory surgery in patients without an escort. Anesth Analg. 2008 Mar 1;106(3):817–20. [PubMed] DOI: 1213/ane.0b013e3181609531
- Hovens IB, Schoemaker RG, van der Zee EA, Heineman E, Izaks GJ, van Leeuwen BL. Thinking through postoperative cognitive dysfunction: how to bridge the gap between clinical and pre–clinical perspectives. Brain Behav Immun. 2012 Oct 1;26(7):1169–79. [PubMed] DOI: 1016/j.bbi.2012.06.004
- Van Harten AE, Scheeren TW, Absalom AR. A review of postoperative cognitive dysfunction and neuroinflammation associated with cardiac surgery and anaesthesia. Anaesthesia. 2012 Mar;67(3):280–93. [PubMed] DOI: 1111/j.1365-2044.2011.07008.x
- Miyamoto K, Miyake S, Mizuno M, Oka N, Kusunoki S, Yamamura T. Selective COX–2 inhibitor celecoxib prevents experimental autoimmune encephalomyelitis through COX–2–independent pathway. Brain. 2006 Jul 10;129(8):1984–92. [PubMed] DOI: 1093/brain/awl170
- Casati A, Aldegheri G, Vinciguerra F, Marsan A, Fraschini G, Torri G. Randomized comparison between sevoflurane anaesthesia and unilateral spinal anaesthesia in elderly patients undergoing orthopaedic surgery. Eur J Anaesthesiol. 2003 Sep;20(8):640–6. [PubMed] DOI: 1017/s0265021503001030
- Rasmussen LS, Johnson T, Kuipers HM, Kristensen D, Siersma VD, Vila P, et al. Does anaesthesia cause postoperative cognitive dysfunction? A randomised study of regional versus general anaesthesia in 438 elderly patients. Acta Anaesthesiol Scand. 2003 Mar;47(3):260–6. [PubMed] DOI: 1034/j.1399-6576.2003.00057.x
- Moller JT, Cluitmans P, Rasmussen LS, Houx P, Rasmussen H, Canet J, et al. Long–term postoperative cognitive dysfunction in the elderly: ISPOCD1 study. Lancet. 1998 Mar 21;351(9106):857–61. [PubMed] DOI: 1016/s0140-6736(97)07382-0
- Williams–Russo P, Sharrock NE, Mattis S, Szatrowski TP, Charlson ME. Cognitive effects after epidural vs. general anesthesia in older adults: a randomized trial. JAMA. 1995 Jul 5;274(1):44–50. [PubMed]
- Zhu Y, Yao R, Li Y, Wu C, Heng L, Zhou M, et al. Protective effect of celecoxib on early postoperative cognitive dysfunction in geriatric patients. Front Neurol. 2018 Aug;9:633. [PubMed] DOI: 3389/fneur.2018.00633
- Mu DL, Zhang DZ, Wang DX, Wang G, Li CJ, Meng ZT, et al. Parecoxib supplementation to morphine analgesia decreases incidence of delirium in elderly patients after hip or knee replacement surgery: a randomized controlled trial. Anesth Analg. 2017 Jun 1;124(6):1992–2000. [PubMed] DOI: 1213/ANE.0000000000002095
- Huang S, Hu H, Cai YH, Hua F. Effect of parecoxib in the treatment of postoperative cognitive dysfunction: A systematic review and meta–analysis. Medicine (Baltimore). 2019 Jan;98(1):e13812. [PubMed] DOI: 1097/MD.0000000000013812
- Wang R, Wang G, Liu Y, Zhang M. Preoperative smoking history is associated with decreased risk of early postoperative cognitive dysfunction in patients of advanced age after noncardiac surgery: a prospective observational cohort study. J Int Med Res. 2019 Feb;47(2):689–701. [PubMed] DOI: 1177/0300060518808162
- Hanning CD. Postoperative cognitive dysfunction. Br J Anaesth. 2005 Jan 7;95(1):82–7. [PubMed] DOI: 1093/bja/aei062