Chaitanya Pratyusha1, Sapna Nikhar2, Ch Rama Krishna Prasad1, R. Gopinath3
1Junior Resident; 2Assistant Professor; 3Professor
Department of Anaesthesiology and Intensive Care, Nizam’s Institute of Medical Sciences, Hyderabad, 500082, India. Email: - chaitanyapa9@gmail.com
Correspondence: Dr. Sapna Annaji Nikhar, Assistant Professor, Department of Anaesthesiology & Intensive Care, Nizam’s Institute of Medical Sciences, Hyderabad, 500082, (India); Telephone: +91 9030460262; E-mail: sapnanikhar@gmail.com,
ABSTRACT:
The use of anticoagulants to prevent thromboembolic complications post mechanical valve replacement is associated with intracranial or subdural hemorrhage. In such cases, the scale has to be balanced to have a good anticoagulation in order to prevent thromboembolism and to have a target INR (International normalized ration) in order to avoid hemorrhages specifically intracranial hemorrhages. A controversy exists on reversal of anticoagulation for emergency surgery and management may differ from case to case. Here, we report a case with massive subdural hematoma on warfarin post mechanical mitral valve replacement for emergency craniotomy and evacuation. Effective optimization and correction of INR by reversing anticoagulation lead to an improved outcome without further increase in thromboembolic complications.
Key words: Anticoagulants; Emergency surgery; Reversal
INTRODUCTION:
Long term anticoagulation is needed to avoid thromboembolic complications due to mechanical valves. The risk of hemorrhagic complications persists because of the narrow therapeutic index of warfarin. The risk of bleeding is aggravated further if INR (International normalized ration) is >4.51. One of the most serious complications is an intracranial haemorrhage. The anesthetic management of these patients is challenging with the deranged coagulation and the associated hemodynamic instability which cannot be corrected completely in the limited time specifically if the patient presents with poor GCS and surgeons are demanding for an immediate surgery. It is the anaesthesiologist who has to take stand to reverse anticoagulation to have good perioperative outcome, as failure to reverse is associated with poor outcome 2.
CASE REPORT:
The current admission of a male patient aged 56 was for drowsiness and non-responsiveness from third day following head injury in a road traffic accident. He was discharged after first aid treatment to apparent wounds in a stable condition with full conscious state from local hospital. On third day he deteriorated and got admitted. His GCS (Glasgow Coma Scale) at admission was E1V1M4 (GCS-6). History revealed a surgery for chronic rheumatic heart disease with mitral stenosis with St Jude’s mechanical mitral valve replacement in the year 1992. He was on anticoagulation therapy with 4mg of daily dose of warfarin & the last dose was administered on the previous day in the evening. The blood investigations were within normal limits except an INR of 4.9 with PT of 52.8, APTT 45.1. The recent 2D-Echo showed normal motility of the mechanical mitral valve. CT scan brain showed a subdural hematoma over the right fronto parieto temporal region with a massive midline shift. Immediately after admission and baseline evaluation, neurosurgeons demanded for surgery and evacuation of blood. We decided to correct INR. An urgent correction of INR to at least 2 was advised with transfusion of five bags of fresh frozen plasma, five bags of cryoprecipitate & vitamin K administration. In the meanwhile the patient was stabilized by tracheal intubation in neuro critical care unit and standard monitoring was continued. The intubation was done after preoxygenation with intravenous fentanyl 150 µg and rocuronium was used for neuromuscular blockade. Intravenous xylocaine 1.5 mg/kg was given to avoid intubation response and further risk of bleeding. The patient was mechanically ventilated and shifted to the operating theatre after 3 hours to undergo a decompressive craniotomy. Blood & blood products were arranged and kept standby for intraoperative transfusion. An additional dose of 80 mics of fentanyl & vecuronium 6mg were given and anaesthesia was maintained with O2+Air+sevoflurane (0.7 to 1MAC). Local infiltration on scalp was given to avoid response to skin incision and blood pressure was maintained with mean arterial pressure of 60-80 mmHg. 20g of mannitol was administered 30 minutes prior to craniotomy. Intraoperative transfusion of 2 bags of FFP was done. Blood pressure dropped from 140/90mm Hg to 80/40 mm Hg with evacuation of large volume (around 500 ml) of subdural hematoma despite calculated fluid administration. Blood pressure recovered with volume replacement and transfusion of one unit packed RBC was done for intraoperative hemoglobin value of 8 g/dl. The surgery went uneventful thereafter. The urine output was adequate with respect to duration of surgery. The patient was shifted back to the ICU for elective postoperative ventilation in view of poor preoperative GCS.
Cardiologist opinion was sought regarding postoperative anticoagulation and was started on low molecular weight heparin (LMWH) on postop day one. Patient continued to be on mechanical ventilation. Daily INR monitoring was conducted and it was around 1.2 to 1.4. The GCS showed a slight improvement of E3VtM5 compared to preoperative E1VtM4 over the next 7 days and no further improvement thereafter. He was tracheostomised on day 14th as there was a need for prolonged mechanical ventilation in view of poor GCS though valve function and hemodynamics were normal. The patient had sudden cardiac arrest and could not be revived on day 20.
DISCUSSION:
Warfarin is an oral anticoagulant with its action3 (Figure1) being inhibition of reactivation of vitamin K epoxide to hydroquinone thus inhibiting gamma-carboxylation of glutamate at amino terminus of coagulation factors synthesised in the liver (factor II, VII, IX, X). It has a t1/2 of 36 to 48 hours and its action lasts for 4 to 6 days. It results in prolongation of PT (INR). INR should be used to monitor the dosage requirements of warfarin for safety against bleeding as it has a wide patient variability. 3
One of the various indications for warfarin use is patients with prosthetic heart valves to prevent thromboembolism. The target INR for this category of patients according to the set guidelines is 3 (range of 2.5 – 3.5). The risk of bleeding is aggravated further if INR (International normalized ration) is > 4.5.1 The reported absolute risk of intracranial hemorrhage with anticoagulation is 0.3% to 1.0% per year and the associated mortality is about 60%.The reported risk of subdural hematoma (SDH) with anticoagulation is 4 to 15 fold.4,5 The reported mortality of anticoagulant-related SDH is between 13% and 20%.6
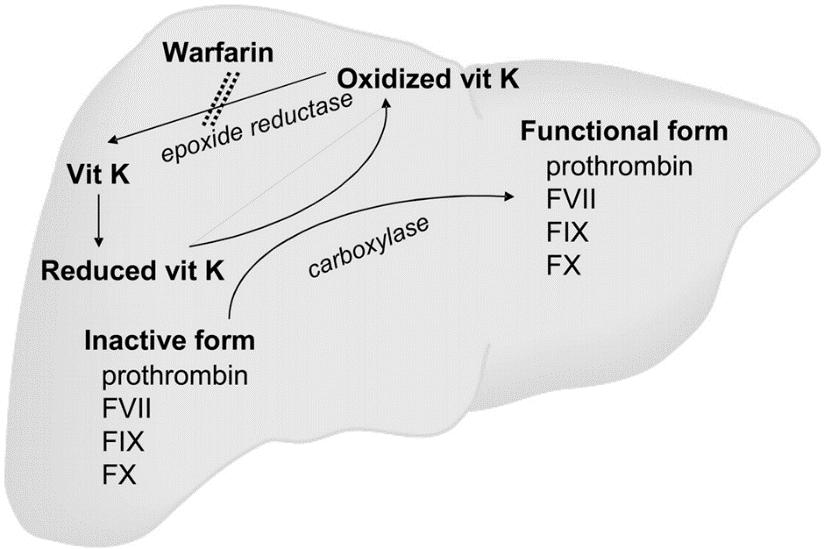
Figure 1: Mechanism of action of warfarin
Acute SDH itself can be fatal and mortality is definitely increased in patients on anticoagulants.7 Failure to achieve reversal preoperatively adds to poor outcome and thus increasing mortality.2 Current guidelines recommend reversal of anticoagulation and normalization of INR to 1.4 which is suitable for most of the neurosurgical procedures.8 For the reversal of anticoagulation the modalities are vitamin K, FFP (Fresh Frozen Plasma), or factor concentrates.7,8,9 The correction may take 9 hours with standard FFP and with factor IX complex in conjuncture with FFP it may take 2.93 hours.8 Recombinant-activated factor VII (rFVIIa) is the best and fastest agent for reversal of anticoagulation.9,10
FFP: The best choice for intracranial hemorrhage though takes 6 to 8 hours or more before INR normalises and the reversal is not always complete. The recommended dose is anywhere between 10 and 40 ml/kg.
PCC (prothrombin Complex Concentrate): It acts within 10 to 15 min & INR normalises in 1 hour. It has limited availability. The dose varies between 25 and 100 units/kg depending on the degree of derangement3.
rVIIa: rapid and complete correction can be achieved.
Vitamin K: 5 to 10 mg intravenously by slow infusion over 30 minutes. It takes 6 – 24 hours to have a therapeutic effect. It is of no use in rapid correction when used alone.
Anesthetic management of patients with intracranial bleed with elevated INR is a challenge due to the following factors:
CONCLUSION:
The patients on anticoagulants presenting post trauma with head injury component must be kept under observation. If airway, ventilation and hemodynamics are taken care of preoperatively, the surgery can be delayed till reversal of anticoagulation is achieved and it will improve the outcome.
Conflict of interest: Nil
Author contribution: All authors took part in design, planning, conduct of the study and data collection, literature review and manuscript preparation
REFERENCES:
1Junior Resident; 2Assistant Professor; 3Professor
Department of Anaesthesiology and Intensive Care, Nizam’s Institute of Medical Sciences, Hyderabad, 500082, India. Email: - chaitanyapa9@gmail.com
Correspondence: Dr. Sapna Annaji Nikhar, Assistant Professor, Department of Anaesthesiology & Intensive Care, Nizam’s Institute of Medical Sciences, Hyderabad, 500082, (India); Telephone: +91 9030460262; E-mail: sapnanikhar@gmail.com,
ABSTRACT:
The use of anticoagulants to prevent thromboembolic complications post mechanical valve replacement is associated with intracranial or subdural hemorrhage. In such cases, the scale has to be balanced to have a good anticoagulation in order to prevent thromboembolism and to have a target INR (International normalized ration) in order to avoid hemorrhages specifically intracranial hemorrhages. A controversy exists on reversal of anticoagulation for emergency surgery and management may differ from case to case. Here, we report a case with massive subdural hematoma on warfarin post mechanical mitral valve replacement for emergency craniotomy and evacuation. Effective optimization and correction of INR by reversing anticoagulation lead to an improved outcome without further increase in thromboembolic complications.
Key words: Anticoagulants; Emergency surgery; Reversal
INTRODUCTION:
Long term anticoagulation is needed to avoid thromboembolic complications due to mechanical valves. The risk of hemorrhagic complications persists because of the narrow therapeutic index of warfarin. The risk of bleeding is aggravated further if INR (International normalized ration) is >4.51. One of the most serious complications is an intracranial haemorrhage. The anesthetic management of these patients is challenging with the deranged coagulation and the associated hemodynamic instability which cannot be corrected completely in the limited time specifically if the patient presents with poor GCS and surgeons are demanding for an immediate surgery. It is the anaesthesiologist who has to take stand to reverse anticoagulation to have good perioperative outcome, as failure to reverse is associated with poor outcome 2.
CASE REPORT:
The current admission of a male patient aged 56 was for drowsiness and non-responsiveness from third day following head injury in a road traffic accident. He was discharged after first aid treatment to apparent wounds in a stable condition with full conscious state from local hospital. On third day he deteriorated and got admitted. His GCS (Glasgow Coma Scale) at admission was E1V1M4 (GCS-6). History revealed a surgery for chronic rheumatic heart disease with mitral stenosis with St Jude’s mechanical mitral valve replacement in the year 1992. He was on anticoagulation therapy with 4mg of daily dose of warfarin & the last dose was administered on the previous day in the evening. The blood investigations were within normal limits except an INR of 4.9 with PT of 52.8, APTT 45.1. The recent 2D-Echo showed normal motility of the mechanical mitral valve. CT scan brain showed a subdural hematoma over the right fronto parieto temporal region with a massive midline shift. Immediately after admission and baseline evaluation, neurosurgeons demanded for surgery and evacuation of blood. We decided to correct INR. An urgent correction of INR to at least 2 was advised with transfusion of five bags of fresh frozen plasma, five bags of cryoprecipitate & vitamin K administration. In the meanwhile the patient was stabilized by tracheal intubation in neuro critical care unit and standard monitoring was continued. The intubation was done after preoxygenation with intravenous fentanyl 150 µg and rocuronium was used for neuromuscular blockade. Intravenous xylocaine 1.5 mg/kg was given to avoid intubation response and further risk of bleeding. The patient was mechanically ventilated and shifted to the operating theatre after 3 hours to undergo a decompressive craniotomy. Blood & blood products were arranged and kept standby for intraoperative transfusion. An additional dose of 80 mics of fentanyl & vecuronium 6mg were given and anaesthesia was maintained with O2+Air+sevoflurane (0.7 to 1MAC). Local infiltration on scalp was given to avoid response to skin incision and blood pressure was maintained with mean arterial pressure of 60-80 mmHg. 20g of mannitol was administered 30 minutes prior to craniotomy. Intraoperative transfusion of 2 bags of FFP was done. Blood pressure dropped from 140/90mm Hg to 80/40 mm Hg with evacuation of large volume (around 500 ml) of subdural hematoma despite calculated fluid administration. Blood pressure recovered with volume replacement and transfusion of one unit packed RBC was done for intraoperative hemoglobin value of 8 g/dl. The surgery went uneventful thereafter. The urine output was adequate with respect to duration of surgery. The patient was shifted back to the ICU for elective postoperative ventilation in view of poor preoperative GCS.
Cardiologist opinion was sought regarding postoperative anticoagulation and was started on low molecular weight heparin (LMWH) on postop day one. Patient continued to be on mechanical ventilation. Daily INR monitoring was conducted and it was around 1.2 to 1.4. The GCS showed a slight improvement of E3VtM5 compared to preoperative E1VtM4 over the next 7 days and no further improvement thereafter. He was tracheostomised on day 14th as there was a need for prolonged mechanical ventilation in view of poor GCS though valve function and hemodynamics were normal. The patient had sudden cardiac arrest and could not be revived on day 20.
DISCUSSION:
Warfarin is an oral anticoagulant with its action3 (Figure1) being inhibition of reactivation of vitamin K epoxide to hydroquinone thus inhibiting gamma-carboxylation of glutamate at amino terminus of coagulation factors synthesised in the liver (factor II, VII, IX, X). It has a t1/2 of 36 to 48 hours and its action lasts for 4 to 6 days. It results in prolongation of PT (INR). INR should be used to monitor the dosage requirements of warfarin for safety against bleeding as it has a wide patient variability. 3
One of the various indications for warfarin use is patients with prosthetic heart valves to prevent thromboembolism. The target INR for this category of patients according to the set guidelines is 3 (range of 2.5 – 3.5). The risk of bleeding is aggravated further if INR (International normalized ration) is > 4.5.1 The reported absolute risk of intracranial hemorrhage with anticoagulation is 0.3% to 1.0% per year and the associated mortality is about 60%.The reported risk of subdural hematoma (SDH) with anticoagulation is 4 to 15 fold.4,5 The reported mortality of anticoagulant-related SDH is between 13% and 20%.6
Figure 1: Mechanism of action of warfarin
Acute SDH itself can be fatal and mortality is definitely increased in patients on anticoagulants.7 Failure to achieve reversal preoperatively adds to poor outcome and thus increasing mortality.2 Current guidelines recommend reversal of anticoagulation and normalization of INR to 1.4 which is suitable for most of the neurosurgical procedures.8 For the reversal of anticoagulation the modalities are vitamin K, FFP (Fresh Frozen Plasma), or factor concentrates.7,8,9 The correction may take 9 hours with standard FFP and with factor IX complex in conjuncture with FFP it may take 2.93 hours.8 Recombinant-activated factor VII (rFVIIa) is the best and fastest agent for reversal of anticoagulation.9,10
FFP: The best choice for intracranial hemorrhage though takes 6 to 8 hours or more before INR normalises and the reversal is not always complete. The recommended dose is anywhere between 10 and 40 ml/kg.
PCC (prothrombin Complex Concentrate): It acts within 10 to 15 min & INR normalises in 1 hour. It has limited availability. The dose varies between 25 and 100 units/kg depending on the degree of derangement3.
rVIIa: rapid and complete correction can be achieved.
Vitamin K: 5 to 10 mg intravenously by slow infusion over 30 minutes. It takes 6 – 24 hours to have a therapeutic effect. It is of no use in rapid correction when used alone.
Anesthetic management of patients with intracranial bleed with elevated INR is a challenge due to the following factors:
- Emergency- Large bleed with midline shift and poor patient GCS.
- The risk of intraoperative bleeding & re-bleeding continues.
- Risky the central line placement but needed to monitor fluid status.
- Valve malfunction leading to hemodynamic disturbances.
- The use of blood products with strict monitoring to avoid fluid overload and keep watch on urine output.
CONCLUSION:
The patients on anticoagulants presenting post trauma with head injury component must be kept under observation. If airway, ventilation and hemodynamics are taken care of preoperatively, the surgery can be delayed till reversal of anticoagulation is achieved and it will improve the outcome.
Conflict of interest: Nil
Author contribution: All authors took part in design, planning, conduct of the study and data collection, literature review and manuscript preparation
REFERENCES:
- Stein PD, Grandison D, Hua TA, et al. Therapeutic levels of oral anticoagulation with warfarin in patients with mechanical prosthetic heart valves: review of literature recommendations based on international normalized ratio. Postgrad Med J 1994; 70 (Suppl. 1): S72-S85.
- Kawamata T, Takeshita M, Kubo O, Izawa M, Kagawa M, Takakura K. Management of intracranial hemorrhage associated with anticoagulant therapy. Surg Neurol. 1995 Nov; 44(5):438-42. [PubMed]
- Ray B, Keyrouz SG. Management of anticoagulant-related intracranial hemorrhage: an evidence-based review. Crit Care. 2014 May 23;18(3):223. [PubMed] [Free full text]
- Hart RG, Boop BS, Anderson DC. Oral anticoagulants and intracranial hemorrhage. Facts and hypothesis. Stroke. 1995 Aug;26(21):1471-7. [PubMed] [Free full text]
- Wintzen AR, Tijssen JG. Subdural hematoma and oral anticoagulant therapy. Arch Neurol. 1982 Feb;39(2):69-72. [PubMed]
- Hylek EM, Singer DE. Risk factors for intracranial hemorrhage in outpatients taking warfarin. Ann Intern Med. 1994 Jun 1;120(11):897-902. [PubMed]
- Chowdary GVS, Naryanan TJ, Basha PSA, Murthy TVRK, Murthy JMK. Anticoagulant-related subdural hematoma in patients with mechanical heart valves. Neurology Asia. 2005;10:13–19.
- Boulis NM, Bobek MP, Schmaier A, Hoff JT. Use of factor IX complex in warfarin-related intracranial hemorrhage. Neurosurgery. 1999 Nov;45(5):1118-9. [PubMed]
- Hirsh J, Fuster V, Ansell J, Halperin JL, American Heart Association/American College of Cardiology Foundation. American Heart Association/American College of Cardiology Foundation guide to warfarin therapy. Circulation. 2003 May 7;41(9):1633-52.. [PubMed] [Free full text]
- Phan TG, Koh M, Wijdicks EF. Safety of discontinuation of anticoagulation in patients with intracranial hemorrhage at high thromboembolic risk. Arch Neurol. 2000 Dec; 57(12):1710-13. [PubMed]