Nadeem Sharif 1, Naeem Bukhari 2, Zubair Ahmed Yousfani 3, Afshan Saleem 4, Amina Arif 5, Hazrat Abbas 2, Muhammad Adeeb Khan6
1-Department of Medical Laboratory Technology, University of Haripur, Pakistan.
2-Centre for Human Genetics, Hazara University Mansehra, Pakistan.
3-Department of Surgery, Liaquat University of Medical and Health Sciences, Jamshoro, Pakistan.
4-Department of Microbiology, University of Haripur, Pakistan.
5-Faculty of Life Sciences, University of Central Punjab, Pakistan
6-Department of Zoology, Women University of Azad Jammu and Kashmir, Bagh, Pakistan.
Correspondence: Naeem Bukhari, M. Phil Research Scholar, Centre for Human Genetics, Hazara University Mansehra, Pakistan;
E-mail: naeembukhari20@gmail.com; Ph: +92-3315493532
Abstract
Background & Objectives: Since COVID-19 outbreak, and the first confirmed case in Pakistan, Pakistani government, media and health departments made significant efforts to ensure that the people stay at homes to avoid massive spread of COVID-19.
Our study aimed to fill the existing gaps in knowledge and research based upon clinical symptoms and gender association of novel coronavirus (COVID-19) among different age groups in Punjab Pakistan.
Methodology: Current cohort study was designed at Centre For Human Genetics, Hazara University Mansehra and conducted at Provisional Public Health Reference Lab, Primary and Secondary Healthcare Department Lahore-Pakistan.
Results: Based on set objectives males were more prone (76%) to COVID-19 then females (24%) from one hundred confirmed cases of SARS-Co-2 enrolled study participants. In comparison to older age participants and children’s youngsters (16-30-y age) were at greater risk 35% of COVID-19 infection with mean age of 34.23 ≈ 1.60 ± (P ˂ 0.05). Only 13% cases with no visible symptoms of SARS-Co-2 were tested positive for COVID-19 PCR test.
Spread patterns of COVID-19 are ultimately based upon exposure to COVID-19 and irrespective of any immunological association reported yet.
Conclusion: we recommend country leadership, media houses and researchers to understand differences in age wise spread patterns of (COVID-19) versus age wise mortality patterns of COVID-19 to educate the common public accordingly.
Key words: COVID-19; Age susceptibility; Gender
Abbreviations: PCR = polymerase chain reaction, SARS = severe acute respiratory syndrome, ARDS = Acute respiratory distress syndrome
Citation: Sharif N, Bukhari N, Yousfani ZA, Saleem A, Arif A, Abbas H, Khan MA. Gender and age factors in COVID-19 patients in Punjab, Pakistan; A cohort study. Anaesth. pain intensive care 2020;24(4):435-439.
Received: 8 June 2020, Reviewed: 30 June 2020, Revised: 19 July 2020, Accepted: 26 July 2020
Introduction
By the end of 2019, severe unusual cases of acute pneumonia were reported in Wuhan, (Hubei province) China, that outspread speedily to other provinces of China as well as to other parts of the world.1-5 Causative agent identified was novel coronavirus by Center for Disease Control and Prevention (CDC) China and declared officially on 7th January 2020.5 International Committee on Taxonomy of Viruses renamed it as severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2).6 World Health Organization (WHO) named it COVID-19. Before COVID-19, two other outbreaks of viruses from the same family occurred i.e. severe acute respiratory syndrome by coronavirus (SARS-CoV) outbreak in 2002, and Middle East respiratory syndrome coronavirus (MERS-CoV) outbreak in 2012.7-8
Novel coronavirus has been classified in subgroup beta-coronavirus due to close similarity to this group.9,10 It seems from the current evidence that transmission to humans occurred from wild animals sold in sea food market.1-3 COVID-19 exhibits high infectivity than SARS-CoV and MERS-CoV as it has high transmissibility and strong pathogenicity. This high infectivity as explained by latest research is due to higher binding affinity of COVID-19 S to angiotensin converting enzyme 2 than SARS-CoV.11 Droplets and direct contact have been found to be the main source of transmission of COVID-19. Viral load in symptomatic patients of COVID-19 are like that of an asymptomatic patient that indicates the transmission potential by asymptomatic ones.12 The research has demonstrated that infants and children may also be infected by COVID-19.13 But there is no evidence about its vertical transmission.14
Imaging examination is rapid and appropriate method to diagnose and track disease progress, but findings may overlap with other inflammatory or infectious disease.15
PCR is used as a diagnostic test for COVID -19 all over the world, hence it is also the recommended method in Pakistan.16 As per media reports males are considered more prone to COVID-19 in Pakistan in comparison to females. Our research hypothesis aims to confirm or negate it; our null hypothesis is based upon non-significant role of gender following COVID-19 seropositivity.
The data acquisition on clinical pattern and outcomes of COVID-19 patients from Pakistan is still in progress but is of utmost importance to combat the disease. This cohort study investigated gender wise positivity trends of Covid-19 in different age groups among multiple areas of Punjab, Pakistan.
Methodology
Current descriptive study was conducted at Provincial Public Health Reference Laboratory, Primary and Secondary Healthcare Department. Lahore-Pakistan. Confirmed positive cases of COVID-19 from six different geographic locations of Punjab were included in the study following multi-purpose convenient sampling method, after ethical approval from the ethical committee of the laboratory, and The Centre for Human Genetics, Hazara University Mansehra Research Ethical Committee. Maximum duration of the study was one month (15th March-15th April 2020). Patients from both genders, but positive for COVID-19, were considered for further analysis.
About 5 ml of blood samples were collected from one hundred clinically confirmed patients of COVID-19 from quarantine centers of selected hospitals from six different regions, e.g., DG Khan, Samanabad, Bakhar, Gujrat, Gujranwala, Lahore city under standard operating procedures (SOPs) of blood collection from COVID-19 patients. In the next step the sample were transported to Provincial Public Health Reference Laboratory by following standard SOPs for sample transportations. The viral RNA was extracted from each sample and amplified by using specific probes as per WHO recommended PCR (polymerase chain reaction protocols.17
Patient data were further analyzed, tested and tabulated by using SPSS version 21.0, Revman5.30 and multiple tools of Microsoft office version 2010.
Results
Based on set objectives assessing gender and age specific distribution of COVID-19 in Punjab by using WHO recommended PCR method, about 76% patients were males and 24 were females. Based on clinical presentation patients were classified into two groups, Group-I, Group-II and Group-III (Table 1).
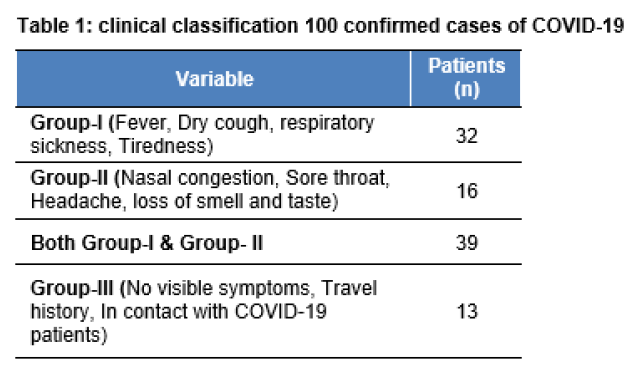
Most of the patients (39%) represent clinical symptoms of fever, dry cough, respiratory difficulty, tiredness, nasal congestion, sore throat, headache and loss of smell/taste. Mean age of the enrolled COVID-19 patients was 34.25 ± 1.60 y.
Based on the age, the group 16-30 y was more prone (35%) to infection. Whereas, age groups 61-75 y and 76 -91 y were least prone to infection (Table 3). The pediatric group (1-15 y) made up 9 % of the cases. A significant increase in the frequency of COVID-19 was recorded, moving from less populated areas towards more populated ones in Punjab, Pakistan. The number of cases were noted in a decreasing order; Lahore City (36 %), Gujrat (19%), Samanabad (19%), Bakhar (9%) and Dera Ghazi Khan (9%) (Table 2).
Gender based comparative geographic exposure analysis to COVID-19 represents an average odd ratio (OR) = 8.43 at 95% confidence interval (CI). The subjected OR reveals huge gender-based gap following COVID-19 exposure. There was insignificant heterogeneity recorded in testing methodology (Tau2 = 0.00) at p < 0.45 and I2 = 0 % (Table 2).
We also assessed the age specific risk ratio (RR) of COVID-19 in both genders. An average RR of COVID-19 infections among both genders was recorded as 3.08 at 95 % CI by following random model analysis approach (Table 3).
Table 2: Distribution of COVID-19 in different geographic of Punjab-Pakistan
Table 3: Age wise Distribution of COVID-19 in Punjab-Pakistan
The lower Chi2 values (6.04) represent a significant relationship among different age groups in terms of COVID-19 infection in both genders. There was insignificant heterogeneity recorded in opted methodology. The I2 = 17 % assures the significance of the p-value. As the overall testing effect value (Z = 6.08) depends on the p-value and I2 value.
The overall statistical outcomes suggest that, in case of zero heterogeneity, lower I2 and greater p-value, we accept the null hypothesis declaring that, the infections of COVID-19 is independent of gender, ultimately it depends on exposure to COVID-19.
Discussion
Current study reported that males were more prone (76%) to COVID-19 in comparison to females (24%). A research report of Begum Sadaquat et al.18 highlighted lower participation of women in workforce in Pakistan due to cultural, social and religious barriers, which indirectly restrict the females going to populated areas. Religious teachings also encourage women to stay at home. This factor alone has minimized the chances of female exposure to COVID-19. Another research report pointed out that 63% of the Pakistani population is relatively younger, e.g., 15-33 y age group. Most of the population in Punjab is linked to the labor profession and is unmarried in comparison to Khyber-Pakhtunkhwa and Baluchistan provinces. In Punjab, Lahore City is considered as the central hub of labor market in the region.19-20 These studies are in accordance to our outcomes suggesting age group 16-30 y, being at greater risk of COVID-19 exposure; and more populated areas like, Lahore City having the highest (36 %) cases of COVID-19 of the total recorded cases (Table 2).
Our outcomes declaring higher number of males infected with COVID-19 in Punjab Pakistan are in concordance with a recent study by Shi Y, et al,21 focusing 487 cases in Wuhan-China and reported males were more prone to COVID-19 (73.3 %) in comparison to female (26.5 %).
Conclusion
We conclude that in Punjab, Pakistan, males are more prone to the viral infection in the current outbreak of COVID-19 as compared to females, which is probably due to higher exposure to COVID-19 by the males. Younger population (age range 16-30 y) is mostly infected by COVID-19 based upon their outside commitments to job, work or enjoyment.
Recommendations
We recommend country leadership, media houses and researchers to understand differences in age wise spread patterns of (COVID-19) and age wise mortality patterns of COVID-19 to educate the common public to overcome its further progression.
Conflict of interests
None
Authors’ contribution
NS: Patient selection, testing and clinical investigation
NB: Questionnaire design, data compilation and Analysis, manuscript editing
ZAY: Safety guidelines, personnel protection guidance, methodology chapter contribution
AS: Introduction and literature review, chapter contribution
AA: Results chapter contribution and plagiarism check
HA: Abstract and discussion drafting
MAK: Reviewing, correction, referencing assessment and journal selection.
References
1-Department of Medical Laboratory Technology, University of Haripur, Pakistan.
2-Centre for Human Genetics, Hazara University Mansehra, Pakistan.
3-Department of Surgery, Liaquat University of Medical and Health Sciences, Jamshoro, Pakistan.
4-Department of Microbiology, University of Haripur, Pakistan.
5-Faculty of Life Sciences, University of Central Punjab, Pakistan
6-Department of Zoology, Women University of Azad Jammu and Kashmir, Bagh, Pakistan.
Correspondence: Naeem Bukhari, M. Phil Research Scholar, Centre for Human Genetics, Hazara University Mansehra, Pakistan;
E-mail: naeembukhari20@gmail.com; Ph: +92-3315493532
Abstract
Background & Objectives: Since COVID-19 outbreak, and the first confirmed case in Pakistan, Pakistani government, media and health departments made significant efforts to ensure that the people stay at homes to avoid massive spread of COVID-19.
Our study aimed to fill the existing gaps in knowledge and research based upon clinical symptoms and gender association of novel coronavirus (COVID-19) among different age groups in Punjab Pakistan.
Methodology: Current cohort study was designed at Centre For Human Genetics, Hazara University Mansehra and conducted at Provisional Public Health Reference Lab, Primary and Secondary Healthcare Department Lahore-Pakistan.
Results: Based on set objectives males were more prone (76%) to COVID-19 then females (24%) from one hundred confirmed cases of SARS-Co-2 enrolled study participants. In comparison to older age participants and children’s youngsters (16-30-y age) were at greater risk 35% of COVID-19 infection with mean age of 34.23 ≈ 1.60 ± (P ˂ 0.05). Only 13% cases with no visible symptoms of SARS-Co-2 were tested positive for COVID-19 PCR test.
Spread patterns of COVID-19 are ultimately based upon exposure to COVID-19 and irrespective of any immunological association reported yet.
Conclusion: we recommend country leadership, media houses and researchers to understand differences in age wise spread patterns of (COVID-19) versus age wise mortality patterns of COVID-19 to educate the common public accordingly.
Key words: COVID-19; Age susceptibility; Gender
Abbreviations: PCR = polymerase chain reaction, SARS = severe acute respiratory syndrome, ARDS = Acute respiratory distress syndrome
Citation: Sharif N, Bukhari N, Yousfani ZA, Saleem A, Arif A, Abbas H, Khan MA. Gender and age factors in COVID-19 patients in Punjab, Pakistan; A cohort study. Anaesth. pain intensive care 2020;24(4):435-439.
Received: 8 June 2020, Reviewed: 30 June 2020, Revised: 19 July 2020, Accepted: 26 July 2020
Introduction
By the end of 2019, severe unusual cases of acute pneumonia were reported in Wuhan, (Hubei province) China, that outspread speedily to other provinces of China as well as to other parts of the world.1-5 Causative agent identified was novel coronavirus by Center for Disease Control and Prevention (CDC) China and declared officially on 7th January 2020.5 International Committee on Taxonomy of Viruses renamed it as severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2).6 World Health Organization (WHO) named it COVID-19. Before COVID-19, two other outbreaks of viruses from the same family occurred i.e. severe acute respiratory syndrome by coronavirus (SARS-CoV) outbreak in 2002, and Middle East respiratory syndrome coronavirus (MERS-CoV) outbreak in 2012.7-8
Novel coronavirus has been classified in subgroup beta-coronavirus due to close similarity to this group.9,10 It seems from the current evidence that transmission to humans occurred from wild animals sold in sea food market.1-3 COVID-19 exhibits high infectivity than SARS-CoV and MERS-CoV as it has high transmissibility and strong pathogenicity. This high infectivity as explained by latest research is due to higher binding affinity of COVID-19 S to angiotensin converting enzyme 2 than SARS-CoV.11 Droplets and direct contact have been found to be the main source of transmission of COVID-19. Viral load in symptomatic patients of COVID-19 are like that of an asymptomatic patient that indicates the transmission potential by asymptomatic ones.12 The research has demonstrated that infants and children may also be infected by COVID-19.13 But there is no evidence about its vertical transmission.14
Imaging examination is rapid and appropriate method to diagnose and track disease progress, but findings may overlap with other inflammatory or infectious disease.15
PCR is used as a diagnostic test for COVID -19 all over the world, hence it is also the recommended method in Pakistan.16 As per media reports males are considered more prone to COVID-19 in Pakistan in comparison to females. Our research hypothesis aims to confirm or negate it; our null hypothesis is based upon non-significant role of gender following COVID-19 seropositivity.
The data acquisition on clinical pattern and outcomes of COVID-19 patients from Pakistan is still in progress but is of utmost importance to combat the disease. This cohort study investigated gender wise positivity trends of Covid-19 in different age groups among multiple areas of Punjab, Pakistan.
Methodology
Current descriptive study was conducted at Provincial Public Health Reference Laboratory, Primary and Secondary Healthcare Department. Lahore-Pakistan. Confirmed positive cases of COVID-19 from six different geographic locations of Punjab were included in the study following multi-purpose convenient sampling method, after ethical approval from the ethical committee of the laboratory, and The Centre for Human Genetics, Hazara University Mansehra Research Ethical Committee. Maximum duration of the study was one month (15th March-15th April 2020). Patients from both genders, but positive for COVID-19, were considered for further analysis.
About 5 ml of blood samples were collected from one hundred clinically confirmed patients of COVID-19 from quarantine centers of selected hospitals from six different regions, e.g., DG Khan, Samanabad, Bakhar, Gujrat, Gujranwala, Lahore city under standard operating procedures (SOPs) of blood collection from COVID-19 patients. In the next step the sample were transported to Provincial Public Health Reference Laboratory by following standard SOPs for sample transportations. The viral RNA was extracted from each sample and amplified by using specific probes as per WHO recommended PCR (polymerase chain reaction protocols.17
Patient data were further analyzed, tested and tabulated by using SPSS version 21.0, Revman5.30 and multiple tools of Microsoft office version 2010.
Results
Based on set objectives assessing gender and age specific distribution of COVID-19 in Punjab by using WHO recommended PCR method, about 76% patients were males and 24 were females. Based on clinical presentation patients were classified into two groups, Group-I, Group-II and Group-III (Table 1).
Most of the patients (39%) represent clinical symptoms of fever, dry cough, respiratory difficulty, tiredness, nasal congestion, sore throat, headache and loss of smell/taste. Mean age of the enrolled COVID-19 patients was 34.25 ± 1.60 y.
Based on the age, the group 16-30 y was more prone (35%) to infection. Whereas, age groups 61-75 y and 76 -91 y were least prone to infection (Table 3). The pediatric group (1-15 y) made up 9 % of the cases. A significant increase in the frequency of COVID-19 was recorded, moving from less populated areas towards more populated ones in Punjab, Pakistan. The number of cases were noted in a decreasing order; Lahore City (36 %), Gujrat (19%), Samanabad (19%), Bakhar (9%) and Dera Ghazi Khan (9%) (Table 2).
Gender based comparative geographic exposure analysis to COVID-19 represents an average odd ratio (OR) = 8.43 at 95% confidence interval (CI). The subjected OR reveals huge gender-based gap following COVID-19 exposure. There was insignificant heterogeneity recorded in testing methodology (Tau2 = 0.00) at p < 0.45 and I2 = 0 % (Table 2).
We also assessed the age specific risk ratio (RR) of COVID-19 in both genders. An average RR of COVID-19 infections among both genders was recorded as 3.08 at 95 % CI by following random model analysis approach (Table 3).
Table 2: Distribution of COVID-19 in different geographic of Punjab-Pakistan
| Geographical Area | Gender | Total | % Ratio | Odd Ratio
[M-H, Random, CI, 95 % CI] |
|
| Male (PCR+VE) | Female (PCR+VE) | ||||
| Bakhar | 7 | 2 | 9 | 8.50% | 12.25 [1.33, 113.06] |
| DG Khan | 6 | 3 | 9 | 10.90% | 4.00 [0.56, 28.40] |
| Gujranwala | 2 | 0 | 2 | 2.30% | 25.00 [0.34, 1831.59] |
| Gujrat | 14 | 5 | 19 | 20.10% | 7.84 [1.85, 33.23] |
| Lahore City | 25 | 11 | 36 | 41.80% | 5.17 [1.89, 14.08] |
| Safdarabad | 6 | 0 | 6 | 2.50% | 169.00 [2.89, 9875.38] |
| Samanabad | 16 | 3 | 19 | 13.80% | 28.44 [4.97,162.12] |
| Total (95% CI) | 76 | 24 | 100 | 100.00% | 8.43 [4.41, 16.12] |
| Heterogeneity: Tau2 = 0.00; Chi 2 = 5.80 , Df= 6 (p = 0.45 ); I 2 = 0%,
Test for overall effect: Z = 6.45 (p < 0.00001) |
|||||
| Age groups (y) | Gender | Total | % Ratio | Odd Ratio
[M-H, Random, CI, 95 % CI] |
|||||
| Male (PCR+VE) | Female (PCR+VE) | ||||||||
| 1-15 | 9 | 0 | 9 | 2.00% | 19.00 [1.27, 284.24] | ||||
| 16-30 | 28 | 7 | 35 | 28.0% | 4.00 [2.02, 7.92] | ||||
| 31-45 | 22 | 8 | 30 | 32.0% | 2.75 [1.46, 5.17] | ||||
| 46-60 | 15 | 8 | 23 | 32.10% | 1.88 [0.99, 3.54] | ||||
| 61-75 | 1 | 1 | 2 | 4.0% | 1.00 [0.14, 7.10] | ||||
| 76-91 | 1 | 0 | 1 | 2.0% | 3.00 [0.24, 37.67] | ||||
| Total (95% CI) | 76 | 24 | 100 | 100.00% | 3.08 [2.14, 4.43] | ||||
| Heterogeneity: Tau2 = 0.00 ; Chi 2 = 6.04 , Df= 5 (p = 0.30); I 2 = 17%, Test for overall effect : Z = 6.08 (p < 0.00001) | |||||||||
The overall statistical outcomes suggest that, in case of zero heterogeneity, lower I2 and greater p-value, we accept the null hypothesis declaring that, the infections of COVID-19 is independent of gender, ultimately it depends on exposure to COVID-19.
Discussion
Current study reported that males were more prone (76%) to COVID-19 in comparison to females (24%). A research report of Begum Sadaquat et al.18 highlighted lower participation of women in workforce in Pakistan due to cultural, social and religious barriers, which indirectly restrict the females going to populated areas. Religious teachings also encourage women to stay at home. This factor alone has minimized the chances of female exposure to COVID-19. Another research report pointed out that 63% of the Pakistani population is relatively younger, e.g., 15-33 y age group. Most of the population in Punjab is linked to the labor profession and is unmarried in comparison to Khyber-Pakhtunkhwa and Baluchistan provinces. In Punjab, Lahore City is considered as the central hub of labor market in the region.19-20 These studies are in accordance to our outcomes suggesting age group 16-30 y, being at greater risk of COVID-19 exposure; and more populated areas like, Lahore City having the highest (36 %) cases of COVID-19 of the total recorded cases (Table 2).
Our outcomes declaring higher number of males infected with COVID-19 in Punjab Pakistan are in concordance with a recent study by Shi Y, et al,21 focusing 487 cases in Wuhan-China and reported males were more prone to COVID-19 (73.3 %) in comparison to female (26.5 %).
Conclusion
We conclude that in Punjab, Pakistan, males are more prone to the viral infection in the current outbreak of COVID-19 as compared to females, which is probably due to higher exposure to COVID-19 by the males. Younger population (age range 16-30 y) is mostly infected by COVID-19 based upon their outside commitments to job, work or enjoyment.
Recommendations
We recommend country leadership, media houses and researchers to understand differences in age wise spread patterns of (COVID-19) and age wise mortality patterns of COVID-19 to educate the common public to overcome its further progression.
Conflict of interests
None
Authors’ contribution
NS: Patient selection, testing and clinical investigation
NB: Questionnaire design, data compilation and Analysis, manuscript editing
ZAY: Safety guidelines, personnel protection guidance, methodology chapter contribution
AS: Introduction and literature review, chapter contribution
AA: Results chapter contribution and plagiarism check
HA: Abstract and discussion drafting
MAK: Reviewing, correction, referencing assessment and journal selection.
References
- Chen H, Guo J, Wang C, Luo F, Yu X, Zhang W, et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: a retrospective review of medical records. The Lancet. 2020;395:809- [PubMed] [Free full text] DOI: 10.1016/s0140‐6736(20)30360‐3.
- Yang X, Yu Y, Xu J, Shu H, Xia J, Liu H, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med 2020;8:475–81; Published Online February 21, [Free full text] DOI: 1016/S2213-2600(20)30079-5
- Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020; 395: 497–506. [PubMed] [Free full text] DOI: 1016/S0140-6736(20)30183-5
- Holshue ML, DeBolt C, Lindquist S, Lofy KH, Wiesman J, Bruce H, et al. First case of 2019 novel coronavirus in the United States. N Engl J Med 2020 Mar 5;382(10):929-936. [PubMed] [Free full text] DOI: 1056/NEJMoa2001191
- Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med 2020;382(8):727-733. [PubMed] [Free full text] DOI: 1056/NEJMoa2001017
- Zhang X, Cai H, Hu J, Lian J, Gu J, Zhang S, et al. Epidemiological, clinical characteristics of cases of SARS-CoV-2 infection with abnormal imaging findings, International Journal of Infectious Diseases 2020, [PubMed] [Free full text] DOI: 1016/j.ijid.2020.03.040
- Chen J. Pathogenicity and transmissibility of 2019-nCoVd A quick overview and comparison with other emerging viruses. Microbes and Infection 22 (2020) 69-71 [PubMed] [Free full text] DOI: 1016/j.micinf.2020.01.004
- Cui J, Li F, Shi ZL. Origin and evolution of pathogenic coronaviruses. Nat Rev Microbiol 2019;17:181e92. [PubMed] [Free full text] DOI: 1038/s41579-018-0118-9
- Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus–Infected Pneumonia inWuhan, China. JAMA;2020;323:1061-1069. [PubMed] [Free full text] DOI: 1001/jama.2020.1585
- Pyrc K, Berkhout B, Van Der Hoek L. Identification of new human coronaviruses. Expert Review of Anti-infective Therapy 2007;5(2):245–53. [PubMed] [Free full text] DOI: 1586/14787210.5.2.245
- Wrapp D, Wang N, Corbett KS, et al. Cryo-EM structure of the 2019-nCoV spike in the prefusionconformation. Science. 2020 Mar 13;367(6483):1260-1263. [PubMed] [Free full text] DOI: 1126/science.abb2507
- Zou L, Ruan F, Huang M, et al. SARS-CoV-2 viral load in upper respiratory specimens of infected patients. N Engl J Med. 2020: Mar 19;382(12):1177-1179. [PubMed] [Free full text] DOI: 1056/NEJMc2001737
- Wei M, Yuan J, Liu Y, Fu T, Yu X, Zhang ZJ. Novel coronavirus infection in hospitalized infants under 1 year of age in China. JAMA. 2020 Feb 14;323(13):1313-1314. [PubMed] [Free full text] DOI: 1001/jama.2020.2131
- Chen N, Zhou M, Dong X, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet 2020; 395: 507–13. [PubMed] [Free full text] DOI: 1016/S0140-6736(20)30211-7
- Chung M, Bernheim A, Mei X, Zhang N, Huang M, Zeng X, et al. CT Imaging Features of 2019 Novel Coronavirus (2019-nCoV). Radiology 2020 Apr;295(1):202-207. [PubMed] [Free full text] DOI: 1148/radiol.2020200230
- Waris A, Atta UK, Ali M, Asmat A, Baset A. COVID-19 outbreak: current scenario of Pakistan. New Microbe and New Infect 2020; 35: 100681 [PubMed] [Free full text] DOI: 1016/j.nmni.2020.100681
- Corman VM, Landt O, Kaiser M, Molenkamp R, Meijer A, Chu DK, et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Euro Surveill 2020;25: [PubMed] [Free full text] DOI:10.2807/1560-7917.ES.2020.25.3.2000045
- Begum Sadaquat, M., Sheikh QA. (2011). Employment situation of women in Pakistan. International Journal of Social Economics, 38(2), 98–113. [Free full text] DOI: 1108/03068291111091981
- Hafeez E, Faseeh S. (2018). Growing Population of Pakistani Youth: A Ticking Time Bomb or a Demographic Dividend. Journal of Education and Educational Development. 5(2). [Free full text] DOI: 22555/joeed.v5i2.2022
- Khan MZ, Hafeez A. Economic activities and unmarried labour, Economic Research-Ekonomska Istraživanja 2017;30(1):985-991. [Free full text] DOI: 1080/1331677X.2017.1305805
- Shi Y, Yu X, Zhao H, Wang H, Zhao R, & Sheng J. Host susceptibility to severe COVID-19 and establishment of a host risk score: findings of 487 cases outside Wuhan. Crit care 2020;24(1):108. [PubMed] [Free full text] DOI: 1186/s13054-020-2833-7