Anees Muhammad1, Muhammad Owais1, Nasir Ali1, Hidayat Khan1
1M.Phil. Lecturer, Department of Medical Laboratory Technology, College of Medical Technology, Bacha Khan Medical College, Mardan, Pakistan.
2M.Phil, Lecturer, Department of Medical Laboratory Technology, College of Medical Technology, Bacha Khan Medical College, Mardan, Pakistan.
3M.Phil, Lecturer, Department of Medical Laboratory Technology, College of Medical Technology, Bacha Khan Medical College, Mardan, Pakistan.
4Ph.D, Assistant Professor, Department of Medical Laboratory Technology, College of Medical Technology, Bacha Khan Medical College, Mardan, Pakistan.
Correspondence: Hidayat Khan,
Lecturer, Department of Medical Laboratory Technology, College of Medical Technology, Bacha Khan Medical College, Mardan, (Pakistan)
E-mail: farhansf9@gmail.com
ABSTRACT
The current outbreak of Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) has attained the dimensions of a pandemic and World Health Organization (WHO) has declared it a global emergency and given it a name of COVID-19. It may remain asymptomatic, but usually presents as influenza-like symptoms initially. It spreads from zoonotic sources, which are still under investigation. Real Time Polymerase Chain Reaction (RT-PCR) is the only available diagnostic and confirmatory lab assay for SARS-CoV-2. There is no specific antiviral drug or vaccine against SARS-CoV-2, hence infected and suspected cases are dependent on supportive treatment along with few anti-HIV drugs. Evidence suggests that, in Pakistan, all cases have returned from Iran and Saudi Arabia after pilgrimage. The number of patients has been increasing gradually. Almost all of the neighboring countries of Pakistan are suffering from an outbreak. So, a big threat is there. Pakistani health authorities need to take critical action urgently. Moreover, it is necessary to take basic preventive measurements including hand washing, use of face masks, keeping the distance from suspected patients and avoiding unnecessary traveling to overcrowded areas. It is concluded that the developing countries might be at higher risk including Pakistan. Personnel and community-based strategy is required to avoid any serious consequences in Pakistan. We searched relevant studies and papers from Google, Google Scholar, National Institute of Health (Pakistan) and WHO by using various medical subject heading (MeSH) terms including COVID-19, SARS-CoV-2, MERS, Preventive Measurements of COVID etc. All downloaded articles were carefully read and conclusions drawn.
Key words: SARS-CoV-2; Epidemic; Pandemic; COVID-19; Pakistan
Citation: Muhammad A, Owais M, Ali N, Khan H. COVID-19 pandemic and precautionary measures in Pakistan. Anaesth pain intensive care 2020;24(1):_
DOI: https://doi.org/10.35975/apic.v24i1.
Received – 20 March 2020; Reviewed – 22 March 2020; Accepted - 27 March 2020
INTRODUCTION
Coronavirus is an enveloped single-stranded RNA virus with positive polarity. The name "corona means crown", the spikes around the surface of the Coronavirus make virus crown shape. Subtypes of coronaviruses include Human Coronavirus-229E (HCoV-229E), HKU1-CoV, HCoV-NL63, and HCoV-OC43 including in common cold disease.1 Few are human transmitted coronaviruses, whereas the majority can be identified in animals. Before a few decades, coronavirus was considered animal virus especially bat-related; however, it was transmitted to a definitive host and involved in previous outbreaks. It is reported that cats and one-humped camels played a major role in the transmission of the severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS) respectively, to human.2 In 2003, SARS-CoV was the first transmitted to human in Asia and infected humans in more than 24 countries particularly in China. The outbreak extended to eight months in which 8,098 individuals were infected and the death toll was 774. Similarly, Middle East respiratory syndrome coronavirus (MERS-CoV) causes severe respiratory infections with common symptoms of cough, fever, and shortness of breath. The first case of MERS-CoV was identified in Saudi Arabia in 2012, and all cases were associated with traveling history in Arabic regions and their neighboring countries. The second outbreak of the disease appeared in 2015, in the Republic of Korea and was similarly linked with a traveling history. The cases of MERS-CoV reached 2,494 with 858 deaths throughout the world.2,3
The recent outbreak of respiratory illness in the Wuhan City of China, caused by the SARS-CoV-2, belongs to the beta-corona virus family, similar to SARS and MERS-CoV. The SARS-CoV-2 are continuously spreading throughout the world irrespective of regional borders.4 WHO declared an outbreak of COVID-19 on 31st January 2020 as an epidemic, an alarming public health issue throughout the world because the deadly virus had been reported in different countries. Later, WHO announced COVID-19 pandemic. The current situation has not been effectively controlled and the health authorities in all countries have been alerted to handle it any seriously.5,6
Table 1: Comparison of SARS, MERS and COVID-19
POSSIBLE TRANSMISSION
Most of the cases from the initial cluster have epidemiological links with a live animal market (Huanan South China Seafood Market), suggesting a possible zoonotic origin.7,8 According to a Chinese report, coronavirus-2019 had a significant link with seafood, live animal market (zoonotic source); later on they found person to person transmission after identifying cases in a family members along with transmission reported from patients to healthcare staff. The official news from China reported that person to person transmission was persistently occurring in the community of China. The transmission of COVID-19 was significantly associated with the immigration of individuals from Wuhan city. It was also reported to be spreading outside the Chinese borders. However, the definitive source of the virus remains unknown.9
Another major issue about SARS-CoV-2 is whether the individuals infected with the virus are symptomatic or not (having no symptoms in early). A child in Shenzhen identified to be infected by SARS-CoV-2 displayed no symptoms. If such asymptomatic cases increase in numbers and can spread the virus, it will be very difficult to handle such transmission and may take a longer time to control it. If this coronavirus could mutate, it will become more virulent and will spread quickly and more likely to cause disease fericiously.10,11
CLINICAL MANIFESTATIONS
The common symptoms related to the COVID-19 are fever, dyspnea, dry cough, and severe respiratory disorders. Most patients are presenting with pneumonia and severe acute respiratory diseases. Few cases have also been reported with kidney failure, heart and other comorbidity.12 In fact, respiratory failure or multiple organ dysfunction syndrome (MODS) are the two most common terminal causes of death.
GENETIC SEQUENCE OF SARS-CoV-2
The genome of SARS-CoV-2 has about 70% similarity with SARS-CoV. The close relation suggests that SARS-CoV-2 can also be expected to be bat originated. Further investigation is yet inconclusive. On 7th January 2020, the Chinese Scientists have isolated a new strain of SARS-CoV-2 and the genetic sequence was shared with different countries to develop diagnostic kits.13,14 This genetic sequence of the SARS-CoV-2 will enable rapid development of point-of-care real-time PCR diagnostic tests. It is based on full genome sequence data on the Global Initiative on Sharing All Influenza Data [GISAID] platform.14-16
DIAGNOSIS AND TREATMENT OF SARS-CoV-2
Till now, there is no particular rapid diagnostic test available except RT-PCR. Hence, diagnosis relies on patient history of traveling to Wuhan city, signs and symptoms along with computerized tomography scanning (CT scan) of the lungs. Polymerase chain reaction-based tests are used for the diagnosis and confirmation of infection. The common samples required for PCR are lower respiratory tract samples including endotracheal aspirate and sputum. Few researchers also reported that virus can be detected from feces, urine and blood specimens.17,18
There is no specific antiviral therapy (drug and/or vaccine) available for the treatment of COVID-19. Supportive treatment is provided to prevent severe complications and secondary infections. Moreover, some HIV drugs can effectively work in such patients as both SARS-CoV-2 and HIV are RNA viruses.19
PRECAUTIONARY MEASUREMENT
Chinese government actively responds to this emergency but actually situation is very panic. Despite their quick response, SARS-CoV-2 shed to other countries and threaten public health all over the world. Efficient collaboration is required to prevent further transmission.
The way to reduce the risk of having an infection is washing hands properly, not touching eyes, nose, and mouth with dirty hands, wash mouth properly and keep it moist, reduce contact with people having cold and flu, avoid the crowded areas and cover the face with mask going out in public transport.20 Traveling and trade should be lockdown temporarily throughout the globe. The development of new diagnostic kits is the demand for the detection of the virus in immunocompetent and asymptomatic patients. It is important to provide facilities to the developing countries before happening any emergency. Suspected patients should be isolated to prevent further shedding of the virus among the community.
CURRENT STATUS OF COVID-19 in the World
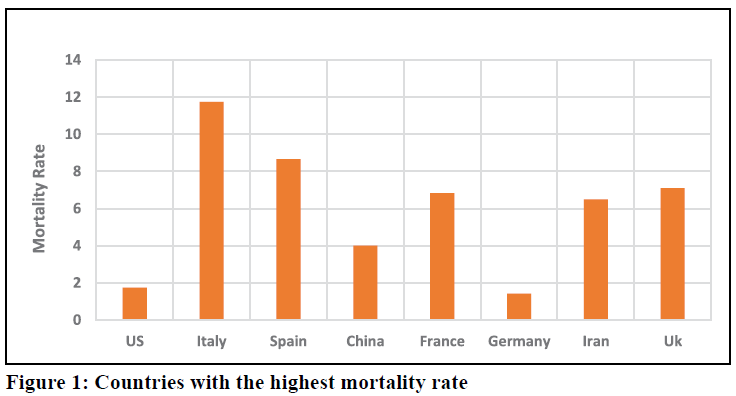
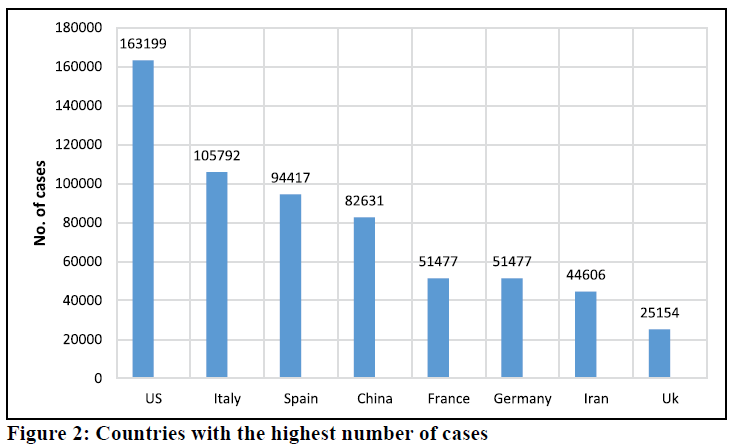
Globally, a total of 823, 6326 cases identified with 40,598 new cases in more 170 countries till 1st April 2020. The European region is more affected then the rest of the continents. About 464,212 cases reported with 30,089 deaths in European region, followed by Region of Americas in which 188,751 cases along with 3,400 causalities. The cases of Western Pacific region, Eastern Mediterranean Region, South-East Asia region and African regions are 106,422 cases (3,701 deaths), 54.281 cases (3,115 deaths), 5,175 (195 deaths) and 4,073 cases (91 deaths) respectively. Highest no. of cases reported in United State (163,199 cases), followed by Italy, Spain, China, France and Germany. However, the mortality rate is greater in Italy (11.7%), followed by Spain (8.7%), United Kingdom (7.11) and France (6.8%). As a result of traveling, an outbreak occurred in several countries especially the European regions is more affected than the rest of world.21
CURRENT STATUS OF COVID-19 IN PAKISTAN
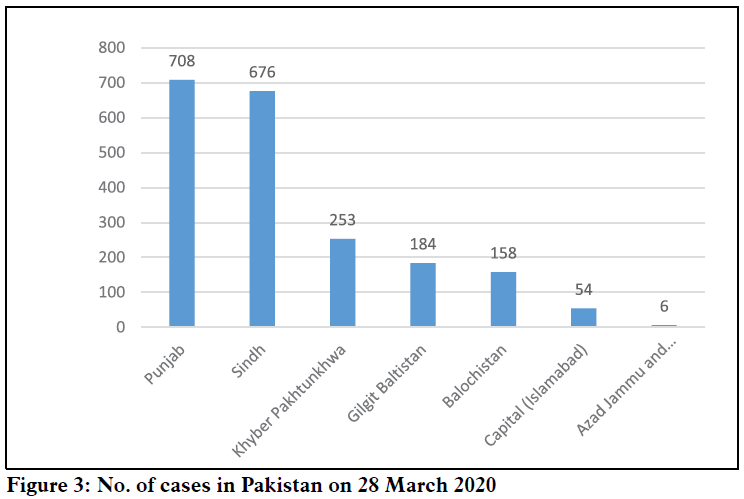
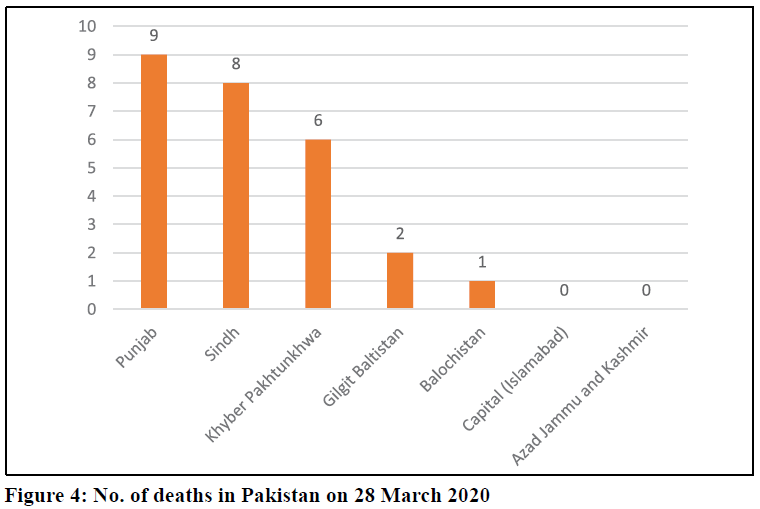
On 27 February 2020, WHO reported the first two cases of COVID-19 in Pakistan; one from the most populated and metropolitan city of Karachi and the other from the federal capital Islamabad. Both cases were called imported ones as they had recently travelled from Iran.23 It has been claimed that all cases were infected in Iran and Saudi Arabia during their pilgrimage tour to those countries, and they travelled back to Pakistan. Many pilgrims from Gilgit-Baltistan were confirmed with COVID-19 infection after arrival from Iran in the past month. Till April 4, 2020, total cases in Pakistan are 2,940 cases with 44 deaths (1.4% mortality rate). Majority of cases are reported from Punjab and Sindh, then Khyber Pakhtunkhwa and Gilgit-Baltistan as shown in figures below. Mortality rate is high in Khyber Pakhtunkhwa than the rest of the provinces.
RESPONSE OF CHINA AND REST OF THE WORLD TO PANDEMIC
An immediate investigation was done by the health commission of the Chinese government to characterize and control the outbreak. The researchers collected the epidemiological and clinical data from patients and were engaged in the development of diagnostics and treatment procedures.
The number of cases is likely to increase from time to time, in China and globally. On 21 January 2020, the WHO suggested that there was a possible sustained human-to-human transmission. Therefore, on 27th January 2020, WHO issued travel guidelines for China to avoid unnecessary traveling. China locked down many cities including the epicenter of COVID-19 (Wuhan) to contain the outbreak. Additionally, the Chinese government officially restricted and suspended all public transport. The Chinese government also took necessary measures to stop further global escalation.22 It was understood that if unprecedented actions like China were not taken by other countries, COVID-19 will not be confined within the borders of China and will become pandemic engulfing most of the countries of the world.
THREAT TO PAKISTAN
Pakistani people were comparatively at higher risk to epidemic of COVID-19 than most of the world, due to close geographical proximity and a shared border of 272 miles with China and 596 miles with Iran. More cases are plausible in the coming days due to several reasons; the healthcare system is more fragile and has no satisfactory resources to manage the condition. Secondly, hundreds of students are studying in China especially in Wuhan city, which is an epicenter of COVID-19. Hence, there is a greater probability of spread of infection in Pakistan. The threat is severe at airports and immigrants’ students/travelers coming from neighbor countries including China and Iran and other countries. A large number of pilgrims, belonging to Shia community, visit Iran during this part of the year, to pay their tribute to notables from the early period of Islam. They spend weeks to few months at there and then return back mostly via Taftan (Balochistan). It is a small town with very little civic facilities. With ever-increasing number of confirmed cases in Iran and poor control on population movement, there has been a great risk of import of the COVID-19 into Pakistan.
PREPAREDNESS AND RESPONSE OF PAKISTAN
It can be postulated that situation will be worst in few upcoming days in Pakistan. We are one of the under developed countries, therefore, Pakistani health organizations need to take all possible precautionary measures preemptively, before the emergency does strike us. Federal and provincial governments of Pakistan have taken few important steps at national and provincial level to tackle COVID-19.23
NATIONAL LEVEL
At national level, Infection and Prevention Control (IPC) training programs have been arranged in different hospitals of the country in order to train and prepare hospital staff. Quarantine centers have been arranged in different regions of countries. All the returnees and pilgrims are continuously monitor at home time to time. Rapid response teams (RRT) have been designated for tracing the contact/suspected persons with infected individuals. RRT teams were used to trace out the students returned from China, Chinese and Hong Kong workers, as well as returnees from various countries including Iran and Saudi Arabia.
The required drugs, personal protective equipment (PPE), surgical masks, ventilators, polymerase chain reaction (PCR) test kits, and viral transport medium (VTM) kits, used to carefully transport the swabs to the laboratories, have been provided to various quarantine centers, diagnostic laboratories and hospitals. All the cinemas, sports activities, wedding ceremonies and social gatherings have been completely banned throughout the country. All police, rangers and army personnel deputed on duty have been alert in order to ensure the social distancing. All institutes including schools, colleges and university are closed till 31st May 2020 in order to make the social distancing. Awareness programs have been arranged on social media, health department websites and also announcement sessions are done on loudspeakers and radio channels insides country. Fumigation process is continuously arranged for ambulances, isolation rooms, hospital centers, central jails and quarantine centers. At national level tender have been issue for further equipment, ventilators, surgical and N95 masks, healthcare workers (HCW) protection suits, PCR machine and kits. Moreover, National Disaster Management Authority (NDMA) announced hundred new vacancies for hiring of medical laboratory technologists in order to fulfill the demand of newly established virology laboratories.
PROVINCIAL LEVEL RESPONSE
PUNJAB
Provincial Disease Surveillance and Response Unit (PDSRU) arranged IPC training for Police line staff. Finance Department of Punjab approved emergency budget of Rs 7.62 billion to combat COVID-19 at provincial level. A total of 19,000 beds was arranged for quarantine. Two more Biosafety level-3 laboratories have been established on emergency basis for rapid detection and diagnosis of COVID-19. At district level all the staff are being trained to properly handle the patients, samples and dead bodies in quarantine centers and hospitals.
SINDH
Quarantine centers including the Sukkur have been designed and made functional for returnees of Iran via Taftan border. The Sindh province has been under complete lockdown for 15 days since 23rd March 2020. The N95 masks were distributed in major and vulnerable region of province. 160 ICU beds have been created in five bigger hospitals of the province to quarantine serious COVID-19 patients.
KHYBER PAKHTUNKHWA
Quarantine center for Iran returnees has been established at Dera Ismail Khan (DI Khan). Incident command and management center has been established at Polio headquarter for COVID-19. A total of 1,299 medical officers were hired on emergency based to fulfill the emergency duties during the period of pandemic. Highly trained and well-equipped screening teams with thermal detectors and PPE’s have been appointed on all entry and exit points in the districts and at border of the province. The district Abbottabad was locked down due to a death of a confirmed patient of COVID-19. Approximately 10 provincial officers have been trained for the newly merged area of province, formerly known as Federally Administered Tribal Area (FATA).
GILGIT BALTISTAN
Isolation rooms and wards have been established at different public and private hospitals of the province. The WHO staff provides support for data management at district level inside the province.
BALUCHISTAN
Field Epidemiology and Laboratory Training Programs (FELTPs) trained HCW’s at Pakistan Council of Scientific and Industrial Research (PCSIR) center, Quetta. Taftan border quarantine center was designed for returnees from Iran and provide all the necessary medicine and equipment including PPE’s, VTM kits, thermoguns and PCR kits along with mobile lab and well-equipped ambulances. Among the affected region of the province N95 masks were distributed to reduce the contact and spread of the virus.
AZAD JAMMU AND KASHMIR
Isolation wards at Chest Diseases General Hospital, New City Hospital, Combined Military Hospital and at other hospitals have been established for better management of suspected or confirmed patients of COVID-19. A 50 bed hospital has been established at Muzaffarabad and will be functional in next few weeks. A new virology laboratory has been established and started the PCR testing of SARS-CoV-2 at Abbas Institute of Medical Sciences (AIMS), Muzaffarabad.
FUTURE DIRECTIONS
WHO needs to take necessary action against COVID-19 in under-developed countries, which are prone to high morbidity and mortality from the pandemic. The occurrence of massive outbreak is expected in Pakistan due to a lack of resources and inadequate diagnostic and healthcare centers, which will be catastrophic for Pakistan. Pakistani authorities have deputed various expert teams at international airports to screen out individuals coming from neighbor countries and the rest of the world. Moreover, health authorities take necessary preventive measures and vigilance regarding the deadly disease.24 Complete cessation of all domestic as well as international flights from Pakistani airports is on the cards.
It is the responsibility of the state to take all precautionary measures for the safety of the community and public. It is required to look for the immigrants from China, Iran and the rest of the world having traveling history after December 2019. All passengers arriving in Pakistan must have a virus-free certificate, installed proper checking counters under the supervision of qualified HCW. All tertiary care centers should have isolation wards and should be ready for any type of emergency and to isolate the victims from other patients.
CONCLUSION
The origin and the mode of spread of COVID-19 among the humans are still unknown. Many factors might be involved in the emergence of SARS-CoV-2 from the previous outbreaks. Climate change, increased traveling and trade locally and internationally, the high burden of the human population and increased wildlife contact, could be the possible factors that provoked and facilitated the outbreak of COVID-19. In the past few years, greater than 20 viruses emerged and re-emerged throughout the world, in which the majority have been zoonotic viruses. This rapidly emerging COVID-19 pandemic is difficult to control in any underdeveloped country. Therefore, this alarming situation needs a coordinated response at an international level. Temporary ban on traveling and wildlife trade, special screening on ports, public training and awareness can overcome the further spread of the disease.
It is important to monitor the current situation in countries suffering with pandemic. Presently, Pakistan is at risk of COVID-19 due to large number of imported cases. Our people should be aware of its mode of transmission, symptoms, precautions, and treatment. The primary action to create awareness among the population can be undertaken through social media, elactronic media and other possible means. Secondly, the government needs to foresee and provide all basic facilities to hospitals for any emergency. Isolation rooms/wards should be established inside all basic healthcare units (BHUs), tehsil headquarter hospitals (THQ’s) districts headquarter hospitals (DHQ’s) and tertiary care hospitals to avoid transmission among HCWs and other patients. It is government responsibility to make sure the availability of N95 masks, surgical masks and sanitizers in the market at affordable prices or should be available in healthcare centers without any cost.
Acknowledgment: All the frontline fighters (healthcare workers) of Pakistan and rest of the world against the deadly COVID-19.
Funding source: No funding source.
Conflicts of interest: The authors declare no conflict of interest.
Authors’ contribution:
AM, MO - Study design, conceptualization, write up, literature review and approval of manuscript
NA, HK - Critical Review, discussion and approval of manuscript
REFERENCES
1M.Phil. Lecturer, Department of Medical Laboratory Technology, College of Medical Technology, Bacha Khan Medical College, Mardan, Pakistan.
2M.Phil, Lecturer, Department of Medical Laboratory Technology, College of Medical Technology, Bacha Khan Medical College, Mardan, Pakistan.
3M.Phil, Lecturer, Department of Medical Laboratory Technology, College of Medical Technology, Bacha Khan Medical College, Mardan, Pakistan.
4Ph.D, Assistant Professor, Department of Medical Laboratory Technology, College of Medical Technology, Bacha Khan Medical College, Mardan, Pakistan.
Correspondence: Hidayat Khan,
Lecturer, Department of Medical Laboratory Technology, College of Medical Technology, Bacha Khan Medical College, Mardan, (Pakistan)
E-mail: farhansf9@gmail.com
ABSTRACT
The current outbreak of Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) has attained the dimensions of a pandemic and World Health Organization (WHO) has declared it a global emergency and given it a name of COVID-19. It may remain asymptomatic, but usually presents as influenza-like symptoms initially. It spreads from zoonotic sources, which are still under investigation. Real Time Polymerase Chain Reaction (RT-PCR) is the only available diagnostic and confirmatory lab assay for SARS-CoV-2. There is no specific antiviral drug or vaccine against SARS-CoV-2, hence infected and suspected cases are dependent on supportive treatment along with few anti-HIV drugs. Evidence suggests that, in Pakistan, all cases have returned from Iran and Saudi Arabia after pilgrimage. The number of patients has been increasing gradually. Almost all of the neighboring countries of Pakistan are suffering from an outbreak. So, a big threat is there. Pakistani health authorities need to take critical action urgently. Moreover, it is necessary to take basic preventive measurements including hand washing, use of face masks, keeping the distance from suspected patients and avoiding unnecessary traveling to overcrowded areas. It is concluded that the developing countries might be at higher risk including Pakistan. Personnel and community-based strategy is required to avoid any serious consequences in Pakistan. We searched relevant studies and papers from Google, Google Scholar, National Institute of Health (Pakistan) and WHO by using various medical subject heading (MeSH) terms including COVID-19, SARS-CoV-2, MERS, Preventive Measurements of COVID etc. All downloaded articles were carefully read and conclusions drawn.
Key words: SARS-CoV-2; Epidemic; Pandemic; COVID-19; Pakistan
Citation: Muhammad A, Owais M, Ali N, Khan H. COVID-19 pandemic and precautionary measures in Pakistan. Anaesth pain intensive care 2020;24(1):_
DOI: https://doi.org/10.35975/apic.v24i1.
Received – 20 March 2020; Reviewed – 22 March 2020; Accepted - 27 March 2020
INTRODUCTION
Coronavirus is an enveloped single-stranded RNA virus with positive polarity. The name "corona means crown", the spikes around the surface of the Coronavirus make virus crown shape. Subtypes of coronaviruses include Human Coronavirus-229E (HCoV-229E), HKU1-CoV, HCoV-NL63, and HCoV-OC43 including in common cold disease.1 Few are human transmitted coronaviruses, whereas the majority can be identified in animals. Before a few decades, coronavirus was considered animal virus especially bat-related; however, it was transmitted to a definitive host and involved in previous outbreaks. It is reported that cats and one-humped camels played a major role in the transmission of the severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS) respectively, to human.2 In 2003, SARS-CoV was the first transmitted to human in Asia and infected humans in more than 24 countries particularly in China. The outbreak extended to eight months in which 8,098 individuals were infected and the death toll was 774. Similarly, Middle East respiratory syndrome coronavirus (MERS-CoV) causes severe respiratory infections with common symptoms of cough, fever, and shortness of breath. The first case of MERS-CoV was identified in Saudi Arabia in 2012, and all cases were associated with traveling history in Arabic regions and their neighboring countries. The second outbreak of the disease appeared in 2015, in the Republic of Korea and was similarly linked with a traveling history. The cases of MERS-CoV reached 2,494 with 858 deaths throughout the world.2,3
The recent outbreak of respiratory illness in the Wuhan City of China, caused by the SARS-CoV-2, belongs to the beta-corona virus family, similar to SARS and MERS-CoV. The SARS-CoV-2 are continuously spreading throughout the world irrespective of regional borders.4 WHO declared an outbreak of COVID-19 on 31st January 2020 as an epidemic, an alarming public health issue throughout the world because the deadly virus had been reported in different countries. Later, WHO announced COVID-19 pandemic. The current situation has not been effectively controlled and the health authorities in all countries have been alerted to handle it any seriously.5,6
Table 1: Comparison of SARS, MERS and COVID-19
| Virus | Disease | Origin | Primary source | Intermediate Source | No. of Cases | Deaths | Mortality rate |
| SARS | SARS | China | Bat | Cavet Cat | 8,098 | 774 | 0.96% |
| MERS | MERs | KSA | Bat | Camel | 2,494 | 858 | 34.4% |
| COVID-19 | COVID-19 | China | Bat | Unknown | 823,626 | 40,598 | 4.9% |
Most of the cases from the initial cluster have epidemiological links with a live animal market (Huanan South China Seafood Market), suggesting a possible zoonotic origin.7,8 According to a Chinese report, coronavirus-2019 had a significant link with seafood, live animal market (zoonotic source); later on they found person to person transmission after identifying cases in a family members along with transmission reported from patients to healthcare staff. The official news from China reported that person to person transmission was persistently occurring in the community of China. The transmission of COVID-19 was significantly associated with the immigration of individuals from Wuhan city. It was also reported to be spreading outside the Chinese borders. However, the definitive source of the virus remains unknown.9
Another major issue about SARS-CoV-2 is whether the individuals infected with the virus are symptomatic or not (having no symptoms in early). A child in Shenzhen identified to be infected by SARS-CoV-2 displayed no symptoms. If such asymptomatic cases increase in numbers and can spread the virus, it will be very difficult to handle such transmission and may take a longer time to control it. If this coronavirus could mutate, it will become more virulent and will spread quickly and more likely to cause disease fericiously.10,11
CLINICAL MANIFESTATIONS
The common symptoms related to the COVID-19 are fever, dyspnea, dry cough, and severe respiratory disorders. Most patients are presenting with pneumonia and severe acute respiratory diseases. Few cases have also been reported with kidney failure, heart and other comorbidity.12 In fact, respiratory failure or multiple organ dysfunction syndrome (MODS) are the two most common terminal causes of death.
GENETIC SEQUENCE OF SARS-CoV-2
The genome of SARS-CoV-2 has about 70% similarity with SARS-CoV. The close relation suggests that SARS-CoV-2 can also be expected to be bat originated. Further investigation is yet inconclusive. On 7th January 2020, the Chinese Scientists have isolated a new strain of SARS-CoV-2 and the genetic sequence was shared with different countries to develop diagnostic kits.13,14 This genetic sequence of the SARS-CoV-2 will enable rapid development of point-of-care real-time PCR diagnostic tests. It is based on full genome sequence data on the Global Initiative on Sharing All Influenza Data [GISAID] platform.14-16
DIAGNOSIS AND TREATMENT OF SARS-CoV-2
Till now, there is no particular rapid diagnostic test available except RT-PCR. Hence, diagnosis relies on patient history of traveling to Wuhan city, signs and symptoms along with computerized tomography scanning (CT scan) of the lungs. Polymerase chain reaction-based tests are used for the diagnosis and confirmation of infection. The common samples required for PCR are lower respiratory tract samples including endotracheal aspirate and sputum. Few researchers also reported that virus can be detected from feces, urine and blood specimens.17,18
There is no specific antiviral therapy (drug and/or vaccine) available for the treatment of COVID-19. Supportive treatment is provided to prevent severe complications and secondary infections. Moreover, some HIV drugs can effectively work in such patients as both SARS-CoV-2 and HIV are RNA viruses.19
PRECAUTIONARY MEASUREMENT
Chinese government actively responds to this emergency but actually situation is very panic. Despite their quick response, SARS-CoV-2 shed to other countries and threaten public health all over the world. Efficient collaboration is required to prevent further transmission.
The way to reduce the risk of having an infection is washing hands properly, not touching eyes, nose, and mouth with dirty hands, wash mouth properly and keep it moist, reduce contact with people having cold and flu, avoid the crowded areas and cover the face with mask going out in public transport.20 Traveling and trade should be lockdown temporarily throughout the globe. The development of new diagnostic kits is the demand for the detection of the virus in immunocompetent and asymptomatic patients. It is important to provide facilities to the developing countries before happening any emergency. Suspected patients should be isolated to prevent further shedding of the virus among the community.
CURRENT STATUS OF COVID-19 in the World
Globally, a total of 823, 6326 cases identified with 40,598 new cases in more 170 countries till 1st April 2020. The European region is more affected then the rest of the continents. About 464,212 cases reported with 30,089 deaths in European region, followed by Region of Americas in which 188,751 cases along with 3,400 causalities. The cases of Western Pacific region, Eastern Mediterranean Region, South-East Asia region and African regions are 106,422 cases (3,701 deaths), 54.281 cases (3,115 deaths), 5,175 (195 deaths) and 4,073 cases (91 deaths) respectively. Highest no. of cases reported in United State (163,199 cases), followed by Italy, Spain, China, France and Germany. However, the mortality rate is greater in Italy (11.7%), followed by Spain (8.7%), United Kingdom (7.11) and France (6.8%). As a result of traveling, an outbreak occurred in several countries especially the European regions is more affected than the rest of world.21
CURRENT STATUS OF COVID-19 IN PAKISTAN
On 27 February 2020, WHO reported the first two cases of COVID-19 in Pakistan; one from the most populated and metropolitan city of Karachi and the other from the federal capital Islamabad. Both cases were called imported ones as they had recently travelled from Iran.23 It has been claimed that all cases were infected in Iran and Saudi Arabia during their pilgrimage tour to those countries, and they travelled back to Pakistan. Many pilgrims from Gilgit-Baltistan were confirmed with COVID-19 infection after arrival from Iran in the past month. Till April 4, 2020, total cases in Pakistan are 2,940 cases with 44 deaths (1.4% mortality rate). Majority of cases are reported from Punjab and Sindh, then Khyber Pakhtunkhwa and Gilgit-Baltistan as shown in figures below. Mortality rate is high in Khyber Pakhtunkhwa than the rest of the provinces.
RESPONSE OF CHINA AND REST OF THE WORLD TO PANDEMIC
An immediate investigation was done by the health commission of the Chinese government to characterize and control the outbreak. The researchers collected the epidemiological and clinical data from patients and were engaged in the development of diagnostics and treatment procedures.
The number of cases is likely to increase from time to time, in China and globally. On 21 January 2020, the WHO suggested that there was a possible sustained human-to-human transmission. Therefore, on 27th January 2020, WHO issued travel guidelines for China to avoid unnecessary traveling. China locked down many cities including the epicenter of COVID-19 (Wuhan) to contain the outbreak. Additionally, the Chinese government officially restricted and suspended all public transport. The Chinese government also took necessary measures to stop further global escalation.22 It was understood that if unprecedented actions like China were not taken by other countries, COVID-19 will not be confined within the borders of China and will become pandemic engulfing most of the countries of the world.
THREAT TO PAKISTAN
Pakistani people were comparatively at higher risk to epidemic of COVID-19 than most of the world, due to close geographical proximity and a shared border of 272 miles with China and 596 miles with Iran. More cases are plausible in the coming days due to several reasons; the healthcare system is more fragile and has no satisfactory resources to manage the condition. Secondly, hundreds of students are studying in China especially in Wuhan city, which is an epicenter of COVID-19. Hence, there is a greater probability of spread of infection in Pakistan. The threat is severe at airports and immigrants’ students/travelers coming from neighbor countries including China and Iran and other countries. A large number of pilgrims, belonging to Shia community, visit Iran during this part of the year, to pay their tribute to notables from the early period of Islam. They spend weeks to few months at there and then return back mostly via Taftan (Balochistan). It is a small town with very little civic facilities. With ever-increasing number of confirmed cases in Iran and poor control on population movement, there has been a great risk of import of the COVID-19 into Pakistan.
PREPAREDNESS AND RESPONSE OF PAKISTAN
It can be postulated that situation will be worst in few upcoming days in Pakistan. We are one of the under developed countries, therefore, Pakistani health organizations need to take all possible precautionary measures preemptively, before the emergency does strike us. Federal and provincial governments of Pakistan have taken few important steps at national and provincial level to tackle COVID-19.23
NATIONAL LEVEL
At national level, Infection and Prevention Control (IPC) training programs have been arranged in different hospitals of the country in order to train and prepare hospital staff. Quarantine centers have been arranged in different regions of countries. All the returnees and pilgrims are continuously monitor at home time to time. Rapid response teams (RRT) have been designated for tracing the contact/suspected persons with infected individuals. RRT teams were used to trace out the students returned from China, Chinese and Hong Kong workers, as well as returnees from various countries including Iran and Saudi Arabia.
The required drugs, personal protective equipment (PPE), surgical masks, ventilators, polymerase chain reaction (PCR) test kits, and viral transport medium (VTM) kits, used to carefully transport the swabs to the laboratories, have been provided to various quarantine centers, diagnostic laboratories and hospitals. All the cinemas, sports activities, wedding ceremonies and social gatherings have been completely banned throughout the country. All police, rangers and army personnel deputed on duty have been alert in order to ensure the social distancing. All institutes including schools, colleges and university are closed till 31st May 2020 in order to make the social distancing. Awareness programs have been arranged on social media, health department websites and also announcement sessions are done on loudspeakers and radio channels insides country. Fumigation process is continuously arranged for ambulances, isolation rooms, hospital centers, central jails and quarantine centers. At national level tender have been issue for further equipment, ventilators, surgical and N95 masks, healthcare workers (HCW) protection suits, PCR machine and kits. Moreover, National Disaster Management Authority (NDMA) announced hundred new vacancies for hiring of medical laboratory technologists in order to fulfill the demand of newly established virology laboratories.
PROVINCIAL LEVEL RESPONSE
PUNJAB
Provincial Disease Surveillance and Response Unit (PDSRU) arranged IPC training for Police line staff. Finance Department of Punjab approved emergency budget of Rs 7.62 billion to combat COVID-19 at provincial level. A total of 19,000 beds was arranged for quarantine. Two more Biosafety level-3 laboratories have been established on emergency basis for rapid detection and diagnosis of COVID-19. At district level all the staff are being trained to properly handle the patients, samples and dead bodies in quarantine centers and hospitals.
SINDH
Quarantine centers including the Sukkur have been designed and made functional for returnees of Iran via Taftan border. The Sindh province has been under complete lockdown for 15 days since 23rd March 2020. The N95 masks were distributed in major and vulnerable region of province. 160 ICU beds have been created in five bigger hospitals of the province to quarantine serious COVID-19 patients.
KHYBER PAKHTUNKHWA
Quarantine center for Iran returnees has been established at Dera Ismail Khan (DI Khan). Incident command and management center has been established at Polio headquarter for COVID-19. A total of 1,299 medical officers were hired on emergency based to fulfill the emergency duties during the period of pandemic. Highly trained and well-equipped screening teams with thermal detectors and PPE’s have been appointed on all entry and exit points in the districts and at border of the province. The district Abbottabad was locked down due to a death of a confirmed patient of COVID-19. Approximately 10 provincial officers have been trained for the newly merged area of province, formerly known as Federally Administered Tribal Area (FATA).
GILGIT BALTISTAN
Isolation rooms and wards have been established at different public and private hospitals of the province. The WHO staff provides support for data management at district level inside the province.
BALUCHISTAN
Field Epidemiology and Laboratory Training Programs (FELTPs) trained HCW’s at Pakistan Council of Scientific and Industrial Research (PCSIR) center, Quetta. Taftan border quarantine center was designed for returnees from Iran and provide all the necessary medicine and equipment including PPE’s, VTM kits, thermoguns and PCR kits along with mobile lab and well-equipped ambulances. Among the affected region of the province N95 masks were distributed to reduce the contact and spread of the virus.
AZAD JAMMU AND KASHMIR
Isolation wards at Chest Diseases General Hospital, New City Hospital, Combined Military Hospital and at other hospitals have been established for better management of suspected or confirmed patients of COVID-19. A 50 bed hospital has been established at Muzaffarabad and will be functional in next few weeks. A new virology laboratory has been established and started the PCR testing of SARS-CoV-2 at Abbas Institute of Medical Sciences (AIMS), Muzaffarabad.
FUTURE DIRECTIONS
WHO needs to take necessary action against COVID-19 in under-developed countries, which are prone to high morbidity and mortality from the pandemic. The occurrence of massive outbreak is expected in Pakistan due to a lack of resources and inadequate diagnostic and healthcare centers, which will be catastrophic for Pakistan. Pakistani authorities have deputed various expert teams at international airports to screen out individuals coming from neighbor countries and the rest of the world. Moreover, health authorities take necessary preventive measures and vigilance regarding the deadly disease.24 Complete cessation of all domestic as well as international flights from Pakistani airports is on the cards.
It is the responsibility of the state to take all precautionary measures for the safety of the community and public. It is required to look for the immigrants from China, Iran and the rest of the world having traveling history after December 2019. All passengers arriving in Pakistan must have a virus-free certificate, installed proper checking counters under the supervision of qualified HCW. All tertiary care centers should have isolation wards and should be ready for any type of emergency and to isolate the victims from other patients.
CONCLUSION
The origin and the mode of spread of COVID-19 among the humans are still unknown. Many factors might be involved in the emergence of SARS-CoV-2 from the previous outbreaks. Climate change, increased traveling and trade locally and internationally, the high burden of the human population and increased wildlife contact, could be the possible factors that provoked and facilitated the outbreak of COVID-19. In the past few years, greater than 20 viruses emerged and re-emerged throughout the world, in which the majority have been zoonotic viruses. This rapidly emerging COVID-19 pandemic is difficult to control in any underdeveloped country. Therefore, this alarming situation needs a coordinated response at an international level. Temporary ban on traveling and wildlife trade, special screening on ports, public training and awareness can overcome the further spread of the disease.
It is important to monitor the current situation in countries suffering with pandemic. Presently, Pakistan is at risk of COVID-19 due to large number of imported cases. Our people should be aware of its mode of transmission, symptoms, precautions, and treatment. The primary action to create awareness among the population can be undertaken through social media, elactronic media and other possible means. Secondly, the government needs to foresee and provide all basic facilities to hospitals for any emergency. Isolation rooms/wards should be established inside all basic healthcare units (BHUs), tehsil headquarter hospitals (THQ’s) districts headquarter hospitals (DHQ’s) and tertiary care hospitals to avoid transmission among HCWs and other patients. It is government responsibility to make sure the availability of N95 masks, surgical masks and sanitizers in the market at affordable prices or should be available in healthcare centers without any cost.
Acknowledgment: All the frontline fighters (healthcare workers) of Pakistan and rest of the world against the deadly COVID-19.
Funding source: No funding source.
Conflicts of interest: The authors declare no conflict of interest.
Authors’ contribution:
AM, MO - Study design, conceptualization, write up, literature review and approval of manuscript
NA, HK - Critical Review, discussion and approval of manuscript
REFERENCES
- Killerby ME, Biggs HM, Haynes A, Dahl RM, Mustaquim D, Gerber SI, et al. Human coronavirus circulation in the United States 2014–2017. J Clin Virol. 2018 Apr 1;101:52–6. [PubMed] DOI: 10.1016/j.jcv.2018.01.019
- Swerdlow DL, Finelli L. Preparation for Possible Sustained Transmission of 2019 Novel Coronavirus. JAMA. 2020 Feb 11. [PubMed] DOI: 10.1001/jama.2020.1960
- Killerby ME, Biggs HM, Midgley CM, Gerber SI, Watson JT. Middle east respiratory syndrome coronavirus transmission. Emerg Infect Dis. 2020 Fe;26(2):191–8. [PubMed] DOI: 10.3201/eid2602.190697
- Novel Coronavirus (2019-nCoV) Situation report-5, 25 January 2020. Geneva, Switzerland. Internet. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports [Accessed 10th March 2020].
- Novel Coronavirus (2019-nCoV) Situation report-11, 31st January 2020. Geneva, Switzerland, 2020. WHO. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports [Accessed 10th March 2020].
- 2019 Novel Coronavirus (2019-nCoV) Situation Summary | CDC. Available from: https://www.cdc.gov/coronavirus/2019-ncov/summary.html [Accessed 10th March 2020].
- Cyranoski D. Mystery deepens over animal source of coronavirus. Nature. Available from: http://www.nature.com/articles/d41586-020-00548-w [Accessed 10th March 2020].
- Transmission of Coronavirus Disease 2019 (COVID-19) | CDC. Available from: https://www.cdc.gov/coronavirus/2019-ncov/about/transmission.html [Accessed 10th March 2020].
- People’s Republic of China – Updates on Immigration Policy during Coronavirus Epidemic. KPMG Glob. Available from: https://home.kpmg/xx/en/home/insights/2020/02/flash-alert-2020-026.html [Accessed 10th March 2020].
- Lewis D. Coronavirus outbreak: what’s next? Nature. 2020 Feb;578(7793):15-6. [PubMed] DOI: 10.1038/d41586-020-00236-9
- Novel Coronavirus (2019-nCoV) Situation report-1, January 2020. Geneva, Switzerland. WHO. Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200121-sitrep-1-2019-ncov.pdf?sfvrsn=20a99c10_4 [Accessed 10th March 2020].
- Ulu Kılıç A. New threat: 2019 Novel Coronavirus Infection and Infection Control Perspective in Turkey. North Clin Istanbul. Available from: http://www.kuzeyklinikleri.com/jvi.aspx?un=NCI-38159 [Accessed 10th March 2020].
- WHO Novel Coronavirus (2019-nCoV) Situation report-7, 27th January 2020. Geneva, Switzerland, 2020. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports [Accessed 10th March 2020].
- Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 2020 Feb 20;382(8):727-33. [PubMed] DOI: 10.1056/NEJMoa2001017
- W.H.O Novel Coronavirus (2019-nCoV) Situation report-19, 8 February 2020. Geneva, Switzerland, 2020. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports [Accessed 10th March 2020].
- Denise Grady. As Coronavirus Explodes in China, Countries Struggle to Control Its Spread. The New York Times, Published Jan. 30, 2020. Available at https://www.nytimes.com/2020/01/29/health/china-coronavirus-outbreak.html [cited 2020 Mar 10]
- Wang M, Cao R, Zhang L, Yang X, Liu J, Xu M, et al. Remdesivir and chloroquine effectively inhibit the recently emerged novel coronavirus (2019-nCoV) in vitro. Cell Res. 2020 Mar;30(3):269-71. [PubMed] DOI: 10.1038/s41422-020-0282-0
- Holshue ML, DeBolt C, Lindquist S, Lofy KH, Wiesman J, Bruce H, et al. First Case of 2019 Novel Coronavirus in the United States. N Engl J Med. 2020 Mar 5;382(10):929-36. [PubMed] DOI: 10.1056/NEJMoa2001191
- Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA. 2020;323(11):1061–9. [PubMed] DOI: 10.1001/jama.2020.1585
- Al-Tawfiq JA, Memish ZA. Infection control measures for the prevention of MERS coronavirus transmission in healthcare settings. Vol. 14, Expert Review of Anti-Infective Therapy. Taylor and Francis Ltd; 2016. p. 281–3.
- Novel Coronavirus (2019-nCoV) Situation report-72, 1st April 2020. Geneva, Switzerland, 2020. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports [Accessed 10th March 2020].
- Jin YH, Cai L, Cheng ZS, Cheng H, Deng T, Fan YP, et al. A rapid advice guideline for the diagnosis and treatment of 2019 novel coronavirus (2019-nCoV) infected pneumonia (standard version). Mil Med Res. 2020 Feb 6;7(1):4. [PubMed] DOI: 10.1186/s40779-020-0233-6
- Ministry of National Health Services, Regulations and Coordination and Field Epidemiology and Disease Surveillance Division (FEDSD), National Institute of Health (NIH), Islamabad. Daily Situation Report – Pakistan COVID-19. April 01, 2020. Available from: https://www.nih.org.pk/wp-content/uploads/2020/04/COVID-19-Daily-Updated-SitRep-01-April-2020.pdf
- Health Alert - U. S. Embassy Islamabad, Pakistan | U.S. Embassy & Consulates in Pakistan. WHO. Available from: https://pk.usembassy.gov/health-alert-u-s-embassy-islamabad-pakistan/ [Accessed 10th March 2020].